
图1")
图2")
图3")
图4")
图5")
图6")
图7")
图8")
图9")
图10")
图11")
图12")
图13")
图14")
图15")
图16")
图17")












| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
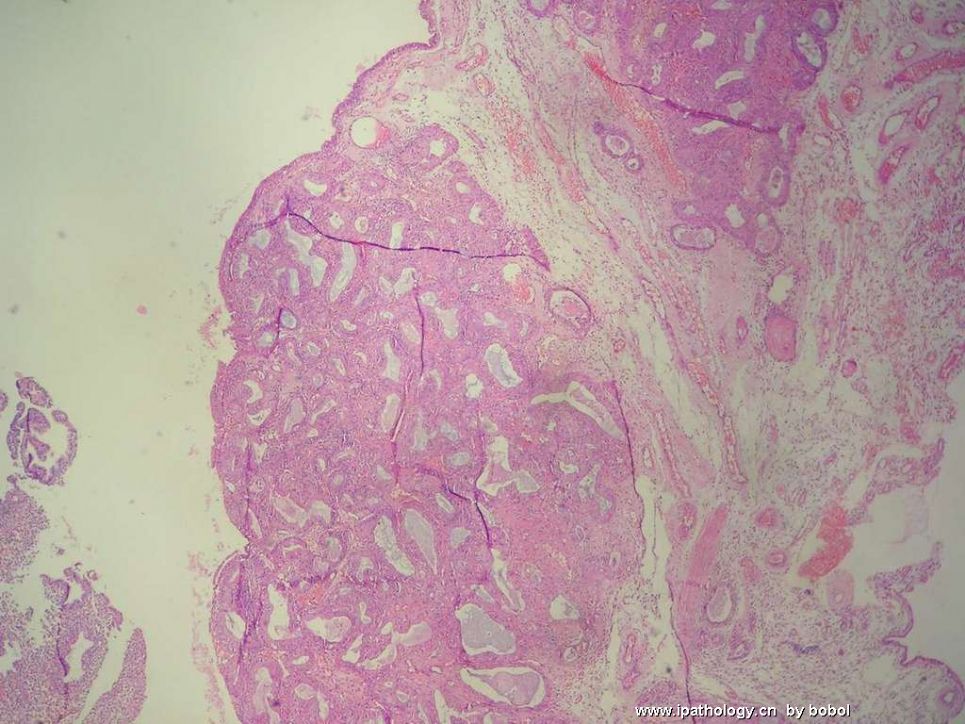
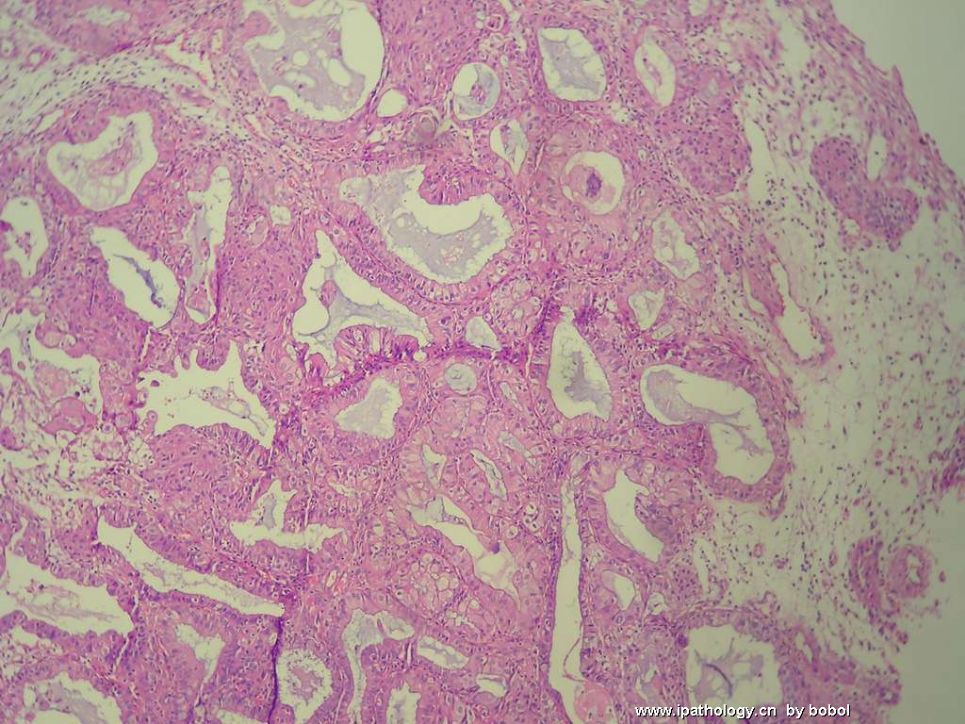
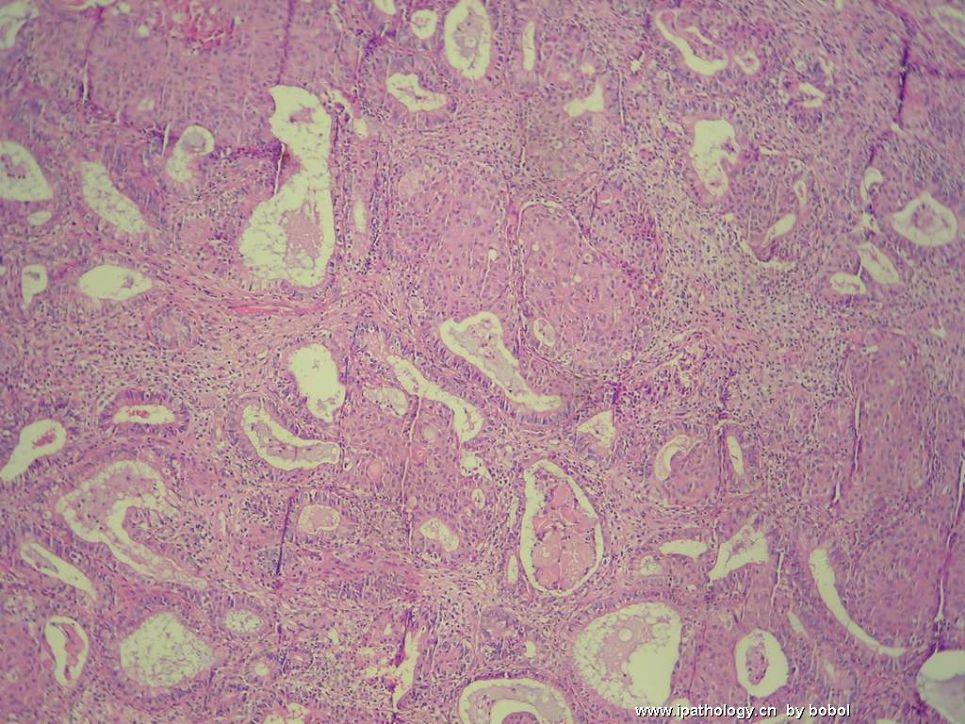
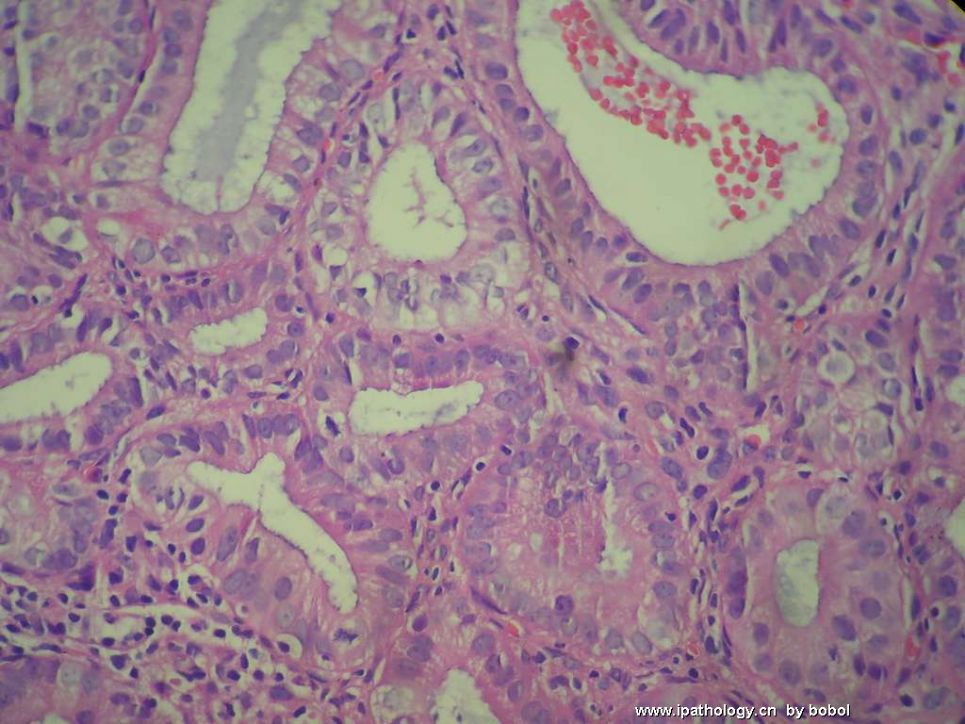
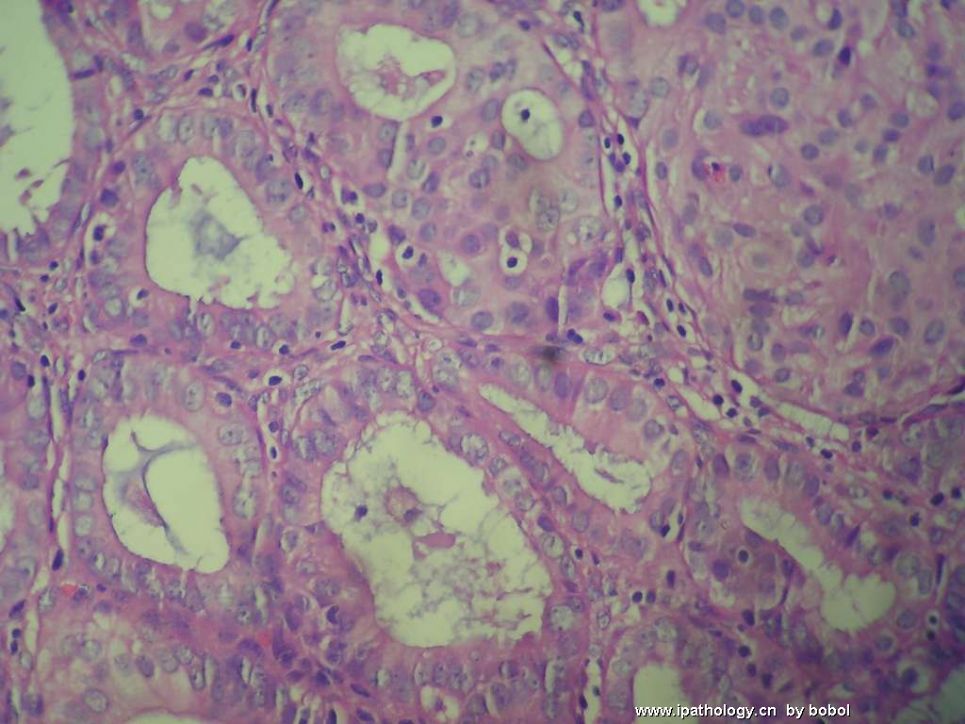
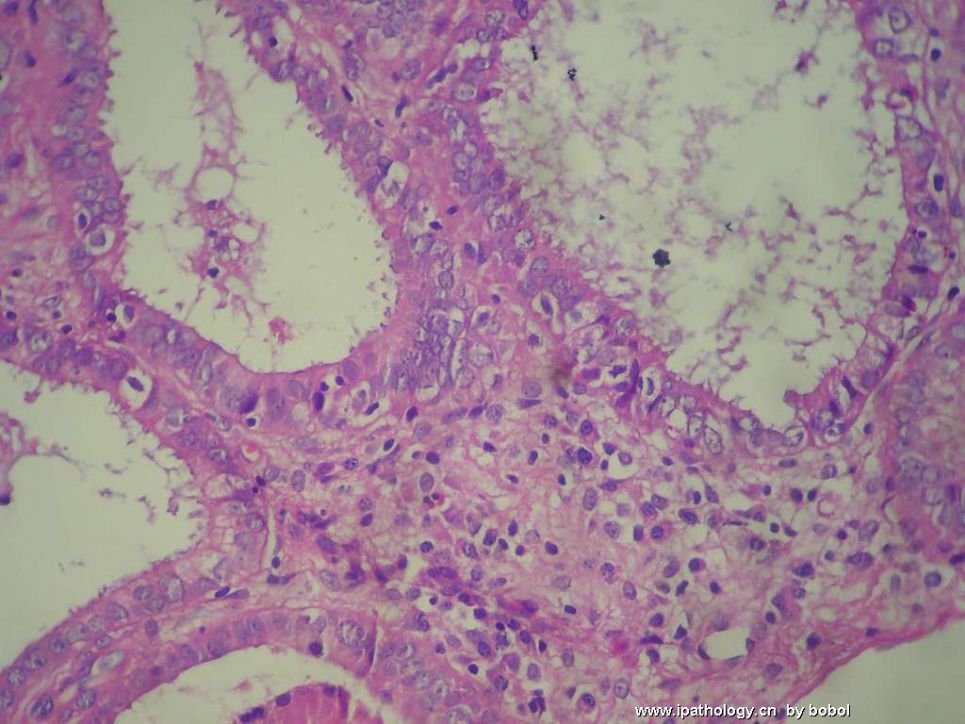
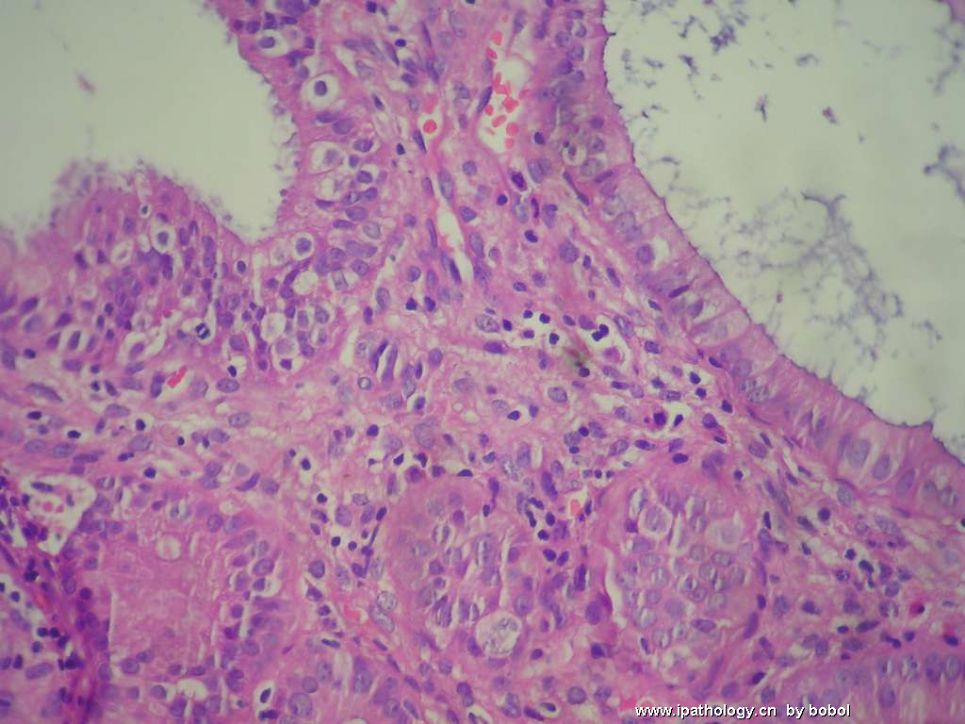
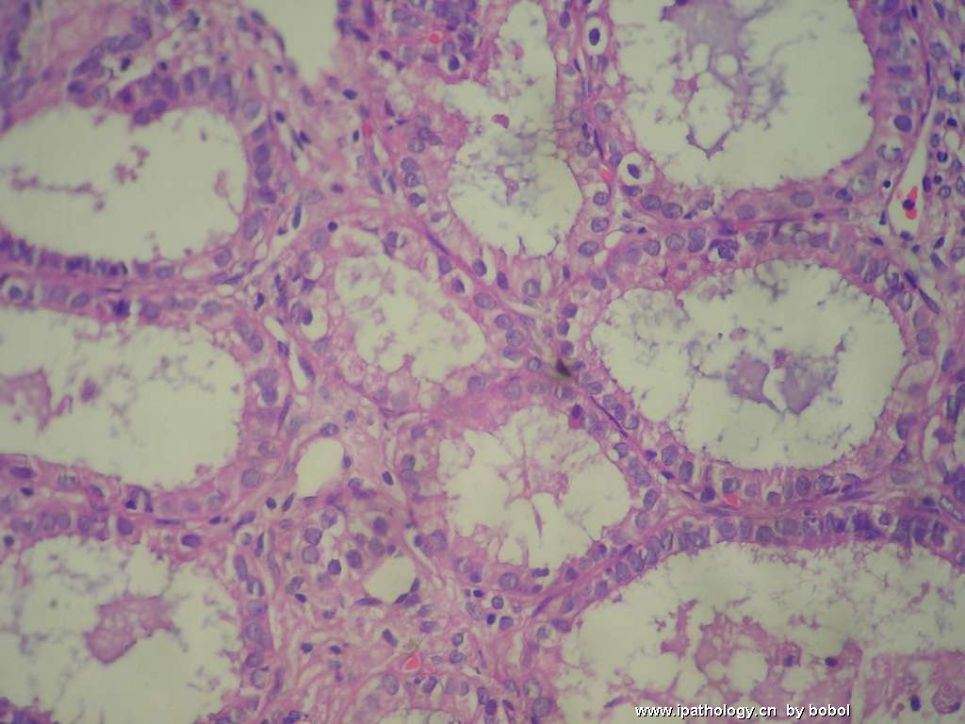
- 子宫内膜活检一例(患者来做术前诊刮了)
图1") 图1
图1图2") 图2
图2图3") 图3
图3图4") 图4
图4图5") 图5
图5图6") 图6
图6图7") 图7
图7图8") 图8
图8图9") 图9
图9图10") 图10
图10图11") 图11
