













| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- Lung mass FNA today Please join in the discussion
 图1
图1 图2
图2 图3
图3 图4
图4 图5
图5 图6
图6
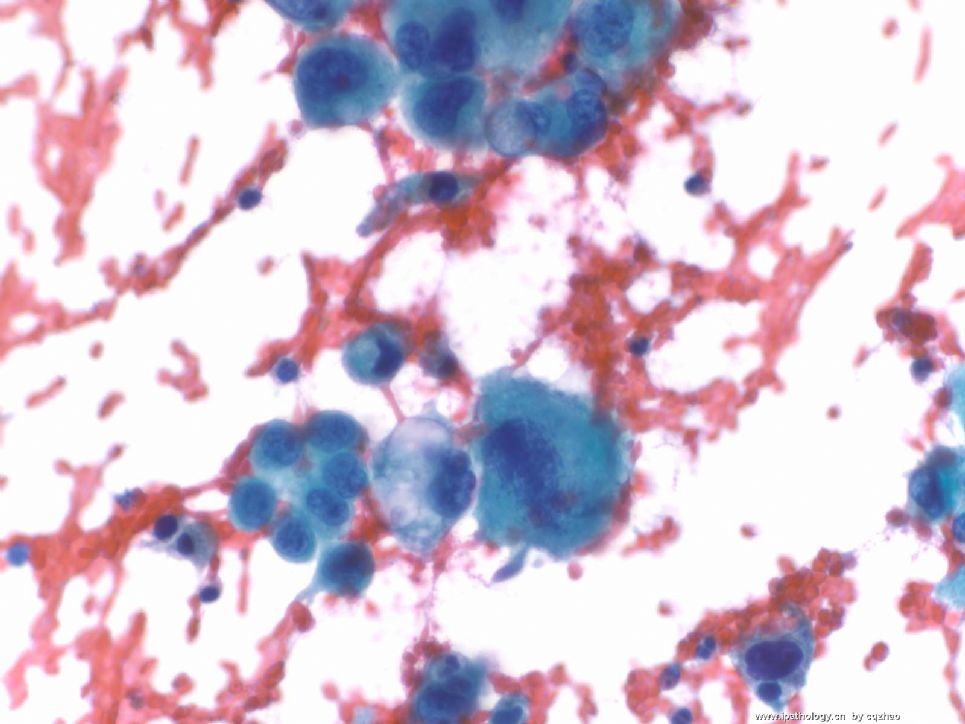
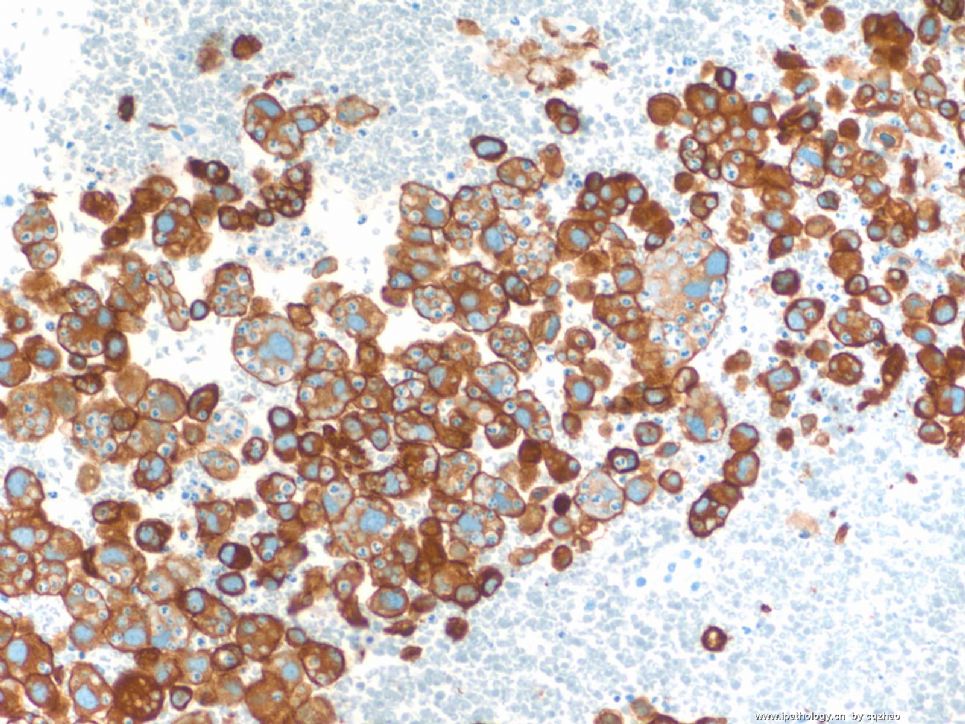
Old man with a lung mass 3 cm.
