
图1")
图2")
图3")
图4")
图5")
图6")
图7")
图8")







| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- 左大腿内侧皮肤发生的肿瘤-病理诊断的两难性(已有诊断结果和会诊意见)
图1") 图1
图1图2") 图2
图2图3") 图3
图3图4") 图4
图4图5") 图5
图5图6") 图6
图6图7") 图7
图7图8") 图8
图8
| 姓 名: | ××× | 性别: | 男性 | 年龄: | 65岁 |
| 标本名称: | 皮损结节 | ||||
| 简要病史: | 左大腿内侧皮损4年,明显增大半年。PE:皮损黑褐色,半球形。 | ||||
| 肉眼检查: | 梭形皮肤2.5x1x0.3cm,皮表灰褐色隆起高出皮表0.2cm,直径0.8cm,中央灰白色。切面灰褐灰白色。 | ||||
标签:
-
本帖最后由 于 2010-06-14 14:24:00 编辑

- 王军臣
×参考诊断
基底细胞癌伴毛囊分化。
-
本帖最后由 于 2010-06-13 22:56:00 编辑
MINI-SYMPOSIUM: CUTANEOUS EPITHELIAL TUMOURS
The use of immunohistochemistry in the differential diagnosis of common epithelial tumours of the skin
D.S.A. Sanders , a, and R.A. Carra
aDepartment of Pathology, Lakin Road, Warwick CV34 5BJ, UK
Available online 25 August 2007.
BerEP4
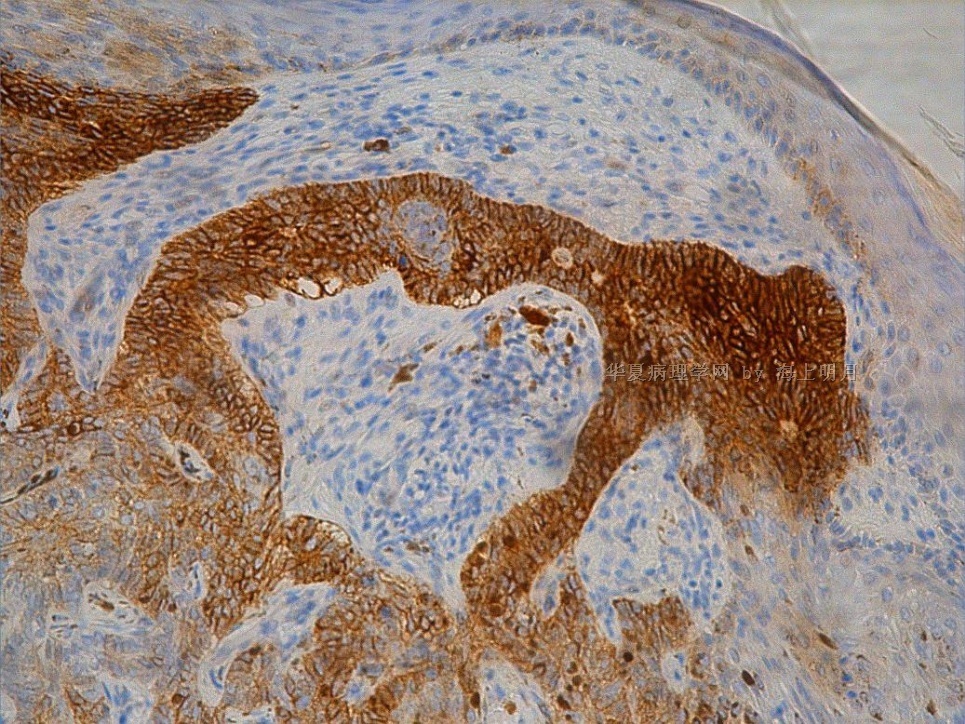
BerEP4 is a monoclonal antibody to a 34/49-kDa glycoprotein on the surface of most epithelial cells, with the exception of superficial layers of squamous epithelia.1 BerEP4 stains the vast majority of non-cutaneous epithelia and is highly conserved in the tumours derived from them, including non-cutaneous squamous cell carcinomas (SCC).1 In normal skin, there is reported positivity of the lower part of telogen hairs (secondary hair germ), matrix and outer root sheath (ORS) of vellus hairs, early anagen of terminal follicles (but not any part of mature anagen follicles), and the lower part of the epithelial strand of late catagen follicles.[2] and [3] Similar strong positive staining is seen in lining cells of eccrine and apocrine coils, with more variable staining of sweat duct lining cells and the acrosyryngium.3 F.J. Jimenez, J.L. Burchette Jr, J.M. Grichnik and M.G. Hitchcock, Ber-EP4 immunoreactivity in normal skin and cutaneous neoplasms, Mod Pathol 8 (1995), pp. 854–858. View Record in Scopus | Cited By in Scopus (32)3 The epidermis, follicular mantle, sebaceous glands and all non-epithelial tissues are negative[1] and [3] (Fig. 1A–C).