图11图12") 图12
图12图13") 图13
图13图14") 图14
图14图15") 图15
图15图16") 图16
图16图17") 图17
图17
患者,39岁,阴道出血一月余。妇检:宫颈内口赘生物,切除局部组织活检。07年5月因阴道流血曾行子宫内膜诊刮并活检,清宫后止血,现又出现阴道流血……去年切片图像与现在相仿(去年切片借片后遗失……)。
今日电话联系了负责取材的妇产科医生,据描述:“送检物取自子宫颈管,但肿物并非与宫颈管相连,而似由宫腔内长出突出于宫颈管,肿物质脆,极易出血(用棉签轻触即出血)”。患者是在门诊做的检查,因门诊部器械不足,妇科医生怕引起大出血,因而只用竹签挑取了少量肿物送检。另外去年的清宫组织物切片正在追回中,望近日能将图片上传。
去年借片的图片发布在本帖第2页的第28楼、29楼。近日诊刮图片在44楼。
标签:子宫内膜 息肉
-
本帖最后由 于 2008-08-08 18:59:00 编辑
相关帖子
×参考诊断
一个很好的子宫内膜息肉的讨论病例
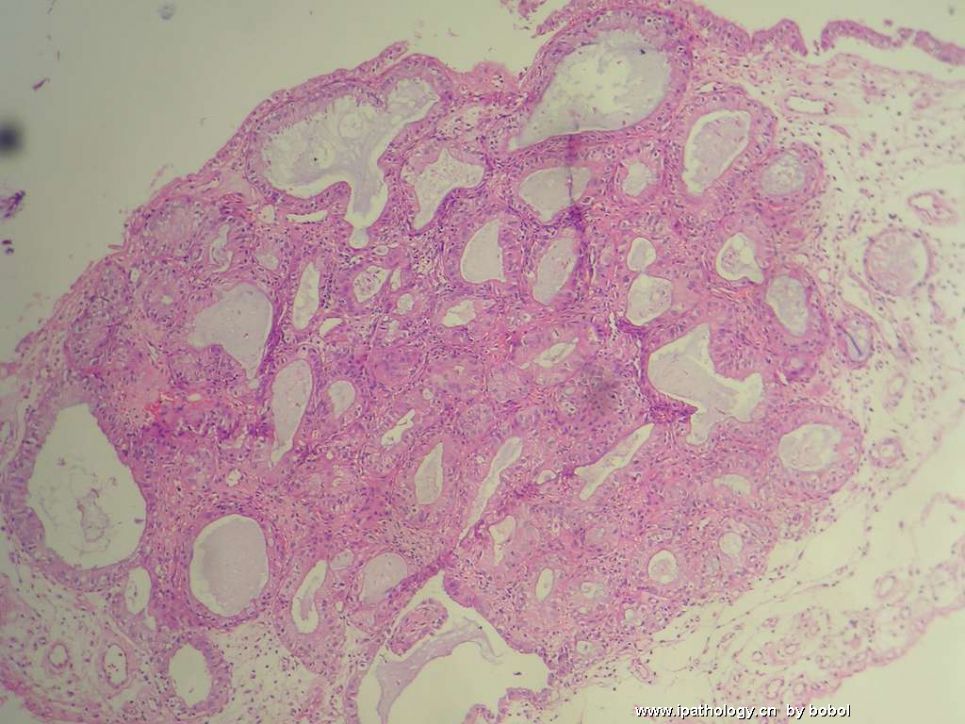
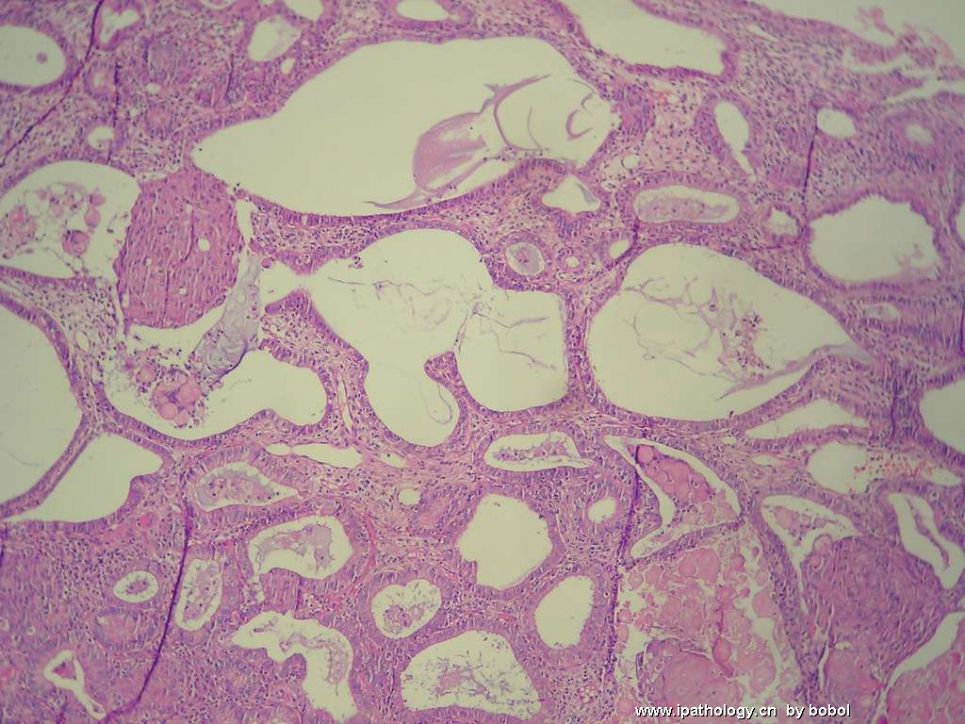
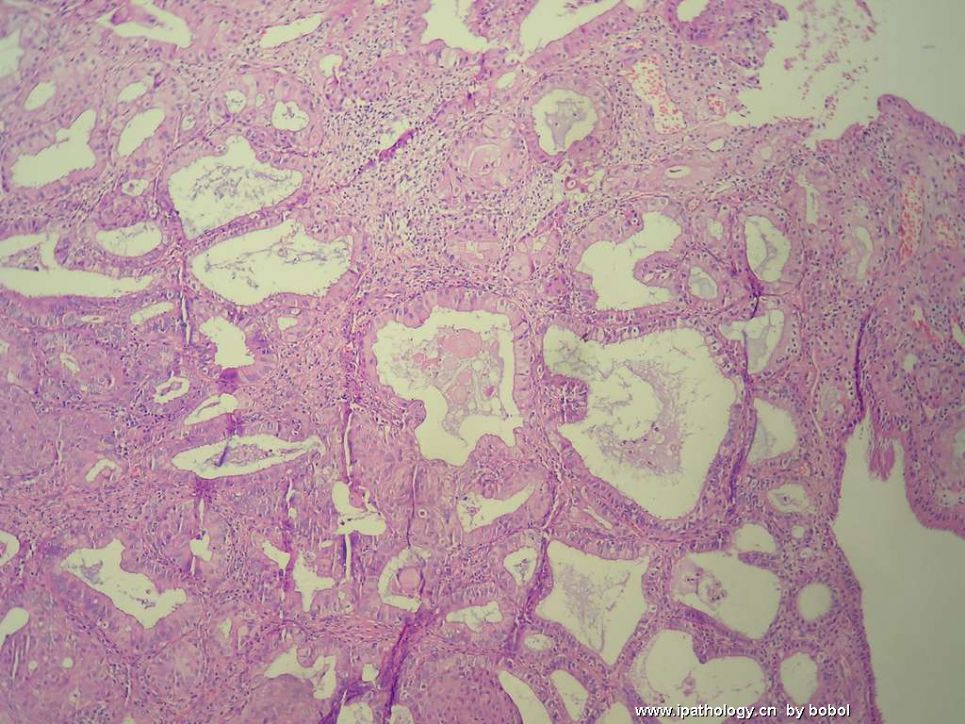
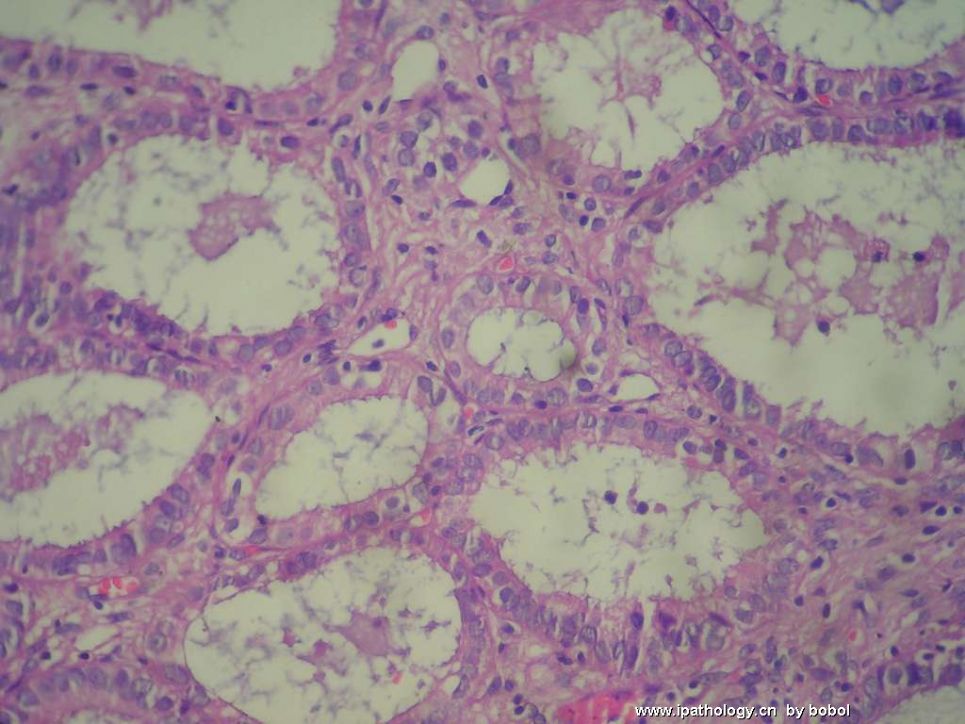
1、子宫内膜息肉
