
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图1")
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图2")
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图3")
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图4")
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图5")
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图6")
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图7")
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图8")
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图9")
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图10")
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图11")
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图12")
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图13")
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图14")
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图15")
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图16")


| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- NP (6) - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..
-
These photos are taken from brain, spinal cord, nerve roots, and dorsal root gangia removed from a 59 year-old woman at autopsy. All sections were stained by the luxol fast blue/H&E method. The patient experienced worsening numbness and weakness of lower extremities with difficulty walking for 6 months prior to death due to pneumonia and secondary sepsis. Left sural nerve biopsy and gastrocnemius muscle biopsy prior to death showed severe axonal neuropathy and chronic neurogenic atrophy, respectively. Brain MRI was normal. What is your diagnosis?
 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图1") 图1
图1 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图2") 图2
图2 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图3") 图3
图3 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图4") 图4
图4 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图5") 图5
图5 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图6") 图6
图6 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图7") 图7
图7 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图8") 图8
图8 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图9") 图9
图9 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图10") 图10
图10 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图11") 图11
图11 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图12") 图12
图12 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图13") 图13
图13 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图14") 图14
图14 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图15") 图15
图15 - Paraneoplastic encephalitis and sensory polyneuropathy associated with small cell carcin..图16") 图16
图16
1. Left frontal lobe neocortex
2-3. Left transentorhinal cortex
4. Substantia nigra
5. Nucleus of oculomotor nerve (midbrain)
6. Cerebellar cortex
7-8. Cerebellar dentate nucleus
9. Basis pontis
10-11. Inferior olivary nucleus of medulla oblongata
12. Lumbar spinal cord
13. Anterior nerve root (lumbar)
14. Posterior nerve root (lumbar)
15-16. Lumbar dorsal root ganglion
标签:
-
本帖最后由 于 2007-01-22 11:31:00 编辑

聞道有先後,術業有專攻
×参考诊断
-
zhongshihua 离线

- 帖子:1608
- 粉蓝豆:0
- 经验:1651
- 注册时间:2006-09-11
- 加关注 | 发消息
马老师讲解的非常好,译文如下:Paraneoplastic syndromes are diseases caused indirectly by the presence of malignancy. 副肿瘤综合征是由恶性肿瘤间接引起的一种病征。They are the results of hormones or cytokines elaborated by cancer cells, or of the body's immune response to cancer cells.是由癌细胞产生的激素或细胞激酶升高造成,或因机体对癌细胞的免疫反应所致。 Sometimes, paraneoplastic syndromes are the first signs of cancer (i.e., before the cancer is diagnosed).有时副肿瘤综合征是肿瘤的首发症状,发现肿瘤之前,先出现了副肿瘤综合征。The types of cancer involved are not disease-specific. 肿瘤的类型并非特定的, Lung (both small cell and non-small cell types), ovarian and breast cancers are the common offenders, but cancers of many other organs have been reported.肺的小细胞癌和非小细胞癌都可引起副肿瘤综合征,卵巢和乳腺癌也可引起,其它部位的恶性肿瘤引起副肿瘤综合征也有报告。There are four categories of paraneoplastic syndromes - hematological, neurological, mucocutaneous, and endocrine/metabolic. 副肿瘤综合征累及四个系统,造血系统,神经系统,粘膜皮肤和内分泌和代谢系统。Neurological paraneoplastic syndromes may affect the central and/or the peripheral nervous systems.可累及神经系统的中枢神经和周围神经, Many neurological paraneoplastic syndromes or disorders are caused by autoimmune mechanisms, with cancer-induced circulating autoantibodies directed against functional components at various parts of our nervous system. 许多神经系统的副肿瘤综合征可因免疫机制引发,癌细胞产生的自体免疫抗体进入血液,直接作用于不同部位的功能性神经组织。These functional elements include neurons and proteins on cellular surface. 这些功能性神经组织包括神经元和神经元表面的蛋白。Depending on their locations and functions, different neurological disorders arise. 因受累部位和功能不同副肿瘤综合征的病征也不同。 Some examples are listed below. 具体例子如下:
