
















| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- 头痛脑脊液检查
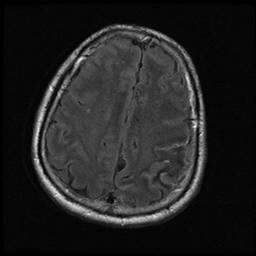
 图1
图1 图2
图2 图3
图3 图4
图4
Our fellow showed a case last week. I think it is interesting. Send here as a chinese new year gift for some ones interested.
about 50 y women with headach, CSF cytology exam. paitent has no previous malignant history.
标签:
-
本帖最后由 于 2010-02-13 10:36:00 编辑
×参考诊断
最后诊断:恶性黑色素瘤,结合临床,可能原发于脑膜。
-
本帖最后由 于 2010-03-30 03:58:00 编辑
Take home message:
l 1. Melanoma should be included in the differential diagnosis of CSF maligancy especially if no history
l2. Melanoma can be primary to leptomeninges in extremely rare cases
l3. Melanoma can be Bcl-2 positive
Melanoma cells in CSF:
l-Melanoma higher predilection for leptomeningeal metastasis (20%)
l-Meninges have Melanocytes!
l-Extremely rare primary (Melanosis Cerebri) 1%
l-If patient had Hx of melanoma, it is easy to say it is metastatic (straight forward)
-DDx: mainly Carcinoma, Lymphoma
For the case I mentioned above:
Cytopathologists asked clinician to get second time of CSF. It is a malignant melanoma based on IHC result and cytologic features (very calssic for both). Patient had no melanoma history, so it may be a primary melanoma of meninges.
This is a rare and interesting case. Occasionally I came here to check and notice no people who are truely interested to this case. I am not interested to continue to complete this case until Dr. 海上明月 asked me about this case.
In this section, I saw a lot of cases to show some atypical cells in pleural or peritoneal fluid. Questions are these cells are reactive mesothelial cells or malignant cells. In many situation we cannot answer the questions. We must do some basic stains, such as calretinin and BerEP4. This is the principle all residents should know. If we know they are malignant cells (most common adenocarcinoma), we should try to know the origins of the adenocarcinoma and provide more information to clinicians. This is our duty.
Do not use the terms too often, suggestive; may be; suspicious et al.
Quickly review above interpretation, suggestion, common.
We are pathologists. It is good for us to make some suggestion. However it is important for us to provide more information or more specific diagnosis for clinic.
For example we make the diagnosis, suspicous malignancy, ? metastatic adenocarcinoma et al. What do yo want to clinicians to do based on our cytology diagnosis.
Can we do some stains for this case?











