
图1")
图2")
图3")
图4")
图5")
图6")
图7")







| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- B1301Uterine high grade malignant tumor with divergent differentiation (cqz3)
图1") 图1
图1图2") 图2
图2图3") 图3
图3图4") 图4
图4图5") 图5
图5图6") 图6
图6图7") 图7
图7
| 姓 名: | ××× | 性别: | 年龄: | ||
| 标本名称: | |||||
| 简要病史: | |||||
| 肉眼检查: | |||||
Share a case of this week.
Old lady with atrophic endometrium showing tumor mass in the surface of cystic atrophic endometrium (first figure)
F1 20x
F2 100x
F3 200x
F4-5 400x
F6 200x
F7 400x
F6 and 7 showing focal glandular lesion mixed with other solid lesion.
Your dx or differential dx
标签:子宫 高级别肿瘤 异源性分化
-
本帖最后由 于 2009-02-25 09:51:00 编辑
相关帖子
- • 来一例简单罕见的(有诊断)
- • 是肉瘤吗?
- • 子宫内膜,复杂性增生?癌?(有大体结果了)
- • 子宫肿物(透明细胞平滑肌瘤?)
- • 子宫肌壁间肿物
- • 子宫腔内占位。
- • 子宫肿瘤
- • 子宫肌层浸润性癌
- • 8 个子宫上皮肿瘤病例-扫描图片
- • 子宫平滑肌肿瘤?间质肉瘤?
×参考诊断
高级别肿瘤伴异源性分化
-
alading1999 离线

- 帖子:63
- 粉蓝豆:31
- 经验:562
- 注册时间:2009-01-17
- 加关注 | 发消息
-
wangdingding 离线
- 帖子:1474
- 粉蓝豆:98
- 经验:6042
- 注册时间:2006-10-19
- 加关注 | 发消息
谢谢Dr.cqzhao!
Dr.cqzhao在41楼提供了一篇有价值的参考文献,大意是:一部分腺泡状横纹肌肉瘤中存在异常表达上皮性标记物和神经内分泌标记物的情况,单独表达其中一种标记物时还不一定证明确实存在上皮性或神经内分泌分化,但是两种标记物同时表达特别是chromogranin阳性时,提示确实存在存在上皮性和/或神经内分泌分化。因此,在原始小圆细胞肿瘤的诊断中,需要使用一组抗体包括desmin, myogenin/MyoD1,以及遗传学研究。
Dr.cqzhao在41楼说“最初我考虑这一例为伴间质样表现的癌。最后它成了复杂的MMMT病例。这例对普通病理医生(大外科病理医生)可能较困难。
OK,我已经完成了2008成的这一部分。祝愿大家拥有美妙的2009!”
__abin译

华夏病理/粉蓝医疗
为基层医院病理科提供全面解决方案,
努力让人人享有便捷准确可靠的病理诊断服务。
-
本帖最后由 于 2008-12-30 12:48:00 编辑
In the begining I thought it is a carcinoma with stromal like appearance. Finally it turned out to be a complicated MMMT case. This case is difficult for general pathologists.
OK, I finish my part in 2008. Wish all of you have a wouderful 2009.
-
Texas Children's Hospital and Baylor College of Medicine, Houston, TX, USA.
