
图1")
图2")
图3")
图4")
图5")
图6")
图7")







| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- B1301Uterine high grade malignant tumor with divergent differentiation (cqz3)
图1") 图1
图1图2") 图2
图2图3") 图3
图3图4") 图4
图4图5") 图5
图5图6") 图6
图6图7") 图7
图7
| 姓 名: | ××× | 性别: | 年龄: | ||
| 标本名称: | |||||
| 简要病史: | |||||
| 肉眼检查: | |||||
Share a case of this week.
Old lady with atrophic endometrium showing tumor mass in the surface of cystic atrophic endometrium (first figure)
F1 20x
F2 100x
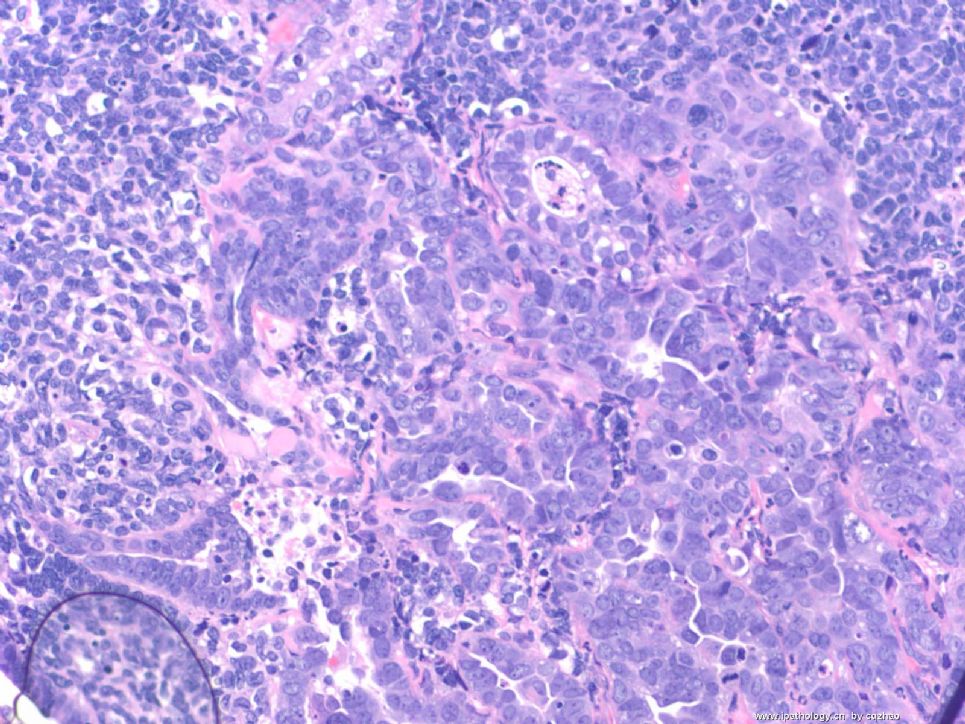
F3 200x
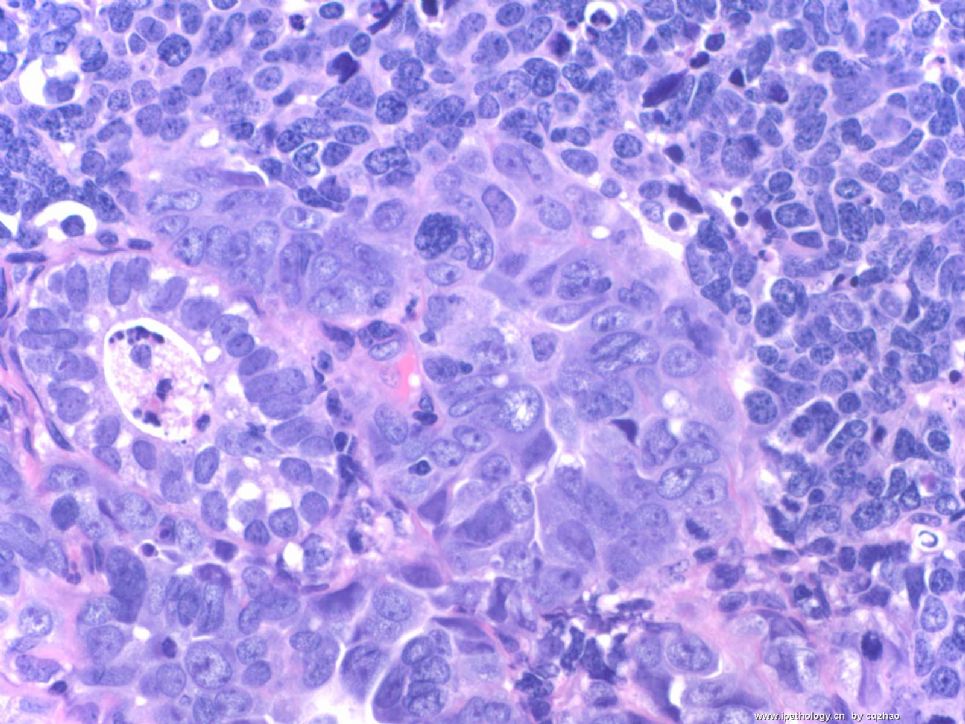
F4-5 400x
F6 200x
F7 400x
F6 and 7 showing focal glandular lesion mixed with other solid lesion.
