








| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- Lung mass FNA today Please join in the discussion
 图1
图1 图2
图2 图3
图3 图4
图4 图5
图5 图6
图6
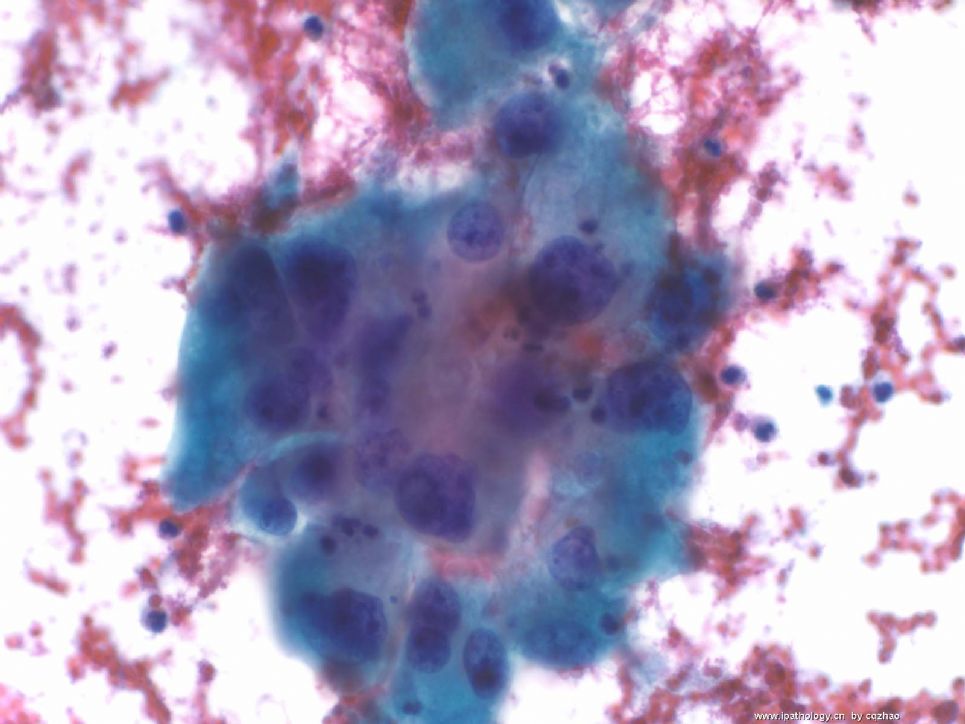
Old man with a lung mass 3 cm.
Radiologist did CT-guided FNA and I did on site evaluation this afternoon. I called malignant cells based on above one DQ. The procedure was stopped because patient had bleeding and also I think I should have enough cells for a cell block. Cytopathologists are required to give diagnosis (at least malignant, atypical, benign) on site in our institute if it is possible.
In fact I really do not know what kinds of tumor for this case. I have not seen the Pap stain yet. I have my differential dx and ordered some IHC already.
Hope people who see this case write down your differential dx and IHC.
When I have IHC results I will put here.
标签:
×参考诊断
低分化非小细胞癌
Thank Dr. 天山望月 and 月新' s great translation.
Conventional RCC=clear cell RCC, most common type of RCC: most cases are CK7 negative, occasional cases can be CK7 negative.
Papillary RCC: most of cases are CK7 positive as Dr. Chen has mentioned..
GU pathology=genitourinary pathology
GI pathology=gastrointestinal pathology
Sorry to cause the confusion.
Thank Dr. Chen, 天山望月's discussion and 月新老师的翻译.
I put this topic here for 2 weeks already. I hope my colleagures in China can join the discussion. In fact it seems that I and dr chen are main persons in discussion here. We do not need to put cases here if we want to discuss some cases. You need to be more active if you think you are weak and want to learn cytopathology.
Anyway I summarize the case now.
i sign out the case as following:
FINAL DIAGNOSIS:
Lung Mass, left, CT-Guided Fine Needle Aspiration Biopsy"
SATISFACTORY FOR INTERPRETATION.
POSITIVE FOR MALIGNANT CELLS.
POORLY DIFFERENTIATED NON-SAMLL CELL CARCINOMA (SEE COMMENT).