-
Alveolar rhabdomyosarcoma may be extremely difficult to distinguish from other primitive round cell neoplasms without ancillary immunohistochemistry and/or genetic study. Particularly in adults and in the head and neck locations, the differential diagnosis of alveolar rhabdomyosarcoma includes small cell carcinoma and neuroepithelial tumors, such as esthesioneuroblastoma. We have recently seen cases of genetically confirmed alveolar rhabdomyosarcoma, which were misdiagnosed owing to expression of cytokeratins and neuroendocrine markers. We studied a large group of well-characterized alveolar rhabdomyosarcomas for expression of such markers. Forty-four alveolar rhabdomyosarcomas (18 genetically confirmed) were retrieved from our archives and immunostained for wide-spectrum cytokeratin (OSCAR), low molecular weight cytokeratin (Cam5.2), synaptophysin, chromogranin A, and CD56 using commercially available antibodies. Cases were scored as 'negative', 'rare' (<5% positive cells), '1+' (5-25%), '2+' (26-50%) and '3+' (>51%). The tumors occurred in 23 males and 21 females at a mean age of 18 years (range, <1-64 years), and involved many sites. Fifty percent of cases (22 of 44) expressed wide-spectrum cytokeratin, and scored almost equally as rare, 1+, and 2+, but rarely 3+. Cam5.2 was positive in 52% (14 of 27). Forty-three percent of cases (16 of 37) expressed at least one of the specific neuroendocrine markers, 32% (12 of 37) expressed synaptophysin, 22% (eight of 36) expressed chromogranin A, and 11% expressed both. Expression of synaptophysin and chromogranin A was typically confined to rare cells but could be more widespread. Thirty-two percent of cases (12 of 37) expressed the wide-spectrum cytokeratin and at least one of the neuroendocrine markers, and 8% (three of 36) expressed cytokeratin and both neuroendocrine markers. CD56 expression was nearly ubiquitous. Aberrant expression of epithelial and neuroendocrine markers is relatively common in alveolar rhabdomyosarcoma, occurring in 30-40% of cases. These findings have significant implications for the diagnosis of alveolar rhabdomyosarcoma, particularly in adults and in the head and neck locations. Although expression of cytokeratin and/or synaptophysin alone does not necessarily indicate epithelial or neuroendocrine differentiation, coexpression of cytokeratin and neuroendocrine markers, and in particular the presence of chromogranin expression, suggest true epithelial and/or neuroendocrine differentiation in a subset of alveolar rhabdomyosarcomas. CD56 is not a specific neuroendocrine marker, and should not be used in the absence of synaptophysin/chromogranin. These findings emphasize the need to employ a panel of markers, to include desmin, myogenin/MyoD1, and genetic study in the diagnosis of primitive round cell neoplasms in all age groups and in all locations.
Useful reference if you are interested in this area.
Mod Pathol. 2008 Jul;21(7):795-806. Epub 2008 May 16.
Aberrant expression of epithelial and neuroendocrine markers in alveolar rhabdomyosarcoma: a potentially serious diagnostic pitfall.
Bahrami A, Gown AM, Baird GS, Hicks MJ, Folpe AL.
-
本帖最后由 于 2008-12-30 19:42:00 编辑
| 以下是引用abin在2008-12-23 23:33:00的发言: 这个区域的免疫组化结果判读: 上皮标记Cam5.2阳性,肌源性标记myogenin、desmin和myoglubin阳性,神经内分泌标记chrom和synaptophysin阳性,vimentin散在阳性。 考虑癌肉瘤(低分化子宫内膜样腺癌伴神经内分泌特征,混杂或合并肌源性肉瘤成分)。 HE还真没看出肌源性肉瘤分化。 |
I essentially agree with Abin's analysis.
This is a very unusual case. We sign-out the case as high grade malignant tumor with divergent differentiation with a long comment.
It can be considered as a variant of MMMT for practical purpose. Gross examination demonstrated a endometrial polyp. The polyp was entirely dubmitted for histologic evaluation. Half of the polyp is like atrophic polyp and the remainder of the histologic sections deminstrated several tumor nodules predominantly composed of medium-size, round to oval, hyperchromatic cells with scant cytoplasm, abundant apoptosis and numerous mitotic figures. These tumor cells show divergent differentiation i.e. patchy reactivity for cytokeraiton (with CAM5.2 reactivity greater than Pan-CK), focal reactivity for mesenchymal marker vimentin, patchy moderate to strong reactivity for neuroendocrine markers, and patchy strong reactivity for muscle markers (desmin and specific skeletal muscle marker-myogenin). Foci demonstrate obvious high grade adenocarcinoma component admised with the above-described high grade tumor component. Given the misture of obvious carcinoma component and high grade malignant tumor component with divergent differentiation, the tumor is classified as a MMMT with heterologous rhabdomyosarcoma component. Whether the epithelial and neuroendocrine marker ecpression, in the tumor component that is also staining for myogenin is an aberrant expression or true differentiation, is debatable. However, the strong reactiity for neuroendocrine markers suggests true divergent differentiation.
