
(11-6-09)图1")
(11-6-09)图2")
(11-6-09)图3")
(11-6-09)图4")






| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
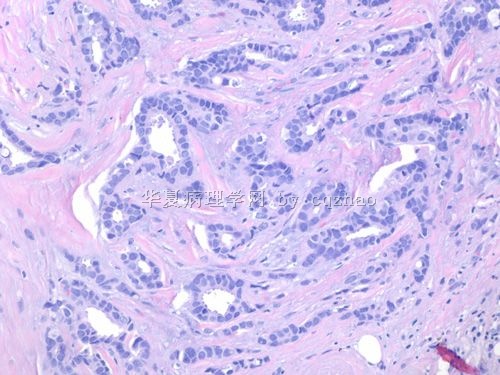
- B2280小叶癌with focal 小管structure(cqz-28)(11-6-09)
(11-6-09)图1") 图1
图1(11-6-09)图2") 图2
图2(11-6-09)图3") 图3
图3(11-6-09)图4") 图4
图4
| 姓 名: | ××× | 性别: | 年龄: | ||
| 标本名称: | |||||
| 简要病史: | |||||
| 肉眼检查: | |||||
50 岁妇女乳腺肿瘤2.5cm
. Fig 1-4. most areas of the tumor.
标签:乳腺浸润性小叶癌 伴小管结构
-
本帖最后由 于 2009-12-16 11:07:00 编辑
相关帖子
- • 女性/45岁 右侧乳腺肿块 诊断?
- • 左乳肿块,新加免疫组化
- • 乳癌?求助
- • 乳腺肿瘤
- • 够小叶癌吗?
- • 女 48岁 左侧乳腺肿块10余天
- • 女性 60岁乳腺肿块 乳腺癌分型
- • 乳腺穿刺
- • 右乳肿块
- • 右乳腺肿块穿刺活检,新加手术后图片
×参考诊断
-
本帖最后由 于 2009-11-18 20:54:00 编辑
2008-04-23 abin医师对浸润性小叶癌做了非常详尽的组织学和细胞学总结, 使我受益非浅。我把它储存在收藏夹量,以便温故知新。
更是敬佩Dr. Chao 乳腺病理诊断的丰富经验和非常感激对国内病理医师的仔细讲解和示教。
对本病例的诊断提出一些问题主要是感到作为一名高年病理医师有责任去帮助求知欲如此高的青年病理医师,去提高他们的诊断思维和拓展他们的知识面。
我个人认为此例就HE形态诊断为混合性浸润性小管小叶癌(Mixed tubulolobular carcinoma)更妥当,是非典型浸润性小叶癌的一种变型(variant)。
请注意 1)典型的小叶癌细胞可以形成微小管-Microtubule(请查阅参考文献中图Fig 9.67)。
2)浸润性小叶癌中可存在小管癌成分(tubular carcinoma), 应诊断为混合性浸润性小管小叶癌(Mixed carcinoma)。
3)混合性癌还包括:浸润性小叶癌 +原位和/或浸润性导管癌( ductal carcinoma)等多种组合。
4)少数浸润性癌在形态学上可具有浸润性导管癌和小叶癌的双重特征或中间特征。因为,形态学表现为浸润性导管癌,而细胞遗传学却具有浸润性小叶癌的分子特点。
参考文献:Diagnostic Surgical Pathology, 5th edition, 2010, p322-323.

- xljin8
| 以下是引用xljin8在2009-11-18 6:27:00的发言: 2008-04-23 abin医师对浸润性小叶癌做了非常详尽的组织学和细胞学总结, 使我受益非浅。我把它储存在收藏夹量,以便温故知新。 更是敬佩Dr. Chao 乳腺病理诊断的丰富经验和非常感激对国内病理医师的仔细讲解和示教。 |
Now what is your diagnosis for the main tumor?