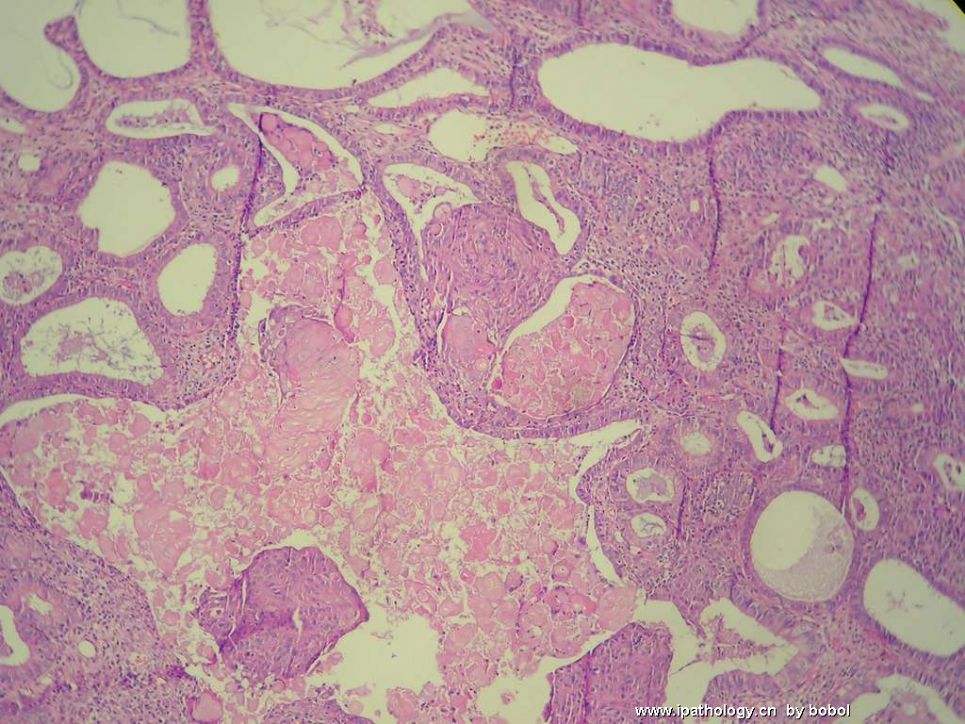
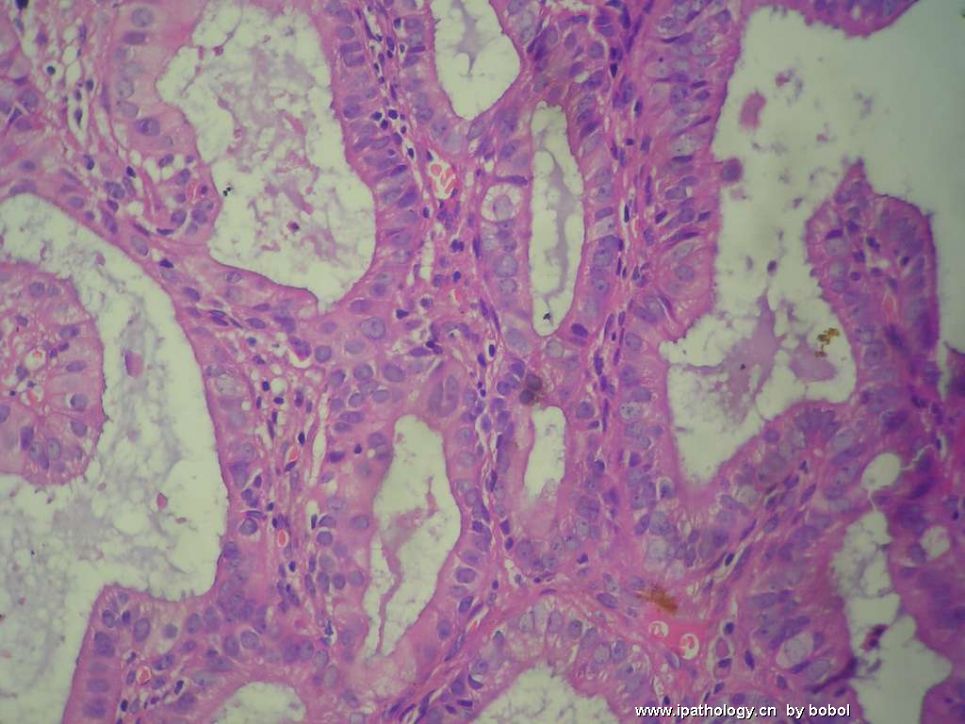
息肉中的腺体可以出现各种改变,包括不典型增生和癌。
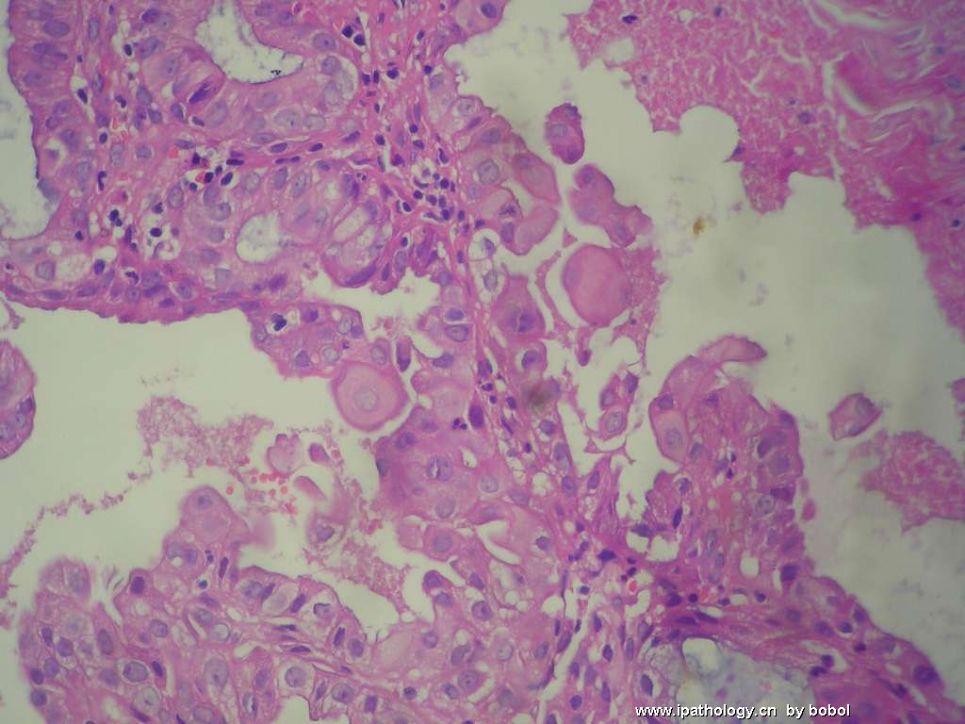
这例出现腺体简单型增生,灶性复杂性增生,轻微的不典型增生,鳞化。总之,无癌。
2、慢性子宫内膜炎
如何处理?
1、看B超,病变到底有多大?B超诊断?
2、临床所见,病变很大,活检很少,会不会有更严惩的病变?无法预测。
3、如何手术?首选宫腔镜切除全部病变,再次病理检查,看情况再作进一步处理。如果临床有手术指征并且患者愿意,也可直接子宫次全切除。
最好与患者充分交流,让患者了解全部情况,让患者自己决定。

华夏病理/粉蓝医疗
为基层医院病理科提供全面解决方案,
努力让人人享有便捷准确可靠的病理诊断服务。
-
本帖最后由 于 2008-06-28 12:56:00 编辑
| 以下是引用bobol在2008-6-25 0:35:00的发言:
对子宫内膜息肉的诊断有疑问,片内虽可见少量厚壁血管,但纤维化看起来不太显著,且子宫内膜息肉较少复发(据悉患者已行结扎术,未上环)。子宫内膜间质内有大量的浆细胞等炎症细胞,可考虑子宫内膜炎,但内膜腺体又存在明显增生性改变,与子宫内膜炎的腺体萎缩不符。还是觉得有些怪异…… 如系手术治疗,有全宫切除的必要吗?患者为同事的至亲,该例有点为难了。 |