abin译:
我基本上同意abin的分析。
这是一个非常少见的病例。我们签发为“高级别肿瘤伴异源性分化”并加上一段长长的评注。
从实用的角度,它可以考虑为MMMT的一种亚型。大体表现为子宫内膜息肉,全部取材。一半息肉像萎缩性,其余切片的组织学表现呈数个肿瘤性结节,主要由中等大、圆到卵圆形、深染细胞组成,胞浆少,大量的凋亡和核分裂。这些肿瘤细胞呈异源性分化,即:上皮标记物片状阳性(CAM5.2比panCK表达更强),间叶标记物Vim局灶阳性,片状中-强阳性表达神经内分泌标记物,片状阳性表达肌源性标记物(desmin和myogenin)。局灶呈明显的高级别腺癌混杂上述高级别肿瘤成分。考虑到明显的癌成分和高级别恶性肿瘤成分伴多向分化,肿瘤归类于MMMT伴异源性横纹肌肉瘤成分。表达上皮性和神经内分泌标记物的肿瘤成分成表达myogenin,这种情况是异学表达还是真性分化,存在争论。然而,神经内分泌标记物强阳性提示确实存在异源性分化。
-
本帖最后由 于 2008-12-23 23:25:00 编辑
The second panel of IHC results were not what we expected.
第二组IHC结果出乎意料。
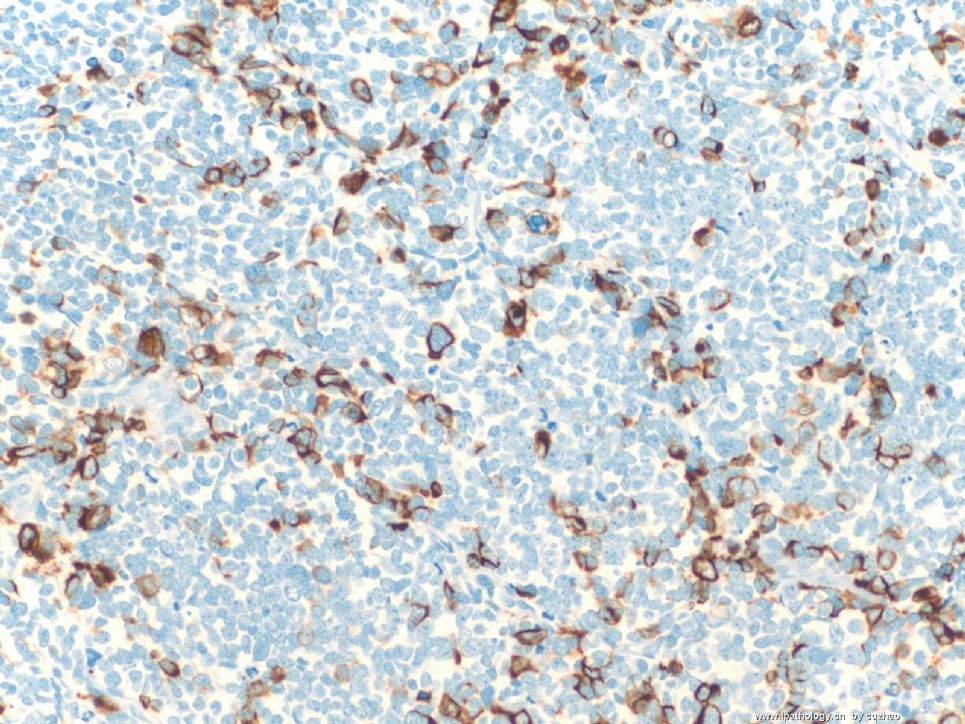