1. Limbic system (hippocampus/medial temporal cortex) - seizures, acute or subacute dementia (limbic encephalitis)
1、边缘系受累(海马/中颞叶皮质),引起眩晕,急性或亚急性的痴呆(边缘性脑炎)。
2. Brainstem - cranial nerve palsy, seizures, sudden death (brainstem encephalitis)
2、脑干受累-,引起颅神经麻痹,眩晕,突然死亡(脑干脑炎)。
3. Cerebellar Purkinje cells - ataxia (cerebellitis)
3、小脑Purkinje细胞受累:共济失调(小脑炎)。
4. Spinal cord - pain and weakness (myelitis)
4、脊髓受累:疼痛和软弱无力(脊髓炎)
5. Posterior root ganglia - pain and numbness (ganglionitis and sensory neuropathy)
5、脊髓后根神经节受累:疼痛和麻木(神经节炎和感觉性神经病)
6. Myelin sheaths of nerve fibers - numbness and weakness (demyelinating sensorimotor polyneuropathy)
6、神经纤维髓鞘受累:麻木和软弱无力(脱髓鞘性感觉运动多神经病变)
7. Calcium channel at neuromuscular junction - muscle weakness (Lambert-Eaton myasthenic syndrome)
7、神经肌肉联接Calcium channel受累:肌软弱无力(肌无力综合征)
8. Voltage-gated potassium channel on neurons - persistent muscular contraction (neuromyotonia), excessive sweating, sleep disorder, memory loss, hallucinations and delusions
8、神经元的Voltage-gated potassium channel受累:持续性肌肉收缩(神经性肌痛),过度出汗,睡眠障碍,记意丧失,幻觉和幻想。
9. Endothelial cells in skeletal muscle and dermis - skin rashes and muscle weakness with inflammation (dermatomyositis)
9、横纹骨和皮肤的血管内皮细胞受累:皮肤红斑和肌无力伴炎症(皮肌炎)
From the list above, it is not difficult to realize that manifestations of paraneoplastic neurological disorders vary from case to case and often mislead clinicians. 综上所述,认识副肿瘤综合征的神经系统病变并不难,但是因人而已,差异很大,临床经常误诊。Since circulating autoantibodies are often present in the serum of these patients, screening for them may occasionally be diagnostic. 患者的血中常常含有自身抗体,筛查偶尔也可确诊。However, only a portion of targeted cells and proteins has been characterized so screening results are often false negative.但是,因蛋白和靶细胞的部位十分特殊,筛查常为阴性。 Biopsy of tissue before death is often non-diagnostic since pathology is non-specific and often very focal. 病理改变是非特异性的,局灶性的,生前活检经常不能确诊,Often the final diagnosis is rendered by a complete autopsy. 多数经尸检确诊。Fortunately, empiric (but expensive) therapy with plasmapheresis and/or IVIg may result in dramatic alleviation of the symptoms and, if implemented early, may even promise partial functional recovery. 幸运的是,用plasmapheresis and/or IVIg治疗的早,可以明显的减轻症状,恢复部分功能。A high index of clinical suspicion, thorough oncologic workup, and complete resection, effective radiation therapy or chemotherapy of the cancer found often is curative for the associated paraneoplastic syndrome.如果临床高度可疑并且发现了肿瘤,完全切除肿瘤,或有效放疗,化疗,可以治愈副肿瘤综合征
Paraneoplastic syndromes are diseases caused indirectly by the presence of malignancy. They are the results of hormones or cytokines elaborated by cancer cells, or of the body's immune response to cancer cells. Sometimes, paraneoplastic syndromes are the first signs of cancer (i.e., before the cancer is diagnosed). The types of cancer involved are not disease-specific. Lung (both small cell and non-small cell types), ovarian and breast cancers are the common offenders, but cancers of many other organs have been reported.
There are four categories of paraneoplastic syndromes - hematological, neurological, mucocutaneous, and endocrine/metabolic. Neurological paraneoplastic syndromes may affect the central and/or the peripheral nervous systems. Many neurological paraneoplastic syndromes or disorders are caused by autoimmune mechanisms, with cancer-induced circulating autoantibodies directed against functional components at various parts of our nervous system. These functional elements include neurons and proteins on cellular surface. Depending on their locations and functions, different neurological disorders arise. Some examples are listed below.