Your dx or differential dx
标签:子宫 高级别肿瘤 异源性分化
-
本帖最后由 于 2009-02-25 09:51:00 编辑
相关帖子
- • 来一例简单罕见的(有诊断)
- • 是肉瘤吗?
- • 子宫内膜,复杂性增生?癌?(有大体结果了)
- • 子宫肿物(透明细胞平滑肌瘤?)
- • 子宫肌壁间肿物
- • 子宫腔内占位。
- • 子宫肿瘤
- • 子宫肌层浸润性癌
- • 8 个子宫上皮肿瘤病例-扫描图片
- • 子宫平滑肌肿瘤?间质肉瘤?
×参考诊断
高级别肿瘤伴异源性分化
-
本帖最后由 于 2008-12-21 02:09:00 编辑
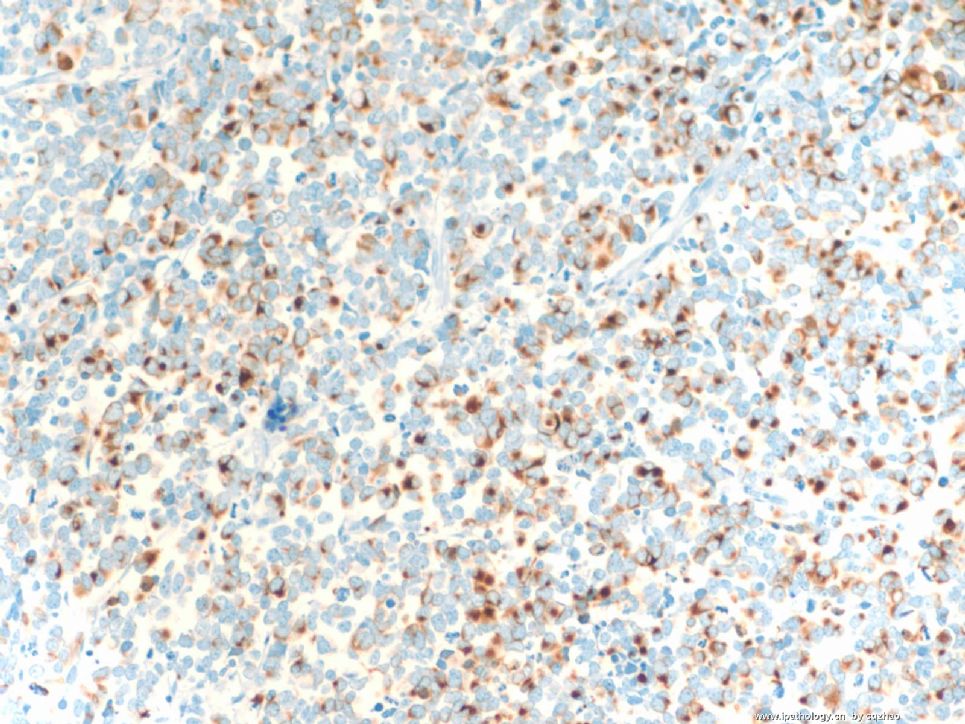
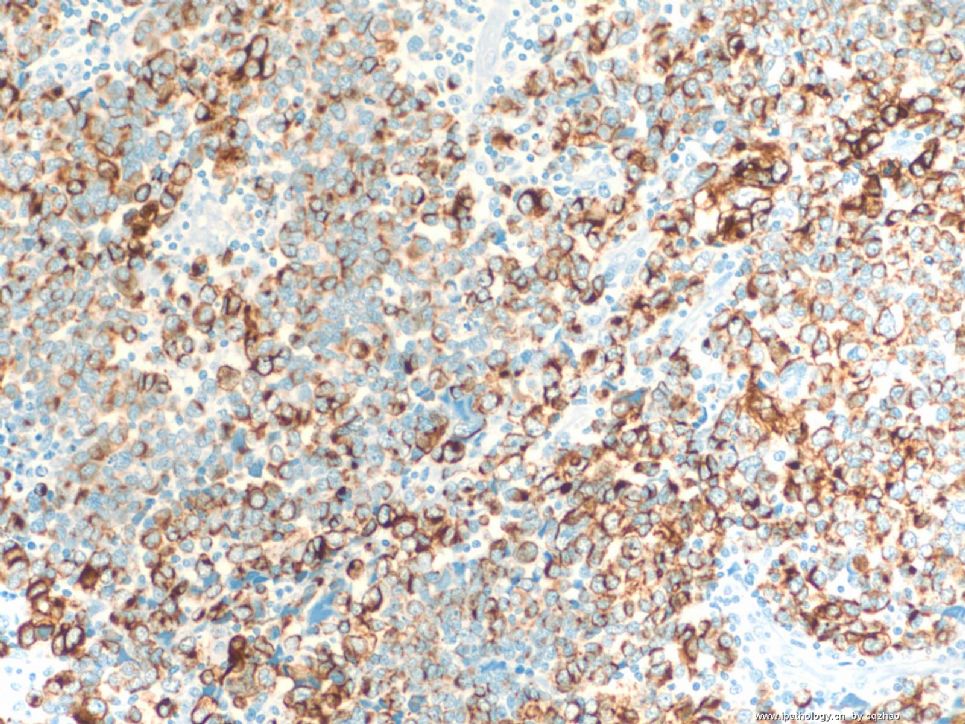
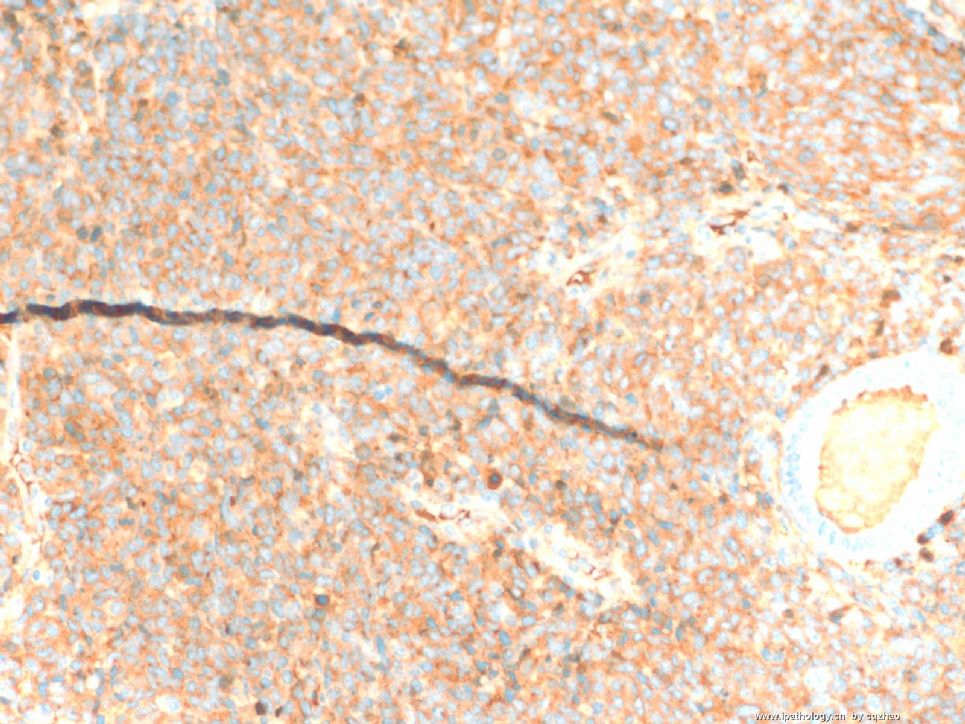
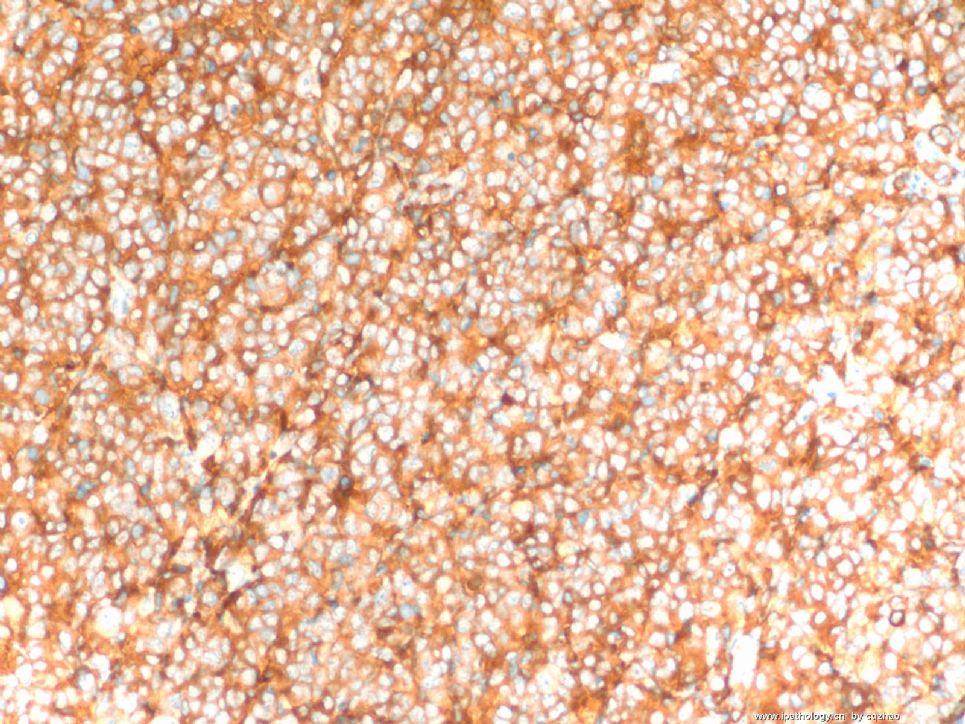
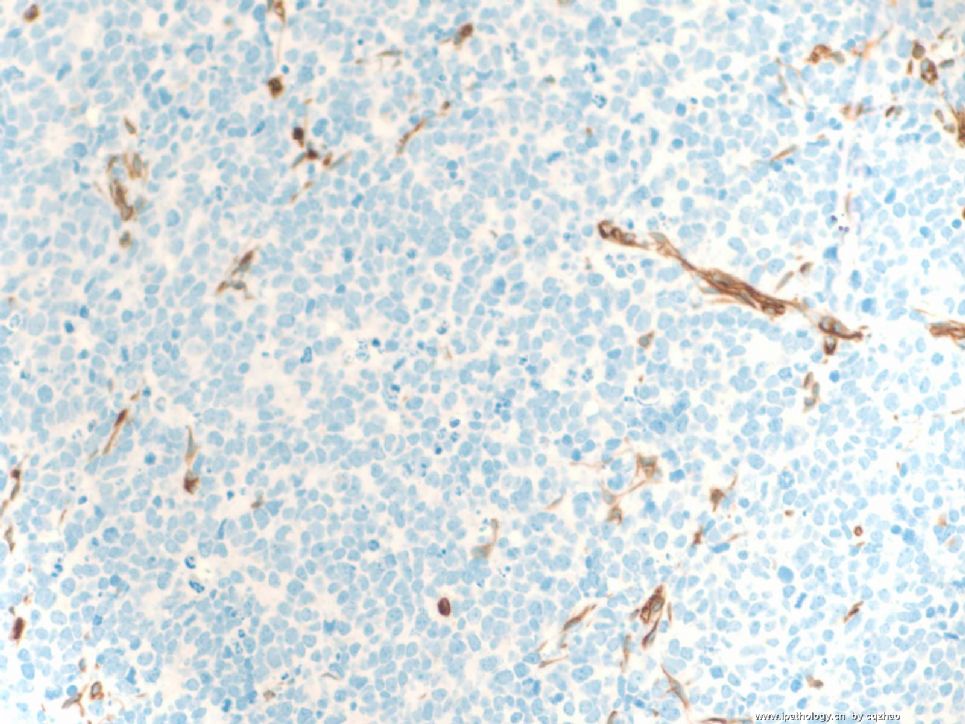
This is my colleague's case. I reviewed the case for diagosis. When we got the above IHC results we thought it is high grade, undifferentiated or poorly differentiated carcinoma with neuroendocrine features plus with well differentiated adenocarcinoma (glanular componnet). I think it is interesting case. Morphology likes a MMMT, but it is a carcinoma finely. So I sent the case for sharing.