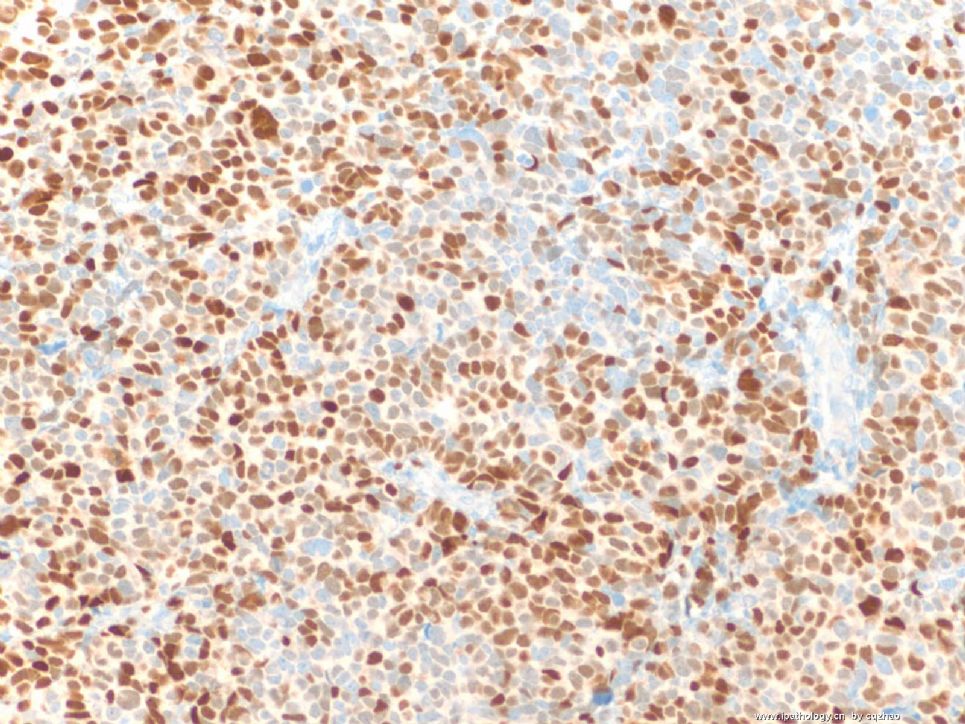
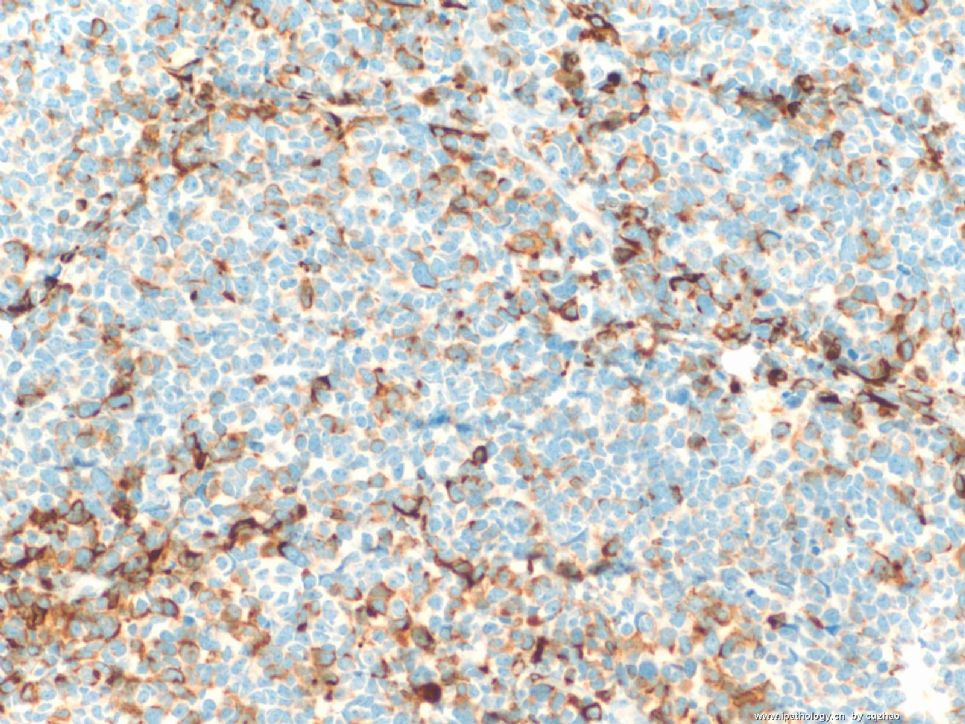
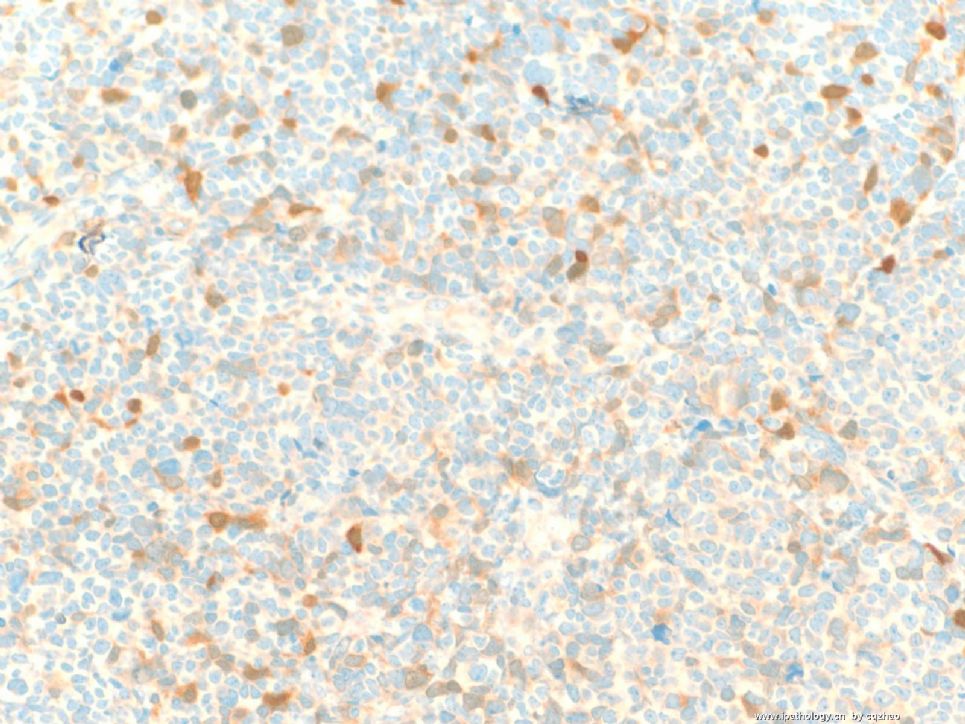
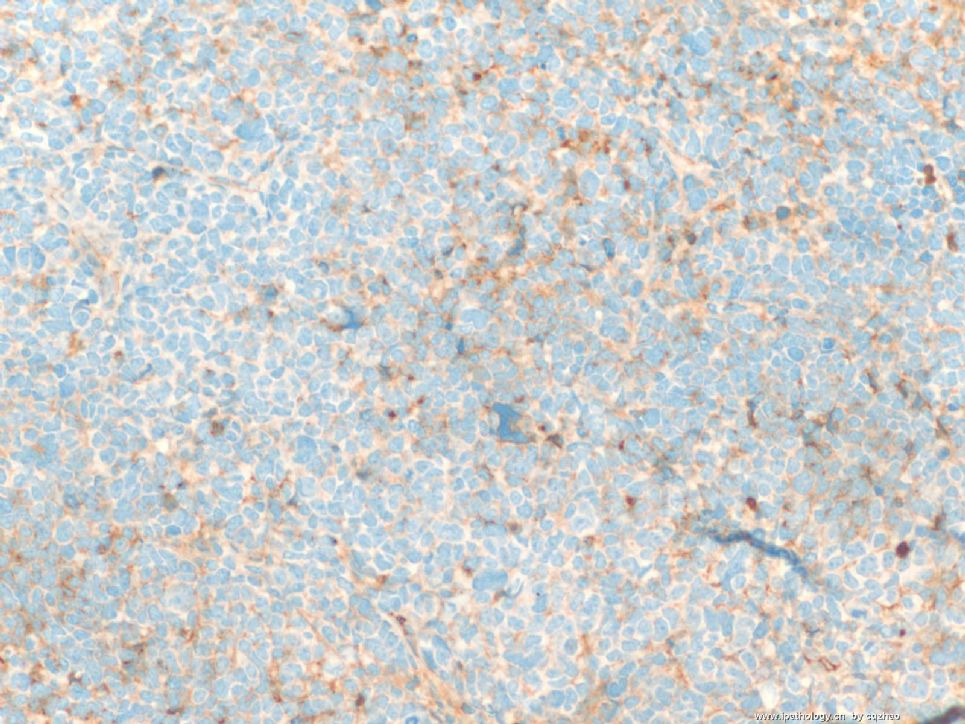
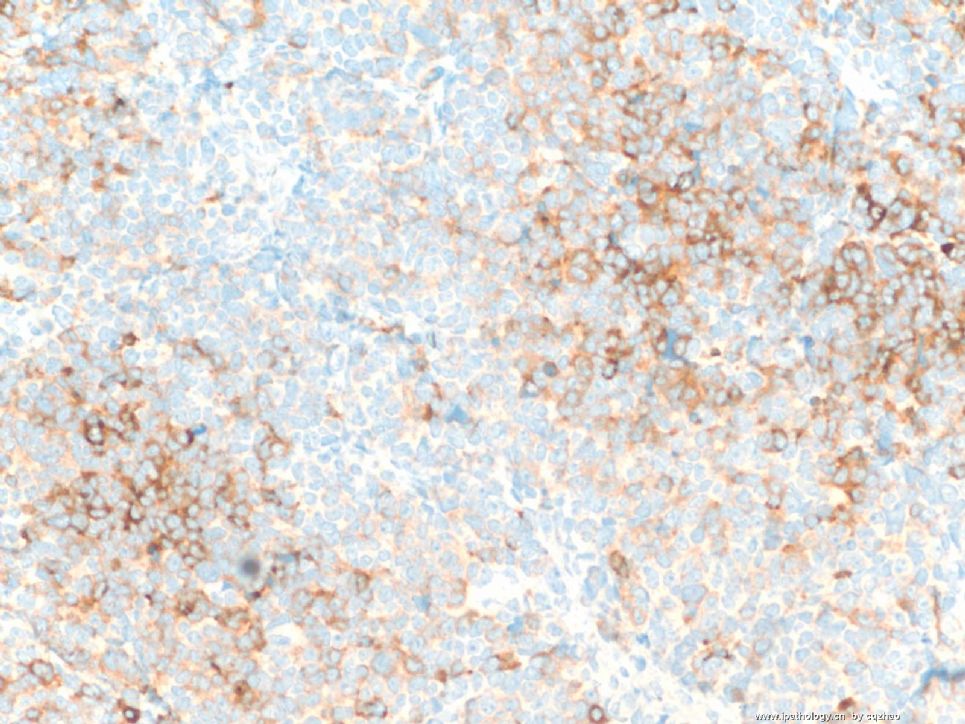
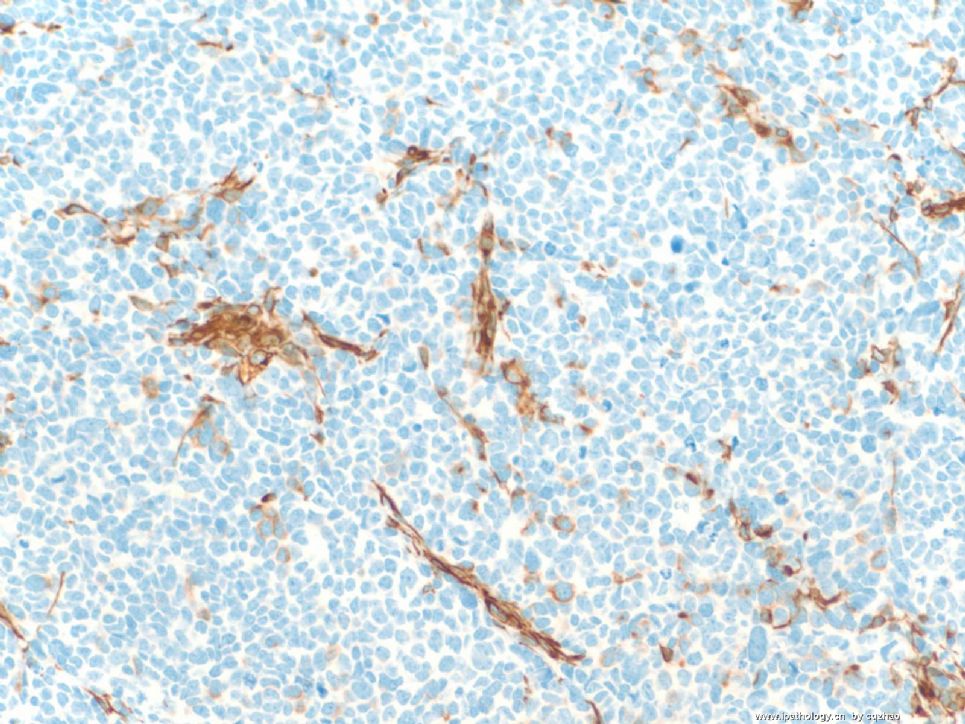
Focal area with IHC:
局部区域IHC图:
f1 Cam5.2
f2 myogenin
f3 desmin
f4 myoglubin
f5. chrom
f6. synaptophysin
f7 vimentin
The area is not the same area I sent you the IHC photos before.
Now what do you think? It is ususual case.
这一区域与前一次上传的免疫组化图片是不同区域。
现在你考虑什么?这是少见病例。
名称:图1
描述:图1
名称:图2
描述:图2
名称:图3
描述:图3
名称:图4
描述:图4
名称:图5
描述:图5
名称:图6
描述:图6
名称:图7
描述:图7











