









 ^_^ O(∩_∩)O哈哈~ 谢谢!
^_^ O(∩_∩)O哈哈~ 谢谢! 




| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
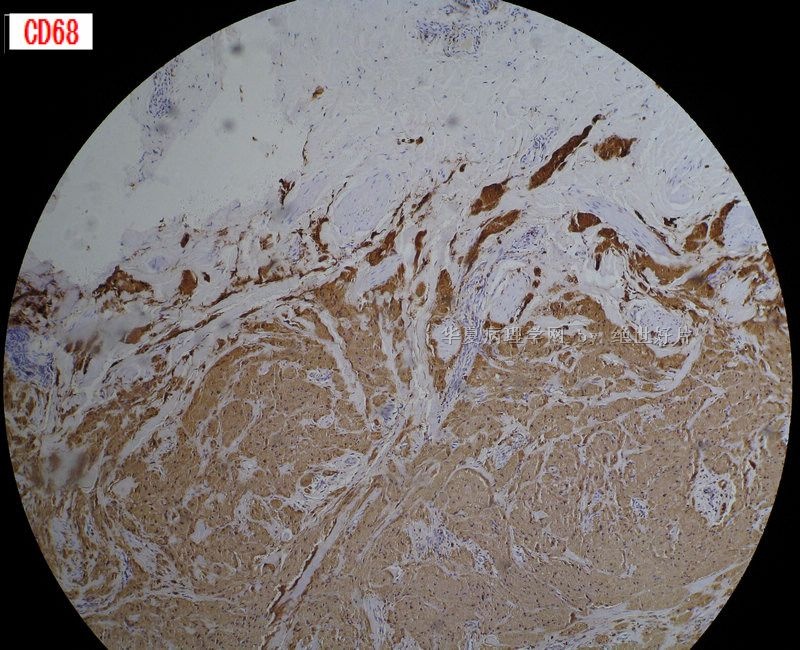
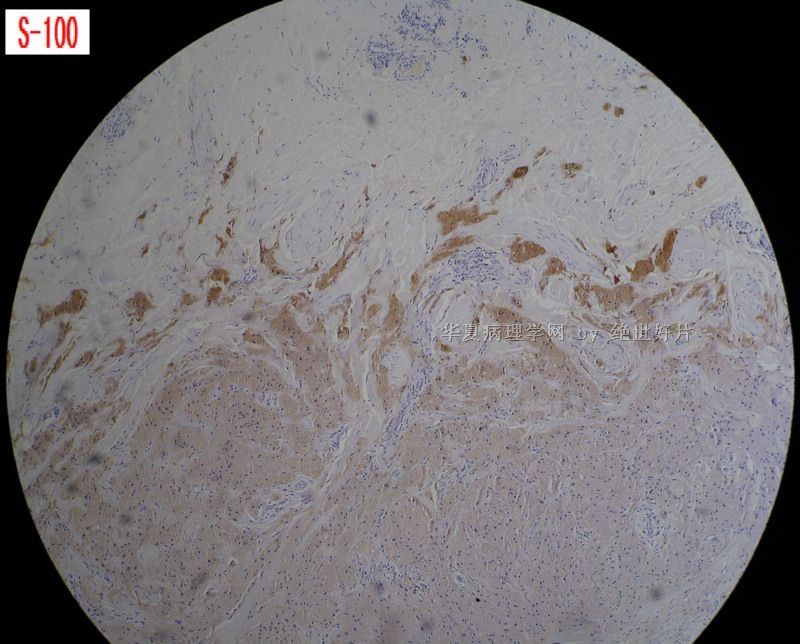
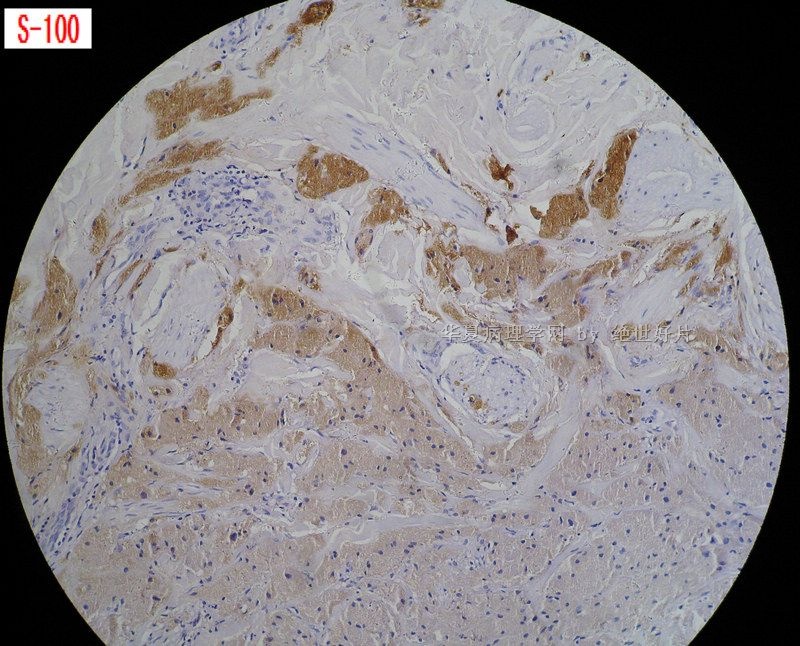
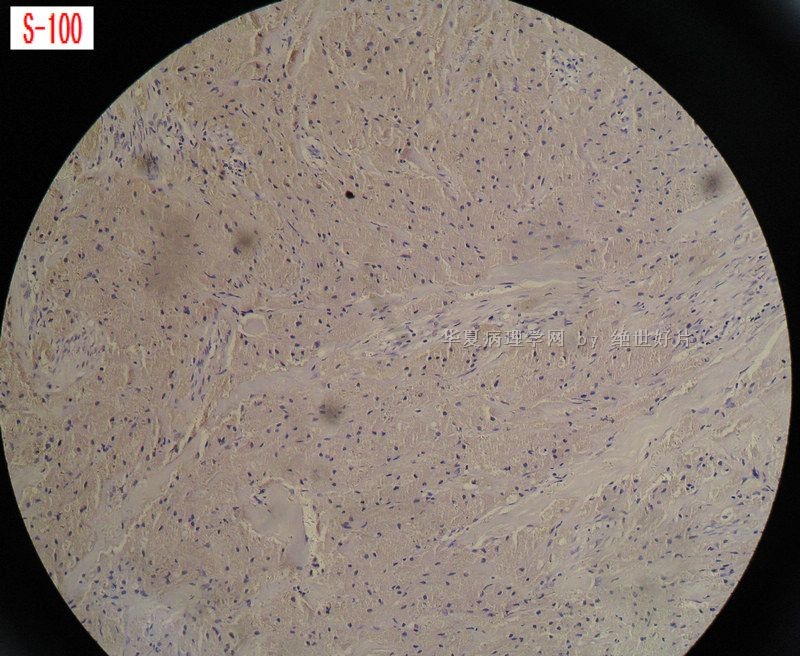
- B2439左乳头皮下肿物 免疫组化已上传 欢迎讨论
| 姓 名: | ××× | 性别: | 女 | 年龄: | 48 |
| 标本名称: | |||||
| 简要病史: | 左乳头肿大 | ||||
| 肉眼检查: | 带皮组织一枚,1.5*1*0.3,皮下见一结节,直径0.7厘米,灰白,质韧,境界尚清。 | ||||

名称:图1
描述:图1

名称:图2
描述:图2

名称:图3
描述:图3

名称:图4
描述:图4
标签:乳腺颗粒细胞瘤 S-100 CD68 NSE
-
本帖最后由 于 2010-01-27 22:01:00 编辑
相关帖子
×参考诊断
-
liguoxia71 离线
- 帖子:4174
- 粉蓝豆:3122
- 经验:4677
- 注册时间:2007-04-01
- 加关注 | 发消息
-
本帖最后由 于 2010-01-28 06:30:00 编辑
It is a typical granular cell tumor of the breast based on morphology and IHC.
Granular cell tumor is positive for s100 and CD68, negative for CK.
The main differential dx is histiocytoid carcinoma.
If you want to order two markers, S100 and AE1/AE3 should be your choice.