1. Limbic system (hippocampus/medial temporal cortex) - seizures, acute or subacute dementia (limbic encephalitis)
2. Brainstem - cranial nerve palsy, seizures, sudden death (brainstem encephalitis)
3. Cerebellar Purkinje cells - ataxia (cerebellitis)
4. Spinal cord - pain and weakness (myelitis)
5. Posterior root ganglia - pain and numbness (ganglionitis and sensory neuropathy)
6. Myelin sheaths of nerve fibers - numbness and weakness (demyelinating sensorimotor polyneuropathy)
7. Calcium channel at neuromuscular junction - muscle weakness (Lambert-Eaton myasthenic syndrome)
8. Voltage-gated potassium channel on neurons - persistent muscular contraction (neuromyotonia), excessive sweating, sleep disorder, memory loss, hallucinations and delusions
9. Endothelial cells in skeletal muscle and dermis - skin rashes and muscle weakness with inflammation (dermatomyositis)
From the list above, it is not difficult to realize that manifestations of paraneoplastic neurological disorders vary from case to case and often mislead clinicians. Since circulating autoantibodies are often present in the serum of these patients, screening for them may occasionally be diagnostic. However, only a portion of targeted cells and proteins has been characterized so screening results are often false negative. Biopsy of tissue before death is often non-diagnostic since pathology is non-specific and often very focal. Often the final diagnosis is rendered by a complete autopsy. Fortunately, empiric (but expensive) therapy with plasmapheresis and/or IVIg may result in dramatic alleviation of the symptoms and, if implemented early, may even promise partial functional recovery. A high index of clinical suspicion, thorough oncologic workup, and complete resection, effective radiation therapy or chemotherapy of the cancer found often is curative for the associated paraneoplastic syndrome.
聞道有先後,術業有專攻
-
本帖最后由 于 2007-01-22 22:10:00 编辑
马老师的帖子太好了,给我们学习的机会.我译文如下
|
This is a rare case of paraneoplastic (autoimmune) encephalitis and sensory polyneuropathy caused by undiagnosed metastatic small cell carcinoma in the mediastinum, most probably of pulmonary origin.本例是罕见病例,纵隔转移性小细胞癌(可能是肺癌转移)引起的副肿瘤性脑炎(自体免疫性疾病)和感觉性多神经性病.Photos uploaded in the first batch reflect the extent of inflammation in the central nervous system, and degeneration of the spinal cord and the peripheral nervous system. 第一次上传的图片显示广泛性的中枢神经系统炎症,脊髓和外周神经系统的退变.Figures 1 and 6 show normal frontal lobe isocortex and normal cerebellar cortex (including intact Purkinje cells that often are targets of paraneoplastic or autoimmune encephalomyelitis) without inflammation. 图1和图6显示正常的同侧额叶皮质和正常的小脑皮质,(包括完整的Purkinj细胞,这些细胞常常做为副肿瘤脑炎或自身免疫性脑炎的靶细胞),首次给的图片中这些Purkinje细胞并没有炎症.Figures 2-3 show perivascular inflammation and microglial nodules in transentorhinal cortex (medical temporal lobe) indicative of active mesial temporal encephalitis.图2和图3显示 颞叶皮质血管外周炎症和微胶质结节形成,提示示为活动性中颞叶脑炎.Figures 4 and 6-11 show varying numbers of microglial nodules with or without neuronophagia in varying parts of the brainstem and cerebellum, indicative of active brainstem encephalitis and cerebellitis.