- “人生没有彩排,每一天都是现场直播”
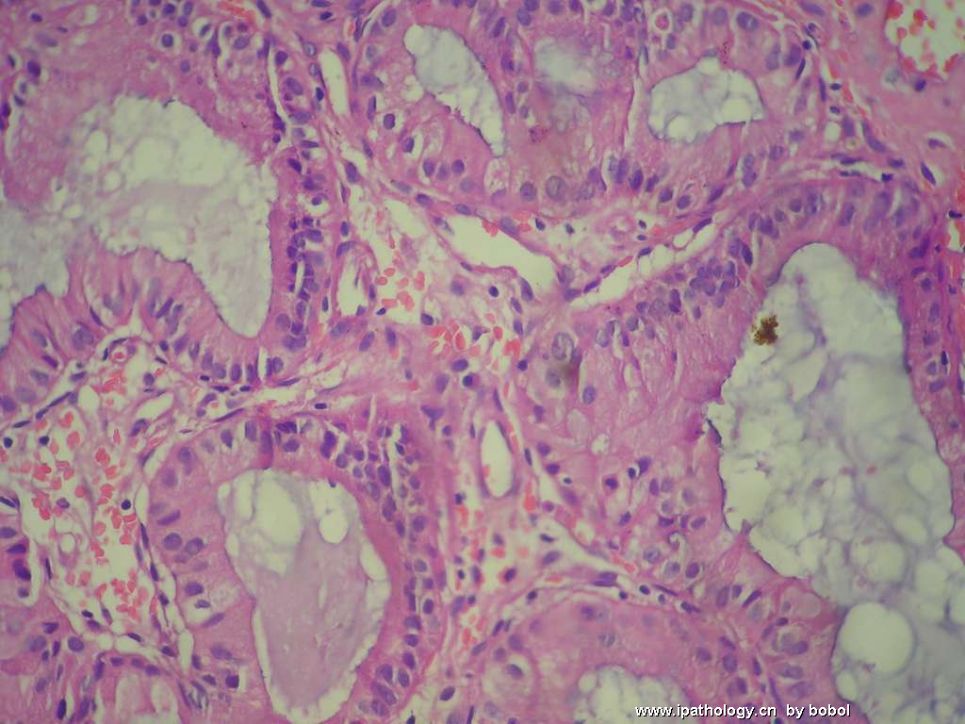
My diagnosis will be: "Complex hyperplasia without nulcear atypia, confined within a benign endometrial polyp with chronic endometritis (复合型子宫内膜上皮增生和鳞状化生, 不伴核间变,局限于一良性内膜息肉内。 伴慢性子宫内膜炎)。
此例关键要看,非息肉宫内膜部分是否也有“复合型子宫内膜上皮增生和鳞状化生”。如果没有,建议临床抗生素治疗慢性子宫内膜炎。如果内膜息肉完全去除,病人随访即可; 如果非息肉宫内膜部分也有复合型子宫内膜上皮增生和鳞状化生,建议临床使用孕激素治疗子宫内膜上皮增生。
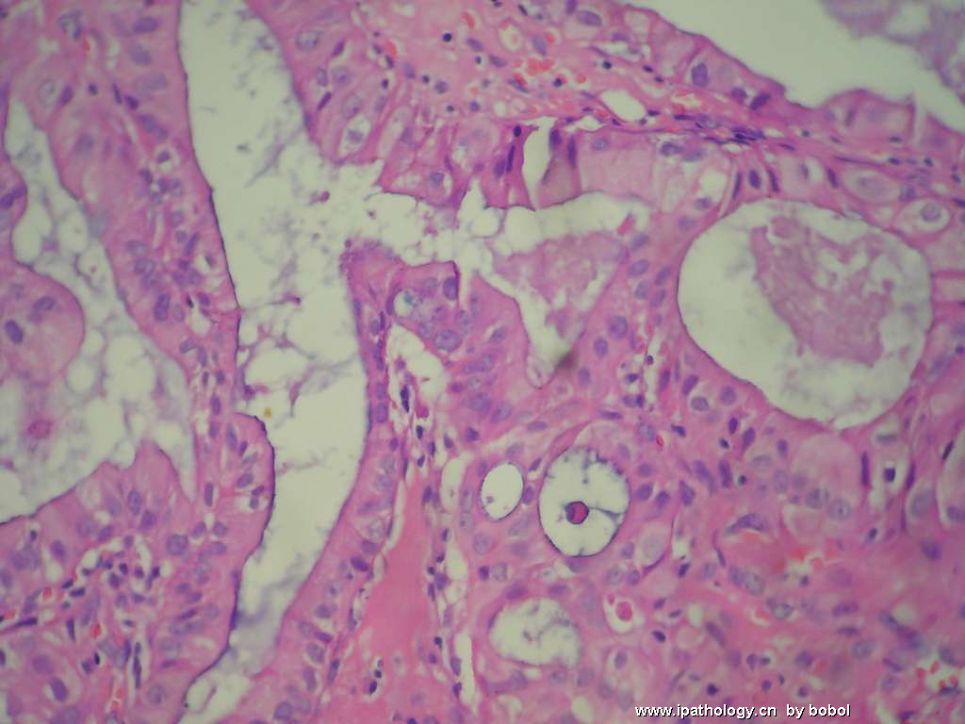
I conceptually agree with Dr. Yu's analysis. My only concern is that squamous metaplasia is not usually seen in benign endometrial polyp, without hyperplasia. In a situation we see squamous metaplasia in an endometrial