Figure 1. BerEP4 staining in normal skin and basal cell carcinoma (BCC): (A) weak staining in upper eccrine duct and acrosyryngium; (B) weak staining in lower sweat duct and strong staining in sweat gland coils; (C) outer root sheath telogen and anagen vellus buds (inset showing perifollicular Merkel cells); (D) nodular BCC; (E) metatypical and infiltrative BCC with weaker staining; (F) sebeorrhoeic keratosis (left side negative) in collision with superficial BCC; (G) fibroepithelioma of Pinkus; and (H) perineural invasion from a micronodular BCC.
Carcinoembryonic antigen
Carcinoembryonic antigen (CEA) is a glycoprotein initially described as a colonic oncofetal antigen,32 but subsequently shown to be expressed in a variety of normal human tissues33 including squames.34 Anti-CEA antibodies are now designated ‘CD66’ with a subclassification a–e depending on which epitope of the antigen is recognized. In normal skin, membranous CEA positivity can occasionally be seen in suprabasal squamous cells of the epidermis, and on the inner lining of sweat gland coils (including canaliculi), dermal ducts and acrosyringium.35 Monoclonal CEA can be used as a marker of ductal/glandular differentiation in skin tumours, and may also highlight mature squamous differentiation. However, in the authors’ experience, immunostaining is sometimes inconsistent and less sensitive for lumina than EMA.
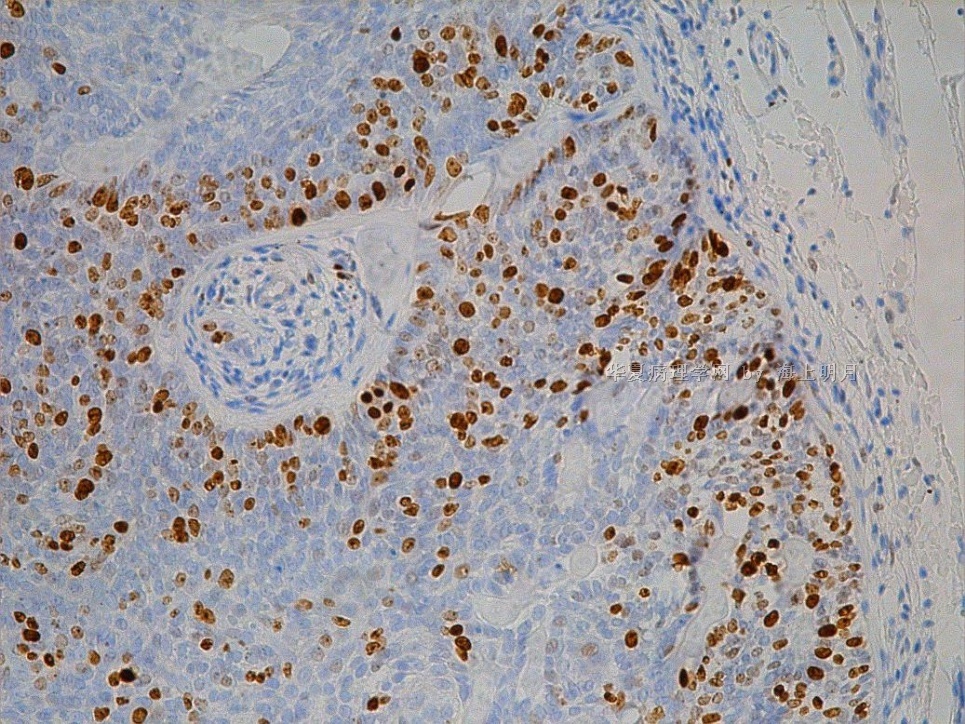
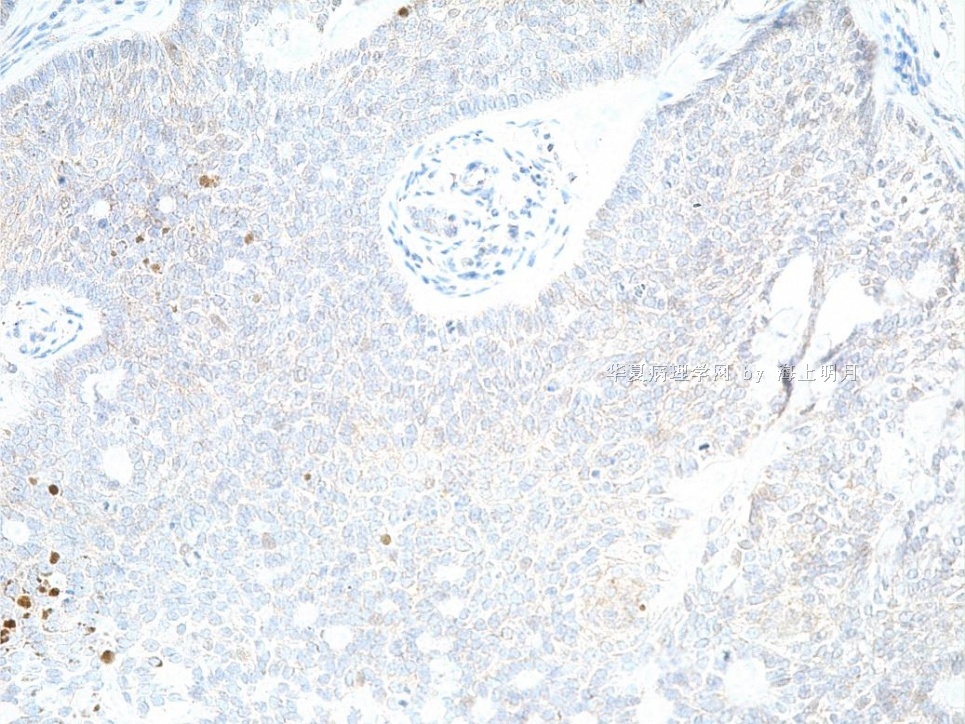
Bcl-2, p53 and Ki-67