Radiologist did CT-guided FNA and I did on site evaluation this afternoon. I called malignant cells based on above one DQ. The procedure was stopped because patient had bleeding and also I think I should have enough cells for a cell block. Cytopathologists are required to give diagnosis (at least malignant, atypical, benign) on site in our institute if it is possible.
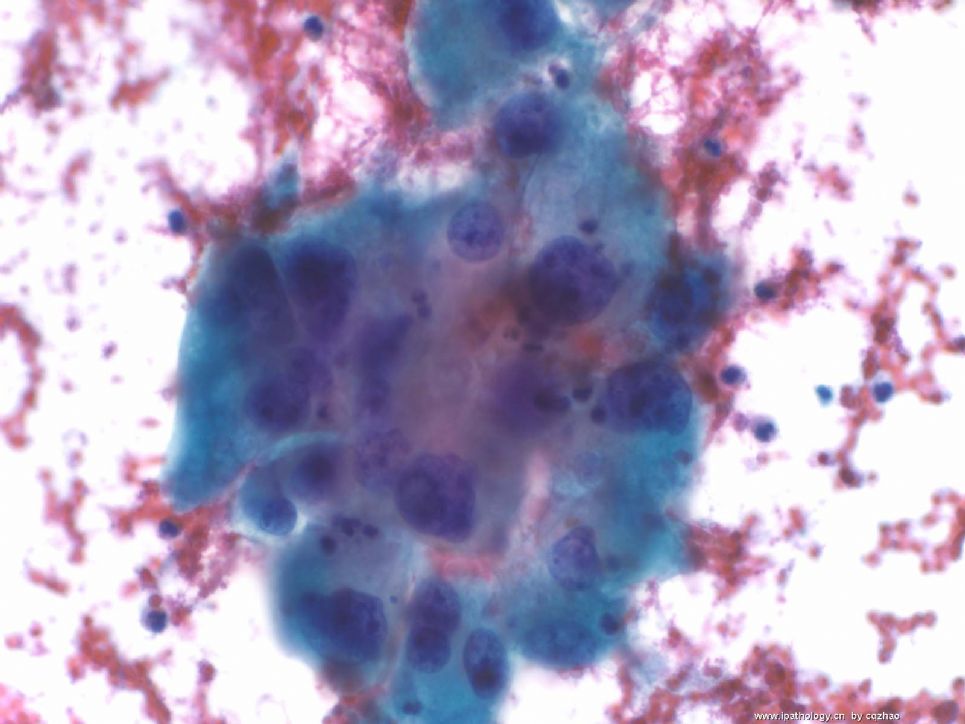
In fact I really do not know what kinds of tumor for this case. I have not seen the Pap stain yet. I have my differential dx and ordered some IHC already.
Hope people who see this case write down your differential dx and IHC.
When I have IHC results I will put here.
标签:
×参考诊断
低分化非小细胞癌
-
本帖最后由 于 2008-12-02 18:19:00 编辑
| 以下是引用cqzhao在2008-12-2 12:24:00的发言:
|
回Dr.cqzhao:如果想把更多的相片放1楼,请点编辑,继续上传就好了。
如果在回帖中放相片,先打几个字发表,然后点编辑再上传就好。
如果还不行,可能是网络问题,我发信息给坛主或管理员,请他们解决。
请Dr.cqzhao先喝杯茶,休息一下!