1. Tubulobular ca ?
2. Mixted lobular and tubular ca?
3. Lobular ca?
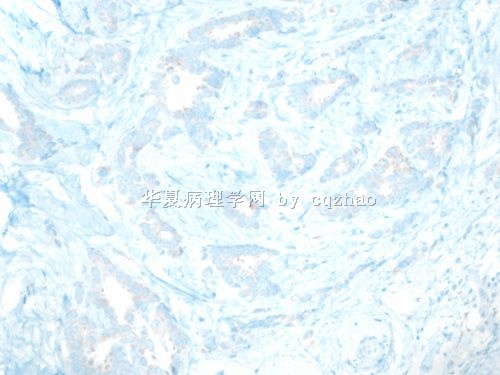
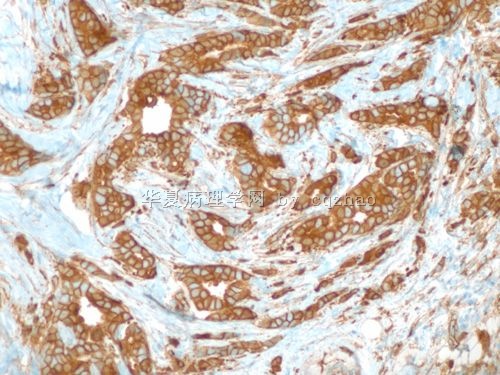
4. Is E-cadherin positive or negative in tubulobular ca (people called)?
5. Is tubulobular ca in the WHO calssification of breast ca?
6. How many cases of tubulobular ca did you see in your clinical practice?
-
尊敬的Dr. Chao, 您好!
“小管小叶”( tubulolobular ) 这一术语由Fisher等1977 年首先运用耒描述23 例在形态学上具有典型的小管癌和浸润性小叶癌二种成分的浸润性乳腺癌 (Tubulolobular invasive breast cancer: a variant of lobular invasive cancer. Hum Pathol. 1977;8:679-683)。
对于这种发生率不高的乳腺低度恶性浸润性癌的大组病例研究非常少。尽管在Tavassoli 主编的WHO 2003年乳腺肿瘤分类中尚未将其列入,但是,在Tavassoli 主编的AFIP 2009年第4版乳腺肿瘤第9章-低度恶性癌中已有小管小叶癌(tubulolobular carcinoma, TLC)。
近年对“小管小叶癌”的免疫表型研究结果TLC是导管表型“ductal phenotype”(Nicole N, et al. The ductal phenotype expression of the E-cadherin/catenin complex in tubulolobular carcinoma of the breast: an immunohistochemical and clinicopathological study. Modern pathology 2007;130-138)。
Eusebi等报道小叶癌病例中约30%有小管癌成分(Tubular carcinoma: a variant of secretory breast carcinoma. Histopathol. 1979;3:407-419), 但是对于这些浸润性小叶癌病例中的“小管癌”结构的免疫表型至今并没有进一步的研究。
我对1980年Linell等提出”小管癌可能是最早期的浸润性乳腺癌的推测和乳腺干细胞学说很感兴趣。看了您提供的病例,想请教您浸润性小叶癌与伴随小管癌样结构的关系。究竟是偶然现象? 还是存在内在联系?
