
腺癌?)图1")
腺癌?)图2")
腺癌?)图3")
腺癌?)图4")












| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
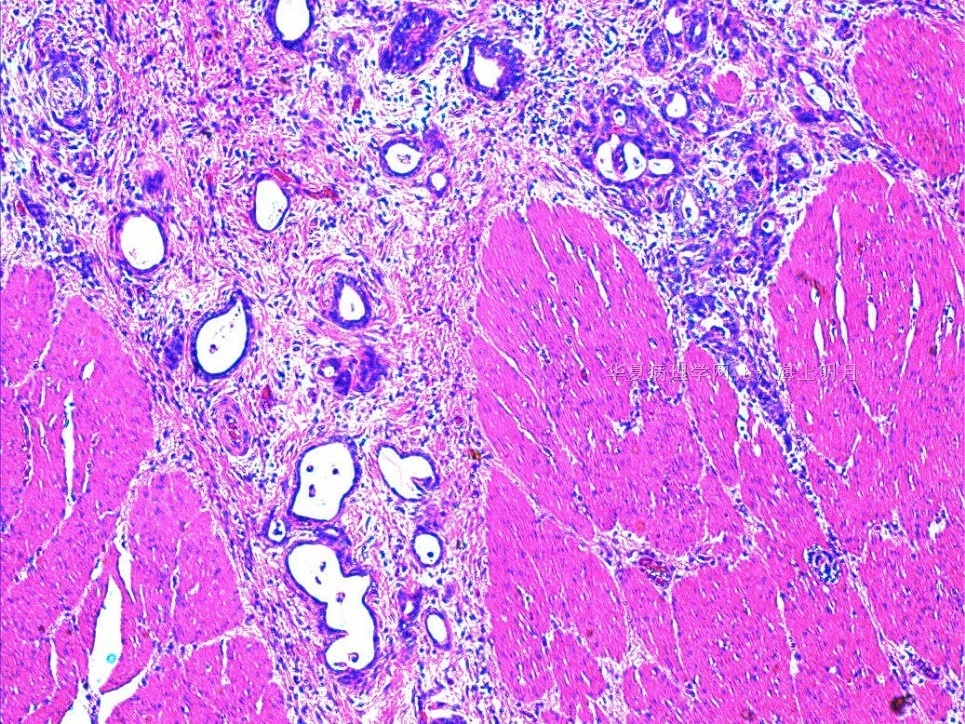