CASE REPORT
Granular Cell Tumor of the Breast: A Series of 17 Cases and Review of the Literature
Copyright © 2004 Blackwell Publishing, Inc.
KEYWORDS
breast neoplasm • granular cell tumor
Abstract:
 |
 |
|
|
|
Abstract: Seventeen cases of granular cell tumor (GCT) of the breast are reviewed. The demographics and clinical features are reviewed and the radiologic and pathologic features as well as the immunohistochemistry are discussed. To our knowledge, our series of 17 breast GCT cases represent the largest series published to date.
Article Text
Granular cell tumor (GCT), first described by Abrikossoff (1) in 1926, is a relatively rare neoplasm that is occasionally located in the breast. The tongue is the single most common anatomic site involved, but GCT may arise in virtually any body site and can be multifocal (2). The histogenesis of this tumor is still rather controversial, but S-100 protein positivity favors the theory of neural or neuroectodermal origin (3). GCT occurs in the breast in 5 to 6% of cases (4,5) and it occurs more commonly in premenopausal black women (6).
Granular cell tumor of the breast is usually benign, although there have been reported malignant GCT cases (7,8). Desmoplasia and lack of circumscription are common features of breast GCT (9) and it has been shown to be nondependent on estrogen and progesterone, despite the fact that most cases occur in premenopausal women and a few cases have also been described during pregnancy (10). Colocalization and coexistence of this tumor with infiltrating ductal carcinoma have been described in two separate reports (5,11). This report presents 17 cases of GCT of the breast (the largest series published to date), and the immunohistochemical markers that define them, seen at the University Hospital, Cincinnati, Ohio, over a period of 12 years.
MATERIALS AND METHODS
 |
|
|
|
|
Data for this study were obtained from medical records at the University Hospital, Cincinnati, Ohio. Seventeen cases were identified between January 1991 and December 2002, each with a histologically confirmed diagnosis of GCT of the breast. The hematoxylin-eosin-stained slides for all these cases were reviewed and the selected paraffin blocks were retrieved and submitted for immunohistochemistry staining for S-100 protein (Dako Corp., Mountain View, CA), estrogen receptor (Ventana Medical Systems Inc., Tucson, AZ), and progesterone receptor (Ventana).
RESULTS
|
|
|
|
|
Fourteen of the 17 cases we reviewed were women. The majority (16 of 17) of the patients were African American and one was Caucasian (Table 1). The age at the time of excision ranged from 17 to 68 years (average 40.3 years), with 9 of the 14 women less than 45 years old. There were three cases of multifocal GCTs, two of which had GCTs in sites other than the breast (right groin and abdomen), and the third later developed a tumor in the vulva 2 years after the initial diagnosis of tumor in the breast. The patient with GCT of the right groin had bilateral breast GCT, diagnosed 3 years prior to the development of the lesion in the groin. There was a case of colocalization with infiltrating ductal carcinoma of the breast, previously described by Al-Ahmadie et al. (11). The average diameter of resected tumor was 0.9 cm (range 0.25–2.6 cm) and both breasts were equally affected. Grossly eight of the tumors were described as well circumscribed, three as poorly circumscribed, and circumscription was not mentioned in the remaining six cases.
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
One of the cases was diagnosed by fine-needle aspiration biopsy before histologic confirmation. Histology showed sheets of large, polygonal cells, with round to oval eccentrically located nuclei, inconspicuous nucleoli, and abundant eosinophilic granular cytoplasm (Fig. 1a). There was no necrosis. Some of the cases showed minimal mitotic activity, however, most did not show any evidence of mitotic activity. There was a spindle appearance to the cells in the bilateral breast case (Fig. 1b), and the cells also showed prominent nucleoli and vesicular nuclei. All the cases showed strong positive staining for S-100 protein. While the estrogen- and progesterone-dependent ducts and breast acini stained positive for estrogen and progesterone receptors, tumor cells in all the cases were negative for both stains (Fig. 1c).