COMMENT:
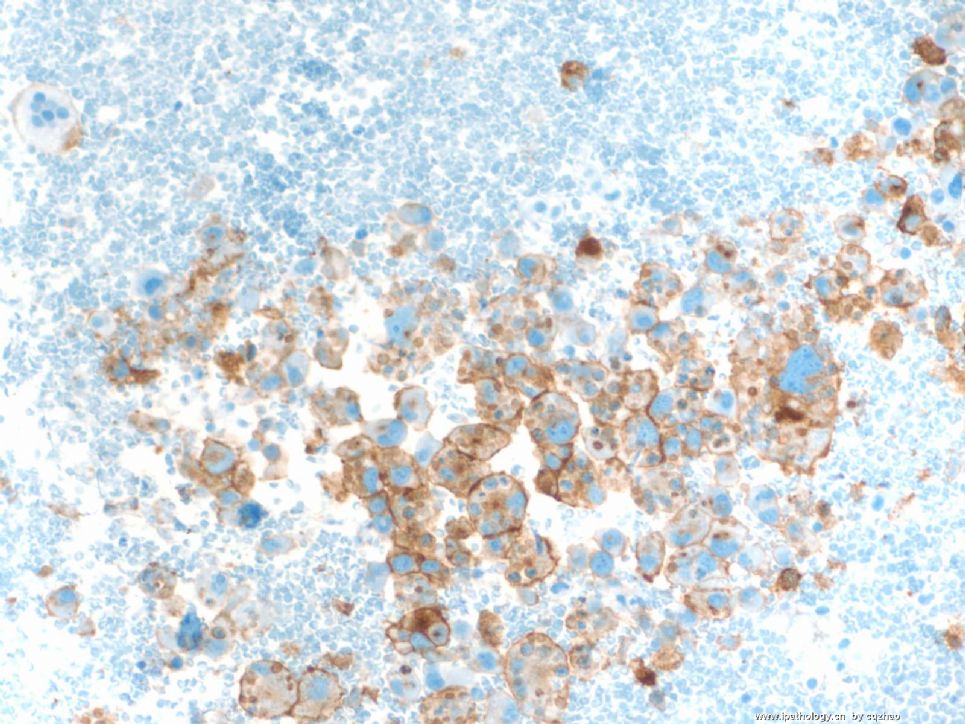
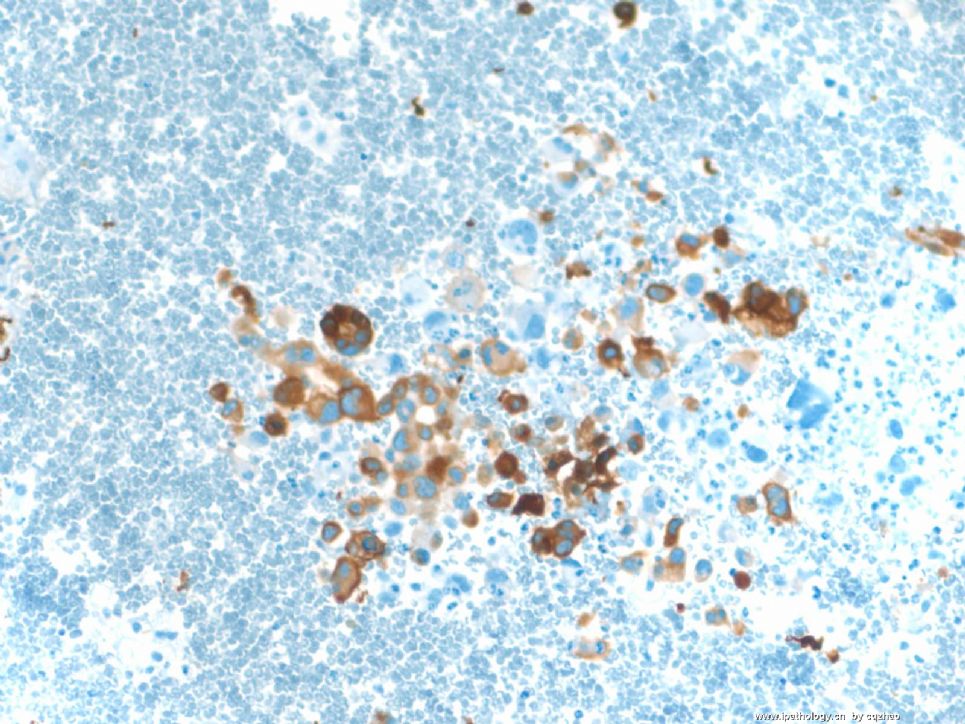
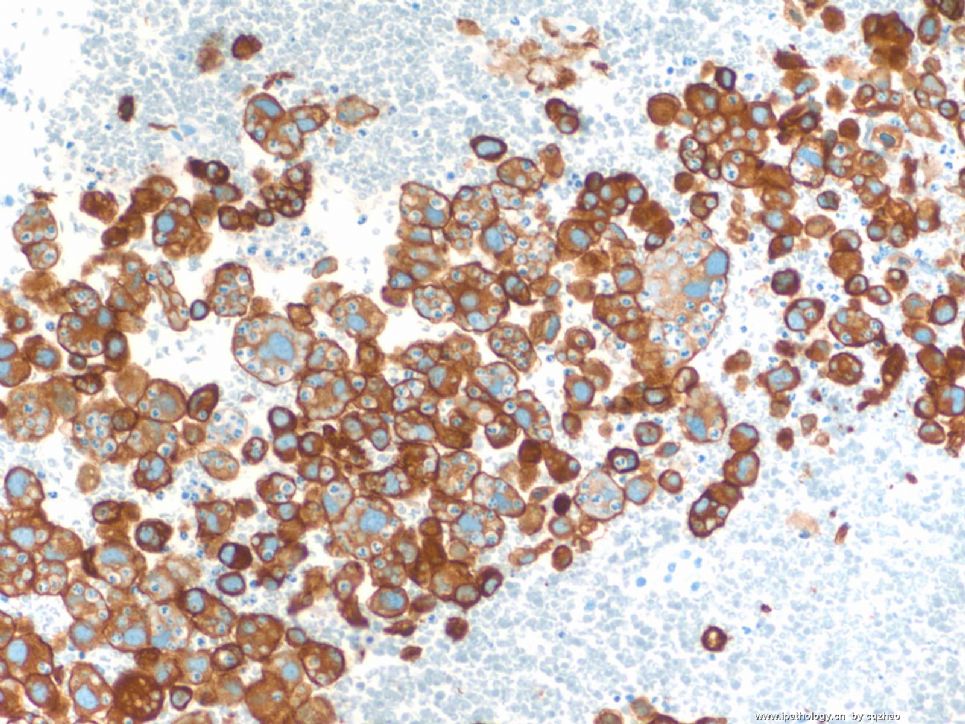
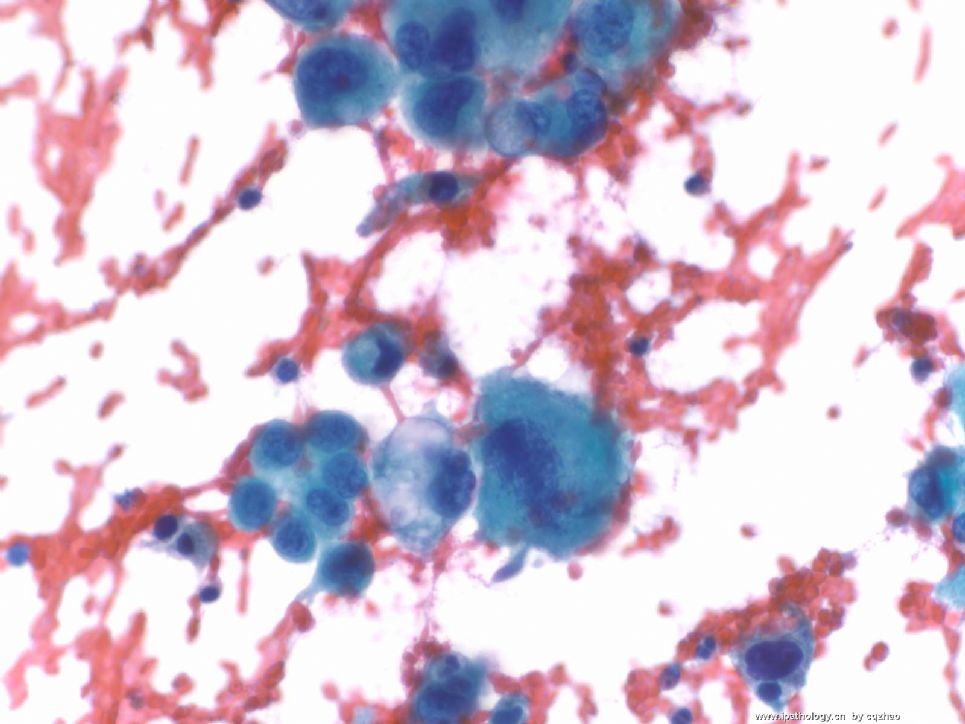
The aspiration smears are cellular and reveal single and dyschhesive clusters of malignant cells in a blood background. The tumor cells are large in size, very pleomorphic, and have abundant, vacuolated to dense cytoplasm, and hyperpchromatic nuclei with irregular contours and prominent nucleoli. Cell block contains similar cells with smears. To further cahracterize the tumor cells, immunohistochemical studies were performed on the cell block sections with the following results.