Bcl-2 is an anti-apoptotic protein residing on the outer mitochondrial membrane. It is implicated in the pathogenesis of several common cancers by inhibiting programmed cell death. In normal skin, Bcl-2 stains the majority of keratinocytes in the basal epidermis, cells of the ORS, mesenchymal cells of the follicular papillae, and clear cells of eccrine glands.57 Diffuse cytoplasmic Bcl-2 expression is reported in BCC[57] and [58] and is reported to be useful in the distinction of BCC (diffuse staining) from TE (staining of basal layer only)59 and BCC and solar keratosis (latter negative).60
p53 is a tumour-suppressor gene and many p53 mutations result in a protein product that is unusually stable and becomes detectable by immunohistochemistry. Ultra-violet light is known to induce both overexpression of wild-type p53 and cause specific mutations in the p53 gene, and a discrepancy between cutaneous tumours with positive immunostaining and those with mutation has been reported.61 Nuclear accumulation of p53 protein is a feature of the majority of malignant adnexal and epidermal tumours including BCC,62 SCC and Bowen's disease,63 and is confined to the areas of basal atypia in solar keratosis.63 Hence, p53 immunostaining may have some utility in the differential diagnosis of intra-epidermal tumours (Fig. 7) and aids the distinction between basaloid proliferations (follicular induction) over dermatofibromas (rarely p53 positive) and the superficial subtype of BCC that they resemble.64 p53 immunostaining is of lesser value in differentiating benign from malignant skin tumours, as evidenced by similar staining patterns reported between BCC and TE, and eccrine poroma and porocarcinoma.[65] and [66]
|
Full-size image (175K) |
Figure 7. Clonal Bowen's: (A) low power of a clonal tumour and (B) high power showing uniform but atypical, acantholytic cells. Negative Cam5.2 is against extramammary Paget's and negative S100 against melanoma. p53 diffusely strongly positive.