从您又提供的Area-4 区E-cadherin 和 P120 标记结果支持具小叶癌免疫表型的"小管癌"成分。因此, 是否可诊断为:浸润性小叶癌伴有局灶小管癌样形态( Invasive lobular carcinoma with foci of tubular carcinoma-like pattern)。这样也许能够避免初学者误认为是真正意义上的“小叶小管癌”。
我是看了你提供的病例, 才注意到浸润性小叶癌中的“小管癌样结构”, 对TLC并无经验。因此, 感谢您提供这样好的病例, 让我学习、思考和进步。
- xljin8
| 以下是引用笃行者在2009-11-7 22:08:00的发言:
对于Dr. zhao提出的问题我个人的看法是: fig 1~4是浸润性小叶癌的图像。 area 2 如果单独看,我认为是低级别导管原位癌,也有可能是小叶癌,需免疫组化鉴别。 area 3 是低级别导管原位癌伴有浸润性小叶癌 area 4 是小管癌的图像,如果这种结构所占比例较少,则可以忽略不计,如果大于50%可以诊断浸润性小管小叶癌,是混合性小叶癌的一种。也有人认为是一种管状小叶癌。 不知是否正确,期待Dr. zhao的讲解。 |
- 轻松工作,快乐生活
| 以下是引用xljin8在2009-11-22 9:16:00的发言: 尊敬的Dr. Chao, 您好! “小管小叶”( tubulolobular ) 这一术语由Fisher等1977 年首先运用耒描述23 例在形态学上具有典型的小管癌和浸润性小叶癌二种成分的浸润性乳腺癌 (Tubulolobular invasive breast cancer: a variant of lobular invasive cancer. Hum Pathol. 1977;8:679-683)。对于这种发生率不高的乳腺低度恶性浸润性癌的大组病例研究非常少。尽管在Tavassoli 主编的WHO 2003年乳腺肿瘤分类中尚未将其列入,但是,在Tavassoli 主编的AFIP 2009年第4版乳腺肿瘤第9章-低度恶性癌中已有小管小叶癌(tubulolobular carcinoma, TLC)。近年对“小管小叶癌”的免疫表型研究结果TLC是导管表型“ductal phenotype”(Nicole N, et al. The ductal phenotype expression of the E-cadherin/catenin complex in tubulolobular carcinoma of the breast: an immunohistochemical and clinicopathological study. Modern pathology 2007;130-138)。 Eusebi等报道小叶癌病例中约30%有小管癌成分(Tubular carcinoma: a variant of secretory breast carcinoma. Histopathol. 1979;3:407-419), 但是对于这些浸润性小叶癌病例中的“小管癌”结构的免疫表型至今并没有进一步的研究。我对1980年Linell等提出”小管癌可能是最早期的浸润性乳腺癌的推测和乳腺干细胞学说很感兴趣。看了您提供的病例,想请教您浸润性小叶癌与伴随小管癌样结构的关系。究竟是偶然现象? 还是存在内在联系? 从您又提供的Area-4 区E-cadherin 和 P120 标记结果支持具小叶癌免疫表型的"小管癌"成分。因此, 是否可诊断为:浸润性小叶癌伴有局灶小管癌样形态( Invasive lobular carcinoma with foci of tubular carcinoma-like pattern)。这样也许能够避免初学者误认为是真正意义上的“小叶小管癌”。我是看了你提供的病例, 才注意到浸润性小叶癌中的“小管癌样结构”, 对TLC并无经验。因此, 感谢您提供这样好的病例, 让我学习、思考和进步。 |

There are two ways to determine the nature of the tumors, ductal vs lobular in some cases. Some people think they should be decided based on the cytomorphology and others think they should be decided based on E-cadhere stains. This is why some people including Dr. Schnit though some lobular ca can be E-Cadherin positive.
I favor they should be dicided by IHC. IHC is more objective than morphology only.
For my case I just call invasive lobular ca and I did not mention the focal 伴随小管癌样结构. Clinically it is no difference. I do not want to make the clinicians confused. Many invasive ductal ca with lobular growth pattern. We just call them as invasive ductal ca and never mention them with invasive ductal ca with lobular growth pattern.
The term of tubulolobular carcinoma is not widely accepted. If we read the original relatied papers carefully we will notice that all cases of tubulobular ca are E-Cadherin positive. So I think tubulolobular ca is just a varaint of ductal ca and no relation to lobular ca.
-
panyl10055 离线

- 帖子:258
- 粉蓝豆:867
- 经验:1331
- 注册时间:2008-08-12
- 加关注 | 发消息