polyp, there are two differential diagnoses we should entertain: 1) atypical polypoid adenomyoma (APA), 2) complex hyperplasia within the polyp. In the former, hyperplasia is similar to atypical complex hyperplasia with nuclear atypia. I did not see smooth muscle bundles in the picture provided. Therefore, I speculate this is enough to call "complex hyperplasia without nuclear atypia". I agree with Dr. Yu that we usually tolerate some complexity and irregularity of glands within an endometrial polyp. Without squamous metaplasia, I may let it go as "Benign endometrial polyp with Chronic endometritis". However, given the infrequence to see squamous metaplasia in a usual polyp, and given the complex glandular archtecture in the focus which is so different from surrounding polypoid tissue, I think it is appropriate to render the diagnosis of "complex hyperplasia" in this case. It is soly academic exercise here. Clinically, it did not change much regarding exogenous progestin therapy, unless there is complex hyperplasia present in non-polypoid endometrium. The latter will be the key evaluation in this case.
- 不坠青云之志,长怀赤子之心
谢谢mingfuyu和杨斌老师精彩的点评,小结如下,供学习:
mingfuyu
诊断:子宫内膜息肉伴子宫内膜炎。上皮反应性改变(胞核变大,核仁明显),并不萎缩,也不够非典型增生。间质较多,纤维化不明显。