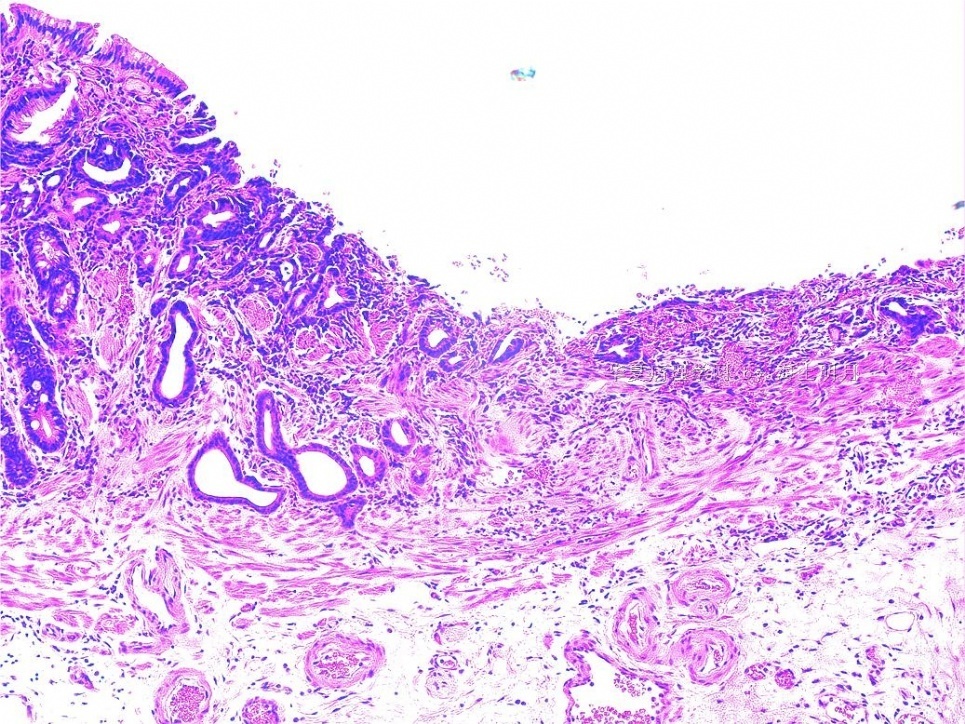
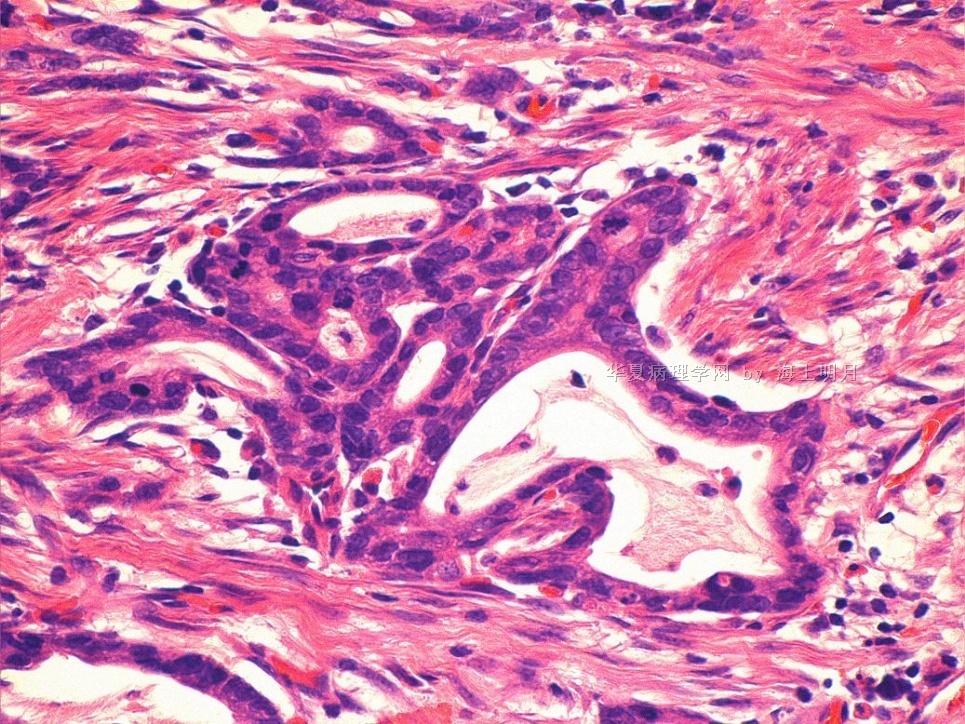
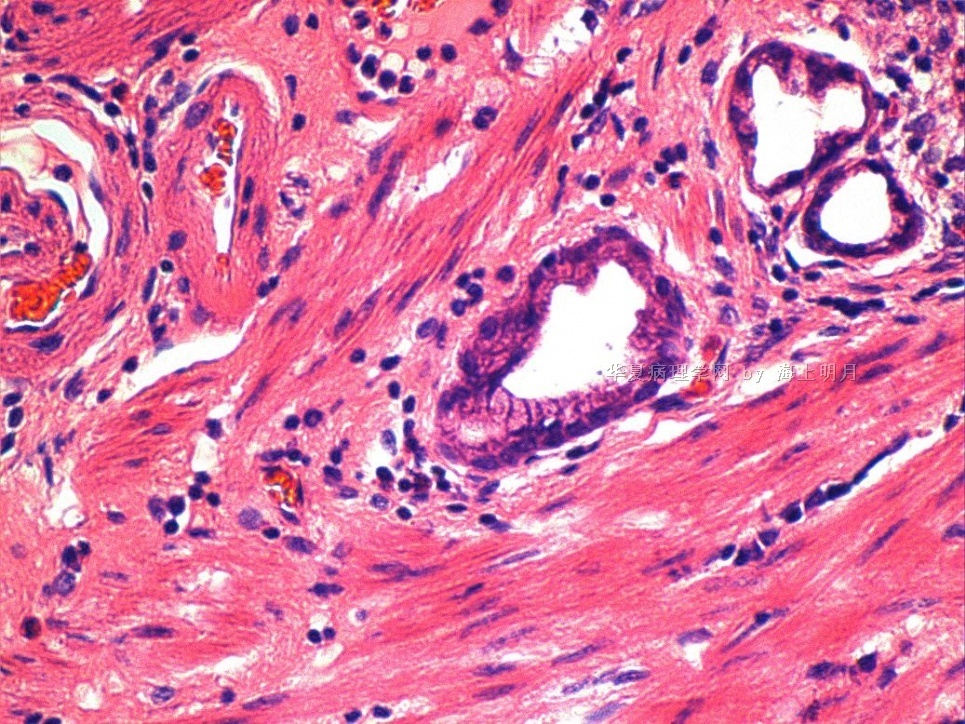