图4和图6-图11显示脑干和小脑程度不同的微胶质结节,伴有或不伴有不同程度的噬节现象,提示为活动性脑干炎和活动性小脑炎。 Figures 12 shows degeneration (loss of blue myelin staining) of the posterior column of the spinal cord due to severe sensory polyneuropathy. 图12显示脊髓后根因严重的感觉多神经病造成的退变(髓鞘染色,箭头指蓝色明显缺少,表明髓鞘脱失)。Figure 13 shows relatively normal anterior spinal nerve root (motor), and Figure 14 shows the markedly degenerated posterior spinal nerve root (sensory). 图13显示脊神经前根(运动)相对正常的髓鞘染色,蓝色的髓鞘正常存在,图14显示脊神经后根(感觉)明显退变,髓鞘染色,蓝色的髓鞘明显减少。Note the abundant myelinated nerve fibers in the former and relatively few remaining myelinated nerve fibers in the latter. 图片提示脊神经前根有较多的有髓神经纤维,而脊神经后根有髓神经纤维明显减少。Figures 15 and 16 show many small lymphocyte-like cells in the posterior root ganglia, suggestive of active ganglionitis, but immunohistochemical stain (not shown) shows these cells to be negative for CD45. 图15和图16显示脊神经后根的神经节有许多小淋巴样细胞(箭头),提示为活动性神经节炎,但是,免疫组化染色这些小淋巴样细胞CD45阴性。Therefore, they probably represent satellite cells normally present around ganglion cells in dorsal root ganglia.因此,这些小淋巴样细胞可能是正常出现的围绕背神经节的卫星细胞。The four photos uploaded in the second batch are diagnostic of small cell carcinoma, most probably of pulmonary origin.第二次给的四副图诊断是小细胞癌可能来源肺。 |
-
本帖最后由 于 2007-01-22 11:32:00 编辑
This is a rare case of paraneoplastic (autoimmune) encephalitis and sensory polyneuropathy caused by undiagnosed metastatic small cell carcinoma in the mediastinum, most probably of pulmonary origin.
Photos uploaded in the first batch reflect the extent of inflammation in the central nervous system, and degeneration of the spinal cord and the peripheral nervous system. Figures 1 and 6 show normal frontal lobe isocortex and normal cerebellar cortex (including intact Purkinje cells that often are targets of paraneoplastic or autoimmune encephalomyelitis) without inflammation. Figures 2-3 show perivascular inflammation and microglial nodules in transentorhinal cortex (medical temporal lobe) indicative of active mesial temporal encephalitis. Figures 4 and 6-11 show varying numbers of microglial nodules with or without neuronophagia in varying parts of the brainstem and cerebellum, indicative of active brainstem encephalitis and cerebellitis. Figures 12 shows degeneration (loss of blue myelin staining) of the posterior column of the spinal cord due to severe sensory polyneuropathy. Figure 13 shows relatively normal anterior spinal nerve root (motor), and Figure 14 shows the markedly degenerated posterior spinal nerve root (sensory). Note the abundant myelinated nerve fibers in the former and relatively few remaining myelinated nerve fibers in the latter.
Figures 15 and 16 show many small lymphocyte-like cells in the posterior root ganglia, suggestive of active ganglionitis, but immunohistochemical stain (not shown) shows these cells to be negative for CD45. Therefore, they probably represent satellite cells normally present around ganglion cells in dorsal root ganglia.
The four photos uploaded in the second batch are diagnostic of small cell carcinoma, most probably of pulmonary origin.