处理意见:取宫腔内子宫内膜做细菌培养,然后抗生素治疗。内膜息肉本身并不可怕,刮掉就好。病人需随访。
杨斌
诊断:复合型子宫内膜上皮增生和鳞状化生, 不伴核间变,局限于一良性内膜息肉内。 伴慢性子宫内膜炎)。
处理意见:此例关键要看,非息肉宫内膜部分是否也有“复合型子宫内膜上皮增生和鳞状化生”。如果没有,建议临床抗生素治疗慢性子宫内膜炎。如果内膜息肉完全去除,病人随访即可; 如果非息肉宫内膜部分也有复合型子宫内膜上皮增生和鳞状化生,建议临床使用孕激素治疗子宫内膜上皮增生。
华夏病理/粉蓝医疗
为基层医院病理科提供全面解决方案,
努力让人人享有便捷准确可靠的病理诊断服务。
Dear Dr. Yang,
So nice to have professional discussion here with you. We have met in USCAP 2006 in Atlanta and i believe we both had the previlege to be trained at BJC/Wash U under superb pathologists like Dr. Huttner and Dr. Dehner. thank you for your comment. I did not pay much attention to the squamous metaplasia in this case because i feel i see squamous met in benign endometrium sometimes, sometimes mimicking epithelioid granulomas. I have seen squamous metaplasia associated with chronic endometritis numerous times. I remember in my early cases, I always do AFB GMS, as our attendings have emphasized for years (but they are almost always negative, only one positive case in my career so far). Then i learned that those are squamous met associated with -itis. Then i did find some literatures or books talking about squamous met as reactive changes.
I like this website very much. Now i feel i work as a pathologist day and night, as to show how much i like it! Ha Ha1