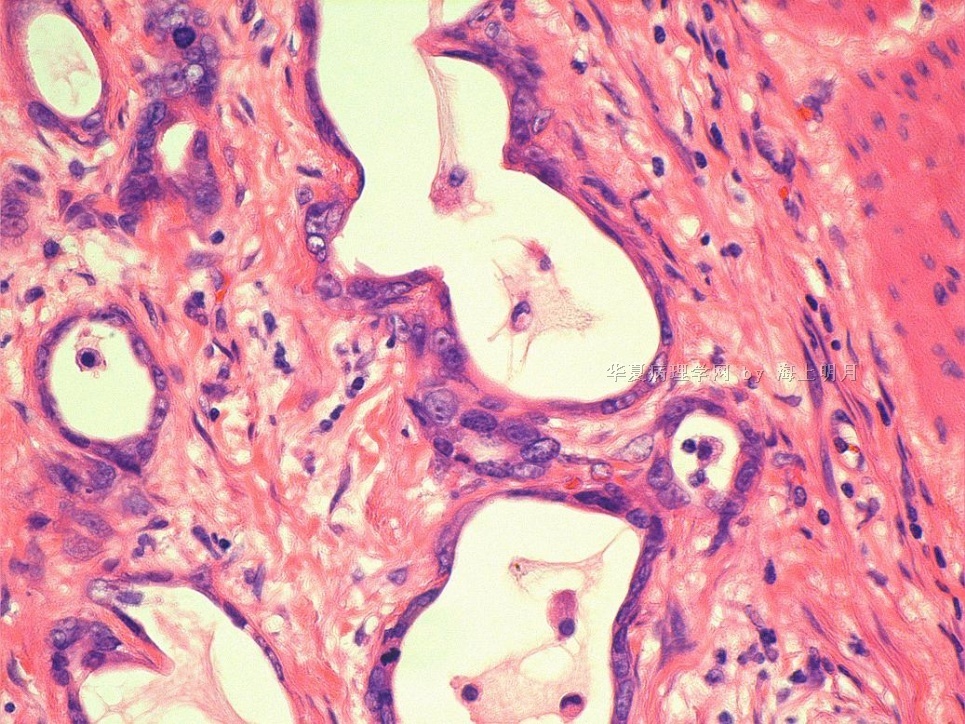
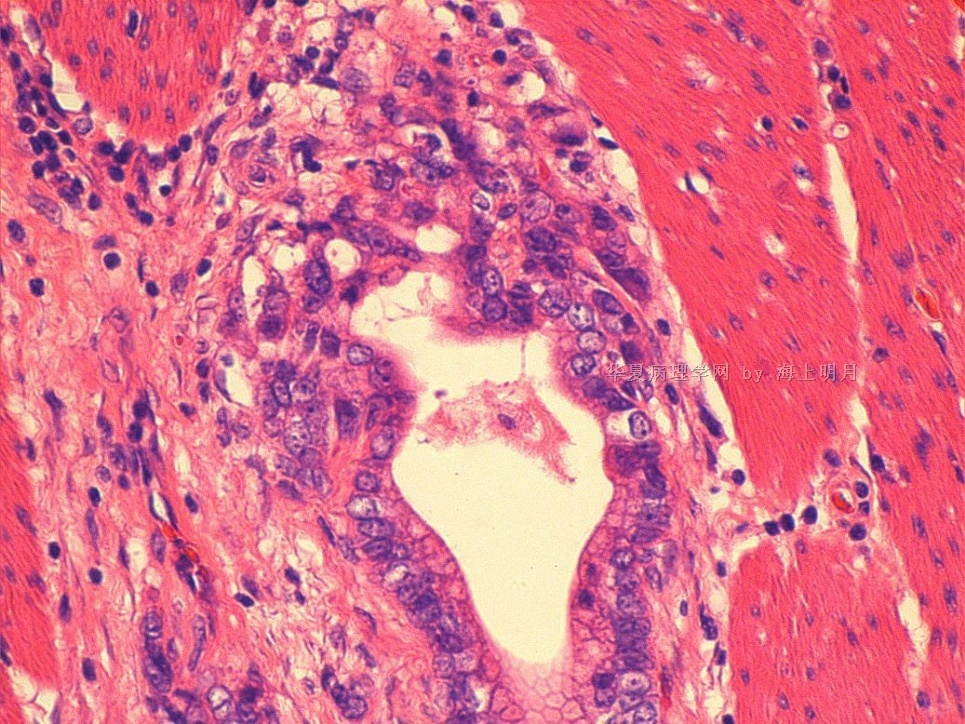
- 胃体小弯粘膜活检会诊病例(38楼大标本,58-59楼组织学。胃型(幽门腺型)腺癌?)