聞道有先後,術業有專攻
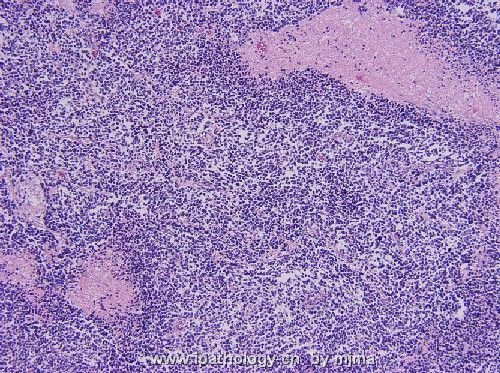
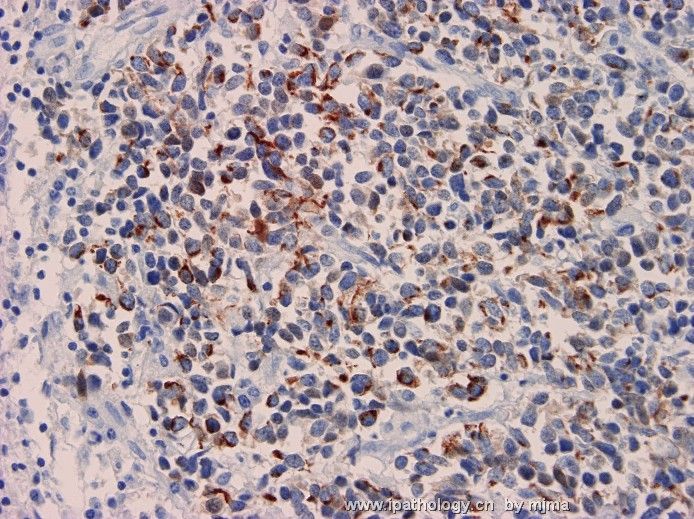
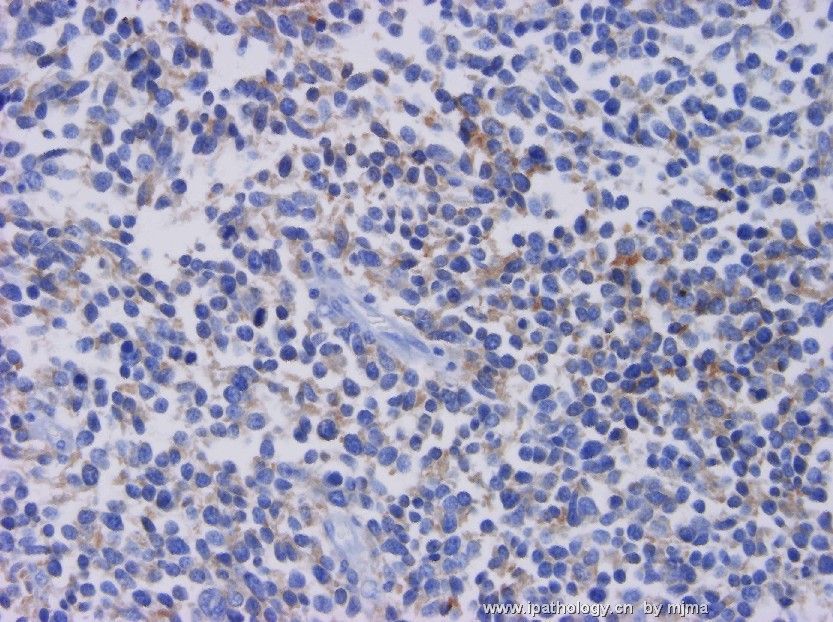
马老师译文如下: Sorry for this delayed follow-up. 抱欠,因随访延误回贴.At the autopsy, a 2 cm enlarged mediastinal lymph node was found. 尸检见纵隔有2cm肿大的淋巴结,No tumor was identified in both lungs or other organs. 肺和其它器官未见肿瘤生长,Figures 1 and 2 are H&E stained section of the enlarged mediastinal lymph node. 图1-2是纵隔肿大的淋巴结HE染色,Figure 3 is Cam5.2 immunostain, and figure 4 is synaptophysin immunostain. 图3是Cam5.2免疫组化,图4是synaptophysin免疫组化染色.With these additional findings, how would you explain the entire case? 加上这些图片,您考虑什么?请回答!
我也问马老师一个问题,第二次给的图片像是一个恶性肿瘤,根据您第一次给的图片敢诊断恶性肿瘤吗?那些箭头所指的是恶性细胞吗?
请马老师做最后分析.
-
Sorry for this delayed follow-up. At the autopsy, a 2 cm enlarged mediastinal lymph node was found. No tumor was identified in both lungs or other organs. Figures 1 and 2 are H&E stained section of the enlarged mediastinal lymph node. Figure 3 is Cam5.2 immunostain, and figure 4 is synaptophysin immunostain. With these additional findings, how would you explain the entire case?
 图1
图1 图2
图2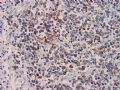 图3
图3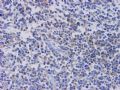 图4
图4
聞道有先後,術業有專攻