- 广州金域病理
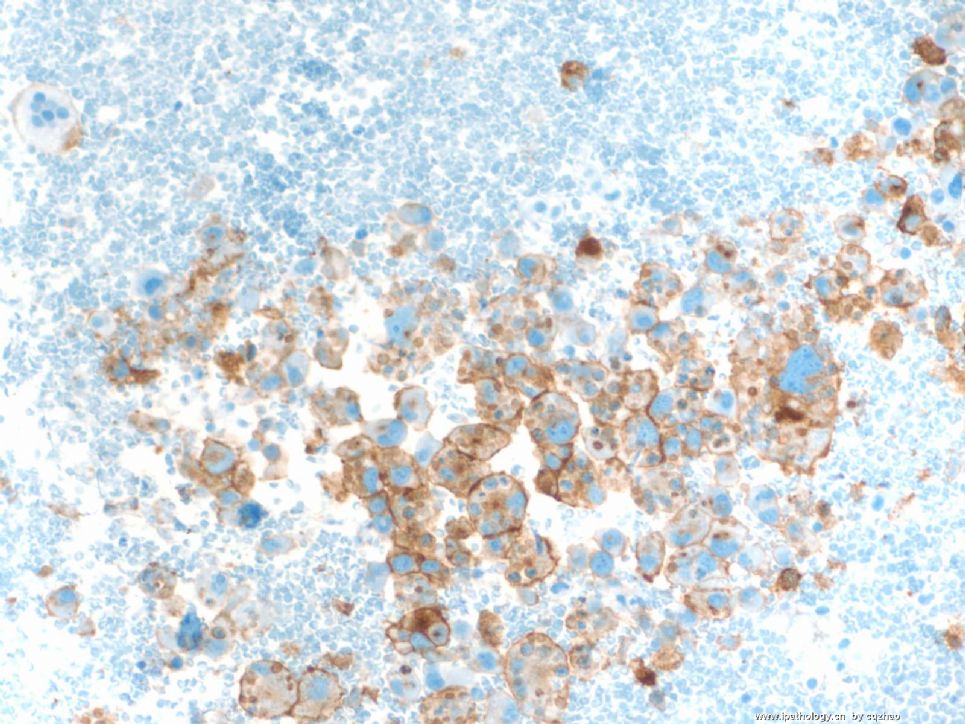
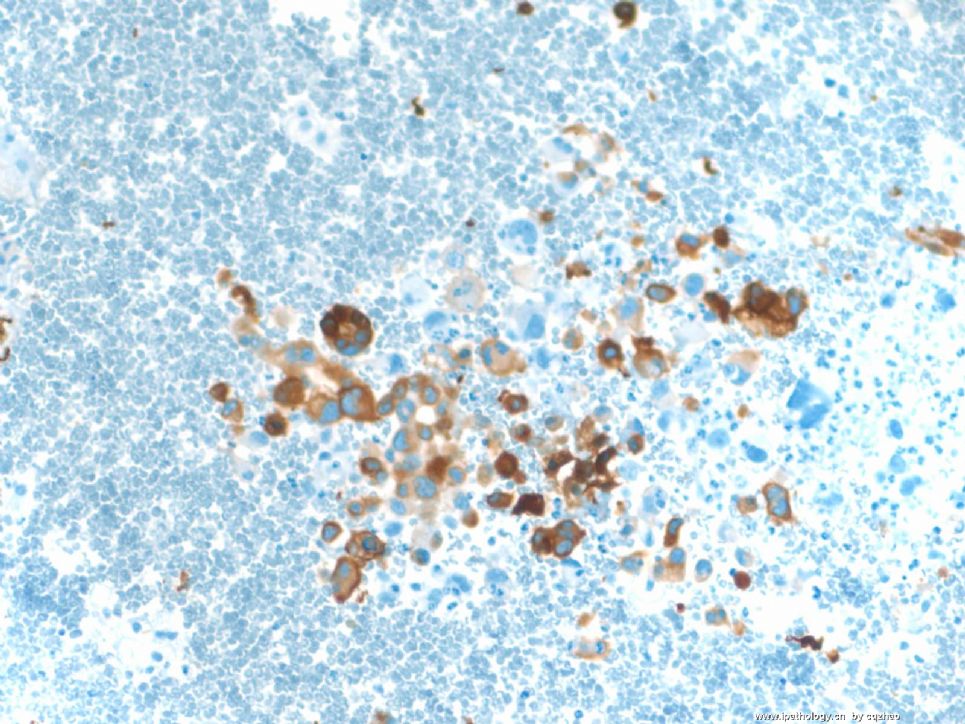
Other IHC:
Negative: TTF1, CK20, EMA, RCC, S-100, HMB45, Melan A, LCA
Previous neck mass is a consult case and no slides available for review. Imaging study indicated no kidney lesions. Interesting to know how you sign out this case. Hope more people in China to join.
-
本帖最后由 于 2008-12-03 23:33:00 编辑
谢谢Dr.cqzhao!非常经典的病例!
新传21楼的图片,有腺样排列,有粘液样胞浆。
试着分析IHC:
HMB45, Melan A, S-100阴性,排除恶黑,
LCA阴性排除淋巴造血疾病?!
TTF1排除甲状腺癌转移.
CA9,CD10,PanCK,vimentin阳性,考虑肾透明细胞癌转移!?RCC 阴性?
与肺原发的透明细胞癌怎样鉴别?
CD7阳性,不知怎么解释?是否需排除胸腺癌?
呵呵,我的问题较多,请专家赐教!谢谢!
- 广州金域病理
I would sign out this case using generic term, such as Non-small cell type carcinoma and then put a comment saying reviewing the patient's previous head&neck slides will be helpful, also ask the clinician to correlate clinically.
In our hospital (Cleveland Clinic), the oncologists are very understanding the limitations of pathology, if the lung has multiple nodules and they highly suspect metastasis, they will get the previous slides to you and do a "whole body" CAT scan. If there is only a single mass and the body scan is negative, they may just treat this as a primary lung Ca.
Thanks for sharing this case!











