

















| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- 胃粘膜下占位-上海市骨与软组织读片2013(12)上交大附属瑞金医院提供
-
上交大附属瑞金医院提供图1") 图1
图1 -
上交大附属瑞金医院提供图2") 图2
图2 -
上交大附属瑞金医院提供图3") 图3
图3
| 性别 | 男 | 年龄 | 31岁 | 临床诊断 | 胃体大弯侧粘膜下占位 |
|---|---|---|---|---|---|
| 一般病史 | 无明显诱因下上腹隐痛。超声内镜:粘膜下见低回声病灶,边界清晰,包膜完整,直径为12.4×10.8mm,提示粘膜下占位。• 腹部CTA:胃体大弯侧胃壁局部增厚,可见结节状等密度灶,大小约1.5×1.3cm,边缘光整,增强动脉期可见明显强化,(平扫CT值约14Hu,动脉期CT值约169Hu,门脉期CT值约128Hu)。 | ||||
| 标本名称 | 胃体大弯侧粘膜下肿块 | ||||
| 大体所见 | 结节一枚,大小1.3×1.3×1cm,切面灰红、质中,局部表面覆胃壁,大小3×3×1.5cm,与肿块相连处粘膜局部隆起。 | ||||
标签:胃 粘膜下 占位
-
本帖最后由 海上明月 于 2013-09-09 23:21:26 编辑

- 王军臣
×参考诊断
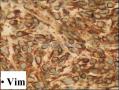
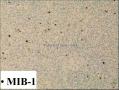
“胃大弯侧” 间叶源性肿瘤。形态学不完全符合胃肠道间质瘤,免疫组织化学结果提示(CD117 -/+, Dog-1 -/+)。倾向上皮样型GIST。必要时相关基因检测以便靶向药物治疗。
-
snowman103cn 离线

- 帖子:518
- 粉蓝豆:9
- 经验:538
- 注册时间:2010-11-07
- 加关注 | 发消息
文献报道,大约有5%GIST病例不表达CD117等相关标志物。本文研究了26例CD117阴性GIST病例中DOG1 和蛋白激酶C-θ (protein kinase C-θ ,PKC-θ) 的表达。PKC-θ被认为是GIST的标志物之一。本文作者对这26例GIST中KIT 和PDGFRA 进行了分析。结果显示,.26例CD117阴性病例中,表达DOG1 和 PKC-θ 阳性率分别为24 例(92%) 和25 例(96%),其中23例(89%)这两种标记阳性。 基因分析显示,26例中只有15 例 (58%) PDGFRA第18 外显子突变,KIT第11 外显子突变至检出1例 (4%),其余10例 (39%) 仍是野生型的KIT 和 PDGFRA。这些结果给我吗的启示,即便是有新的标志物投入应用,还是有少数病例市区表达GIST相关标志物。
Mod Pathol. 2011 Jun;24(6):866-75. doi: 10.1038/modpathol.2011.11. Epub 2011 Feb 25.
DOG1 and PKC-θ are useful in the diagnosis of KIT-negative gastrointestinal stromal tumors.
Source
Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
Abstract
Pathological diagnosis of gastrointestinal stromal tumors (GISTs) is based on histological findings and immunohistochemical demonstration of the KIT protein. KIT-negative GISTs account for ∼5% of cases and cause diagnostic difficulties. In the era of imatinib therapy, a correct diagnosis of GISTs is important for therapeutic reasons regardless of KIT expression. Recently, DOG1 has been introduced as an important diagnostic marker with high sensitivity and specificity. In this study, immunohistochemical staining for DOG1 and protein kinase C-θ (PKC-θ) in whole tissue sections, and mutation analyses for KIT and PDGFRA were performed in 26 KIT-negative GISTs. Tissue microarrays of 112 KIT-positive GISTs were used as controls. Overall, 25 KIT-negative GISTs were located in the stomach, and 1 in the rectum. The histological subtype was spindle in 12, epithelioid in 11, and mixed in 3 cases. The expression of DOG1 and PKC-θ was positive in 24 (92%) and in 25 cases (96%), respectively. All 26 KIT-negative GISTs expressed either DOG1 or PKC-θ, and 23 cases (89%) were positive for both makers. PKC-θ was positive in two cases (8%), which lacked both KIT and DOG1 expressions. Mutation analysis showed PDGFRA exon 18 mutation in 15 cases (58%) and KIT exon 11 mutation in 1 case (4%), whereas the remaining 10 cases (39%) were wild type for both KIT and PDGFRA. The expression of DOG1 and PKC-θ showed no significant difference in KIT-negative and KIT-positive GISTs (P=1.000 and P=0.167, respectively). Our findings suggest that both DOG1 and PKC-θ can be used in the diagnosis of KIT-negative GISTs and they show positive staining even in KIT-negative tumors, which are wild type for KIT and PDGFRA on mutation analysis.
- 王军臣
引用 3 楼 海上明月 在 2013-08-20 09:08:18 的发言:
• 镜下:肿瘤组织主要位于粘膜下层,大部分呈膨胀性生长,局部呈浸润性生长,累及固有层,细胞短梭形或卵圆形,束状片状排列,核圆形,局灶见核分裂象(2个/10HPF), 间质血管丰富。
细胞形态和结构不是太像GIST和神经鞘瘤,如果是GIST那也太简单了,不会拿出来讨论了。
当然首先考虑常见的是对的。如果常见的套不进去,就要考虑少见的,少见的也套不进去,还要考虑转移来的。
该例提供的图像信息少了点,那就只好猜了:短梭形至卵圆形的瘤细胞,束状、略编织状和旋涡状排列,细胞界限不清楚,高倍镜下看瘤细胞相对较温和,似乎有个把淋巴细胞,如果只猜一个诊断的话,我首选 滤泡树突细胞肿瘤。
当然,鉴别诊断还有一大堆。
- 博学之,审问之,慎思之,明辨之,笃行之。
-
本帖最后由 jcw62 于 2013-08-20 22:06:31 编辑
引用 3 楼 海上明月 在 2013-08-20 09:08:18 的发言:
• 镜下:肿瘤组织主要位于粘膜下层,大部分呈膨胀性生长,局部呈浸润性生长,累及固有层,细胞短梭形或卵圆形,束状片状排列,核圆形,局灶见核分裂象(2个/10HPF), 间质血管丰富。
首先考虑炎症性肌纤维母细胞瘤(1、肿瘤组织位于粘膜下;2、肿瘤细胞梭形或椭圆形,束状、片状排列,部分区域呈旋涡状,可见炎症细胞浸润;3、间质可见丰富的血管)。
鉴别诊断:1、纤维瘤病;2、滤泡树突状细胞肉瘤;3、GIST;4、其他。