| 以下是引用天山望月在2010-6-21 9:54:00的发言:
谢谢海上明月老师提供文献摘要及翻译!受益了。 还有个问题想请教:新近发现的MUC 基因编码的粘蛋白核心蛋白,通过检测可以鉴别腺瘤和癌吗?我查全文看看。
|

- 王军臣
| 以下是引用海上明月在2010-6-13 11:59:00的发言:
内镜见胃体小弯粘膜糜烂灶,活检见高级别上皮瘤变。异型增生腺体紧贴平滑肌组织。由于是活检组织,内镜下又没有见溃疡,活检出这样的平滑肌一般会是肥厚的粘膜肌,而不是真正的肌层。 当然,如果有溃疡存在,活检中见到累及肌层倒是有可能的。可是,本例没有溃疡,所以报告时要慎重为佳。 会诊意见:高级别上皮瘤变,见异型增生腺体贴近平滑肌组织,粘膜内癌不能除外。 |
谢谢王老师!
其实这样的病例很常见,有时令人头痛,内镜所见明显是癌的描述,但因取材表浅局限,报告不好发,忧郁不定,诊断不足或过诊断都不利,因此,赞同王老师的意见,要非常慎重,可加些修饰语:高级别上皮内瘤变或粘膜内癌,因组织表浅局限,请结合临床,以排除局部浸润。
不知当否?谢谢!
- 广州金域病理
| 以下是引用海上明月在2010-6-12 18:04:00的发言:
二者的治疗措施不一样。 粘膜内癌可采用微创治疗,即:内镜下粘膜切除。 而粘膜下及其更深的浸润癌需根治手术。
|
内镜活检标本常因取材局限表浅,诊断粘膜内癌,一部分病例做微创粘膜切除后病检,会见到浸润癌,因此活检标本诊断时要结合内镜下所见,以排除进展期癌。
个人浅见,谢谢赐教!
- 广州金域病理
大意译文如下:
从1985年证明胃型高分化腺癌发生于胃增生性息肉以来,一些学者对胃肠道上皮病变的表型表达进行了研究。新近发现的MUC 基因编码的粘蛋白核心蛋白,促进了胃肠道肿瘤表型表达的研究。胃型高分化腺癌的肿瘤分类最近已被接受,尤其是被日本和欧洲所接受。即便是内镜和组织病理诊断这种类型有困难,但因其生物学行为可能为高度恶性的,该类型腺癌已常成为临床病理研讨的主题。即便如此,所谓“胃腺瘤”常被认为是肠型扁平腺瘤。直到最近,胃型腺瘤才被认为是例外的情况。 胃型腺瘤理论上可分为胃颈-小凹型和幽门腺型,但实际上胃颈-小凹型腺瘤难以与胃颈-小凹型腺癌相鉴别。 2003 年,作者首次报告了对幽门腺腺瘤进行的系统性临床病理分析,结果表明其变化多样,并具有癌前病变性质。文献中复习和讨论了胃型高分化腺癌和幽门腺型息肉的临床病理及分子病理方面的内容。
- 王军臣
-
本帖最后由 于 2010-06-20 23:48:00 编辑
请见如下文摘:
Gastric Cancer. 2006;9(3):177-84.
Gastric-type well-differentiated adenocarcinoma and pyloric gland adenoma of the stomach.
Kushima R, Vieth M, Borchard F, Stolte M, Mukaisho K, Hattori T.
Since 1985, when gastric-type well-differentiated adenocarcinomas were demonstrated in hyperplastic polyps of the stomach, we have studied phenotypic expression in gastrointestinal epithelial lesions. The recent discovery of MUC genes coding core proteins of mucin has improved research on the phenotypic expression of gastrointestinal neoplasms. The disease entity of gastric-type well-differentiated adenocarcinoma has recently been accepted, especially in Japan and Europe. This entity has often become a clinicopathological subject of discussion, because its biological behavior is possibly highly malignant, in spite of the difficulty in making endoscopic and histopathological diagnoses. Even under these circumstances, the term "gastric adenoma" usually means flat adenoma of the intestinal type. Gastric-type adenomas have been regarded as exceptional until recently. Although gastric-type adenomas could theoretically be classified into foveolar type and pyloric-gland type, foveolar-type adenoma is, in practice, difficult to distinguish from gastric-foveolar-type adenocarcinoma. In 2003, we first reported systematic clinicopathological analyses of pyloric gland adenoma, demonstrating its unstable and precancerous nature. In this article, we review and discuss the clinicopathological and molecular pathological aspects of gastric-type well-differentiated adenocarcinomas and pyloric gland adenomas, mainly based on our published and unpublished data.
- 王军臣