More IHC were ordered for this case.
See Photos
abin译:
这是同事的病例,我复片诊断。我们得到免疫组化结果时,认为它是高级别、未分化或低分化癌伴神经内分泌特征,并有高分化腺癌成分(腺样成分)。我觉得这例很有趣。形态学像MMMT,但它是纯粹的癌,因此上传分享。
这例还有更多免疫组化,见图。
-
本帖最后由 于 2008-12-15 23:01:00 编辑
Sharp eyes. I will send some IHC photos in the weekend.
The main differential dx: MMMT (癌肉瘤) vs carcinoma. I may need to learn how to type Chinese. Who would like to be my teacher? In fact my Chinese Pin Yin is very good. Ha, ha
abin译:
目光锐利。周末我会上传一些免疫组化图片。
主要鉴别诊断:恶性苗勒氏混合瘤(癌肉瘤)VS癌。
我可能需要学习中文打字了。谁愿意做我的老师?事实上我的中文拼音非常好,哈哈。
(如果赵老师想学中文打字,abin愿意效劳。我精通五笔盲打,各种拼音输入法也很熟练。)
-
本帖最后由 于 2008-12-11 23:35:00 编辑
All the cases posted by Dr. Zhao are pretty interesting. This case is no exception. Basically, we all agree that it is a high-grade malignancy and it mostly likely involve an endometrial polyp (fist figure). There are mainly several possibilities: 1) a high nuclear grade carcinoma (such as serous carcinoma or undifferentiated carcinoma); 2) Carcinosarcoma (癌肉瘤); 3) Adenosracoma (腺肉瘤) with sarcomatous overgrowth. I don't think that this case fits well with adenosarcoma, since I favor there is at least some adenocarcinomatous components. I did not realize that even expert GYN pathologists cannot always agree on the diagnosis of Cracinosarcoma until I came to Cleveland Clinic and learned GYN path from Dr. Bill Hart (one of the top GYN pathologists in the USA). He has a very strigent criteria for Carcinosarcoma, which should have a perfect bi-phasic pattern of malignant glands and stroma. I doubt that he will call this thing carcinosarcoma.
For all practical purpose, we would NOT do a lot immunostains in biopsy cases in our practice, since the clinical management does not matter, if you call high-grade carcinoma vs. carcinosarcoma or even adenosarcoma with sarcomatous overgrowth, it will be total hystrectomy with lymph node staging. So, we usually further classify a tumor on the bigger resection specimen. Not uncommon, you thought it was high-grade carcinoma on the biopsy, but when the whole uterus came out, it clearly showed carcinosarcoma. Is this a biopsy (curretings) or hysterectomy? Thanks!
abin译:
Dr. Zhao提供的病例都非常有趣,这一例也不例外。我们基本上都一致认为它是高级别恶性肿瘤,并且它可能累犯子宫内膜息肉(第1图)。有几种可能性:1)高核级别的癌(如浆液性癌或未分化癌);2)癌肉瘤;3)腺肉瘤伴肉瘤样过度生长。我认为不太像腺癌,我倾向于至少有部分腺癌样成分。在我来到Cleveland Clinic并向Dr. Bill Hart(美国顶级妇科病理专家之一)学习妇科病理之前,不知道即使妇科病理专家对癌肉瘤的诊断也不一致。他对癌肉瘤有非常严格的诊断标准,即:恶性腺体和间质必须形成非常完美的双相性形态。
从实用角度看,我们不会对活检标本做许多免疫染色,因为临床处理差别不大,如果称为高级别癌vs癌肉瘤vs腺癌伴肉瘤样过度生长,都是全子宫切除加淋巴结分期。因此,我们通常在较大标本上作进一步分类。不少情况下,活检认为是高级别癌,而全子宫标本变成明显的癌肉瘤。这是活检(诊刮)还是子宫切除标本?谢谢!