Ki-67 (MIB 1) is a proliferation marker with a pattern of nuclear positivity. Demonstration of the proliferation index in skin tumours, in conjunction with the mitotic index, is used by many pathologists to help differentiate between benign and potentially malignant tumours. p53 positivity in conjunction with Ki-67 positivity is reported to be a feature of malignancy in the differential diagnosis of hidradenoma from hidradenocarcinoma, although histological parameters remain paramount.67
原文太长,截取部分,希望对大家分析有帮助,继续学习
续上篇
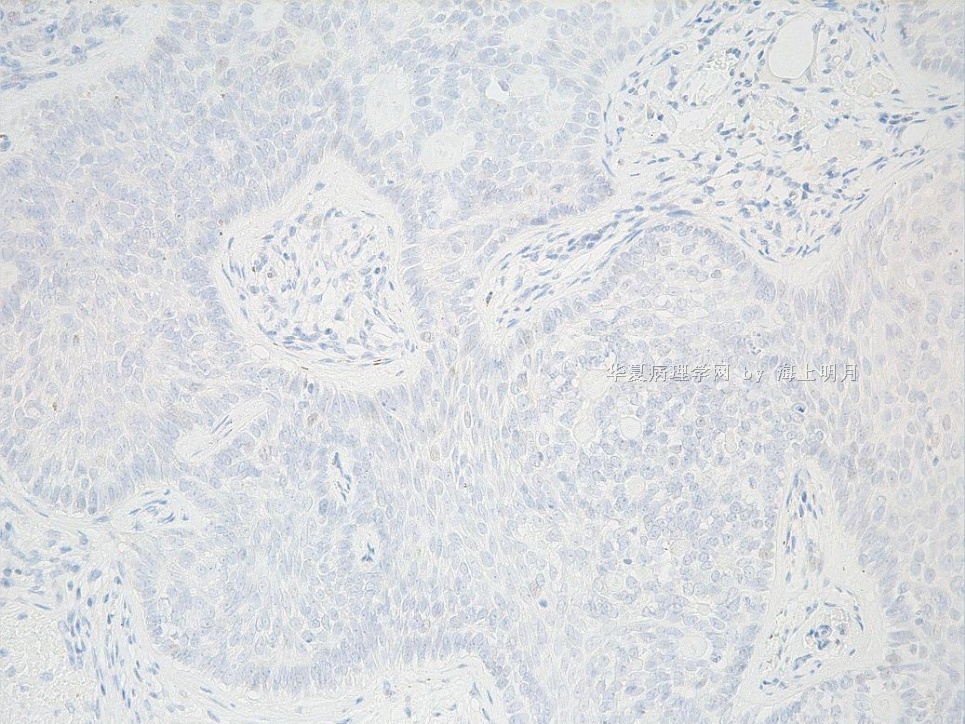
Basal cell carcinoma vs. trichoblastoma (trichoepithelioma)
Immunopanel—BerEP4, CD10, Bcl-2, CD34, CK20, Cam5.2
In trichoblastomas, CD10 typically highlights the peritumoral stroma, including papillary mesenchymal bodies, with minimal patchy staining of basaloid cells. In contrast, in BCC, the stroma is negative and basaloid cells variably strongly positive with CD10. Diffuse Bcl-2 positivity is reported in BCC, whereas the basal layer alone is highlighted in TE. The authors have found this to be variable and unreliable in practice. CD34 may highlight the peritumoural stroma in the desmoplastic variant of TE and not in infiltrative BCC, but this is also an unreliable finding in the authors’ experience. Merkel cells can be highlighted with Cam5.2 or CK20 and are absent from BCC but increased in number in trichoblastoma.
突击学习,本例形态学集中在基底细胞癌和毛母细胞瘤的鉴别。这两种瘤形态学相似,老师就其鉴别诊断的免疫组化分析提出问题,就BerEP4可以做为基底细胞肿瘤和鳞状细胞癌鉴别的重要marker,但是在基底细胞癌和毛母细胞瘤(Modern Pathology (2008) 21, 178–185; doi:10.1038/modpathol.3801000; published online 7 December 2007,57% of desmoplastic trichoepithelioma)中都有表达,
明天在学习继续写
- 文章:1151
- 积分:5660
- 经验:1247
- 注册:2007-1-31 18:12
这是一位网友对诊断的回答
|
| ||||||||
- 王军臣
- 文章:1290
- 积分:7265
- 经验:1608
- 注册:2009-3-4 3:39
这是金主任帮我回答了关于诊断的问题
|
| |||||||||
谢谢金主任!
- 王军臣