Lists of all the IHC results (I have mentioned above)
Combined the cytomorphologic and immunophenotypic findings are of a poorly differentiated non-small cell carcinoma. The immunoprofile of this lesion is similar to the neck mass (case No) and this may represent similar or same tumor. No slides of previous case are available for review. The differential diagnosis includes but is not limited to poorly differentiated adenocarcinoma of lung or metastatic carcinoma from nasopharyngeal origin, upper gastrointestinal origin including esophagus, stomach, pancreatobillary sites. In review of CA9, vimentin, and CD10 immunostain positivity in the present cells, it raises the possibility of metastatic renal cell carcinoma. Clincal correlation with imaging is recommedded.
I discussed the case with Dr. xxxx (primary physician) at 3:30 PM, on m/d/y.
Dr. xxxxx (cytopathologist) and Dr. xxx (GU pathologist) have reviewed the case and concur with above interpretation.
Above is present in my full final report.
Share some thought with you guys:
Previous surgical specimen is a neck mass diagnosed as poorly differentiated carcinoma. The origin of the neck mass was not known. I do not think the review of these slide can help me and this why I did not ask for these slides. This is complicated case and I cannot figure out the origin on FNA. It is fine that people know the limitation of the FNA cytology and even surgical pathology. In fact I will choose metastatic RCC if this is test, but not a true case.
Support RCC:
1.Multiple locations of metastasis
2.Cytologic features (even though the cytology of most RCC cases is not so ugly).
3. IHC results: positive for CD10, vimentin, CA9. CK7 is positive for papillary RCC. CK7 is negative in most conventional RCC cases, but some conventional cases can be positive. We cannot rule out RCC based on the positive CK7.
I feel unconfortable about RCC
The clinician said no lesion in kindey in imagining result.
I do not understand what carcinomas can be EMA purely negative.
Anyway this is what I can do for this case.
Suggest to you:
1. Know the limitation of cytopath and pathology.
2. Do not need to make a definite dx if you are not sure. Leave some spce for you.
3. Contact with the primary doctors to know the clinical information, let him know your interpretation. Record the comunication in your final report for some difficult case.
4. Show your case with other pathologists for some difficult cases and record in your report.
Thank for reading and discusing the case.
Other IHC:
Negative: TTF1, CK20, EMA, RCC, S-100, HMB45, Melan A, LCA
Previous neck mass is a consult case and no slides available for review. Imaging study indicated no kidney lesions. Interesting to know how you sign out this case. Hope more people in China to join.
Thank Dr. Chen's analysis. Pt has hx of ENT carcinoma. I asked the cytofellow to find surgical slides to review. My initial differeential dx includes sarcoma and carcinoma (especial RCC and squamous ca based on the hx even though the morphologic features do not look like). Some IHC stains I ordered on site have completed. I have not read them yet. I was in a shadysite cancer center for FNA last week and come back Magee this week. The fellow told me that epithelial markers are positive (PanCK, CK7), squamous markers and TTF1 are negative, vimentin and CD10 positive, EMA negative. I called the primary doctor and told him it is a carcinoma. I ordered more IHC and will review the initial stains tomorrow. Now my differential diagnoses are metastatic RCC (no any history) and metastatic poorly differential nasopharygeal ca. How do I know it is not a lung primary tumor? I will reveiw the original ENT tumor and think more how to signout the case finely.
I will like you know when I have more information.
To pathologists in China:
You see FNA cytology is interesting.