|
Figure 1. (a) Sheets of large polygonal cells with round to oval, eccentrically located nuclei and eosinophilic granular cytoplasm (hematoxylin-eosin; original magnification ×164). (b) Cells of GCT show intense positive S-100 staining. The spindle appearance of the cells is also highlighted (original magnification ×14.2; inset ×71). (c) Estrogen receptor demonstrates positive reactivity in the estrogen-dependent breast ducts, whereas it is negative in tumor cells (original magnification ×65). (d) Well-circumscribed lesion of GCT (hematoxylin-eosin; original magnification ×7.85). |
DISCUSSION
|
|
|
|
|
Granular cell tumor occurs in a wide variety of visceral and cutaneous sites. Abrikossoff (1) postulated a myogenic origin for the first case of GCT, which he described in the tongue. However, the histogenesis of this lesion has been the subject of controversy. Ulrich et al. (12) showed evidence of a histiocytic derivation, and Churg and Work (13) proposed a possible origin from smooth muscle cells, but the most widely accepted theory has been that of a Schwann cell origin, apparently because of the positivity of the tumor for the S-100 protein (4) and the similarities exhibited in the ultrastructural features of the tumor cells and those of a Schwann cell (10).
The granular appearance of the cytoplasm may be caused by accumulation of secretory granules, mitochondria, or lysosomes (14). Mittal et al. (15) showed evidence of granule origin as infoldings of cell membrane by a process similar to myelin formation around nerves. They further argued that the subsequent phagocytosis of the infoldings by lysosomes results in the characteristic cytoplasmic granules. The differential diagnosis of breast GCT includes fat necrosis and mammary duct ectasia, in which foamy macrophages may resemble the granular cells (16).
Granular cell tumor of the breast accounts for 5 to 6% of all GCTs (5,6), approximately 1 in every 1000 breast cancers (9), and it arises from interlobular breast stroma. While the majority of GCTs behave in a benign manner, occasional malignant cases have been described (7,8). One of the cases we reviewed was that of a bilateral breast GCT, with a spindle appearance of the cells, vesicular nuclei, and prominent nucleoli. We are not aware of a previous report of such a case. One may speculate in cases of bilateral breast GCT that there are two benign synchronous lesions, there are two malignant synchronous lesions, or one lesion represents metastasis.
A similar argument can be made for the other cases in which diagnosis of GCT was made in additional sites outside of the breast. In contrast to breast carcinomas, which occur more commonly in the upper outer quadrant, GCTs more frequently occur in the upper inner quadrant of the breast (10), and this distribution appears to correspond to the area of innervation of the skin of the breast by the supraclavicular nerve (5). It may cause retraction and ulceration of the overlying skin and may also be fixed to the pectoralis fascia, thereby mimicking carcinoma.
Breast GCT occurs more commonly in premenopausal women and it is more common in African American patients (6). This ethnic propensity was confirmed in our series, where all of the males and 13 (93%) of the females were African American. However, Strong et al. (17), in a clinical study of 95 patients, found a predominance of white patients.
The premenopausal age group comprised nine of the patients in our series. Due to the preponderance of this tumor in premenopausal women, high levels of estrogen and progesterone have been suggested to play a key role in tumor growth. This is further corroborated by the rapid increase in the size of breast GCT observed in pregnancy (10). However, all of the cases in our series stained negative for both estrogen and progesterone receptors, an indication of nondependence of this tumor on both estrogen and progesterone.
Lack et al. (2), in their review of 110 cases of GCT from various body sites, described GCTs as generally well circumscribed, whereas Kragel et al. (9) opined that a lack of circumscription is a common feature of breast GCT. However, eight (47%) of the cases in our series were well circumscribed, three (18%) were poorly circumscribed, and circumscription was not described in six (35%).
The mammographic presentation of GCT is variable. These lesions may present as round, circumscribed masses, as indistinct densities, or as spiculated masses indistinguishable from carcinoma (Fig. 2a). Microcalcifications are usually not present. The ultrasound appearance is also variable, including solid, poorly marginated masses with marked posterior shadowing, as well as more benign-appearing circumscribed masses (Fig. 2b). Cross section usually shows a firm, grayish-white to yellow tumor. Microscopically the tumor may be well circumscribed (Fig. 1d), and it is usually characterized by nests and sheets of polygonal cells with distinct borders and abundant granular eosinophilic cytoplasm. Nuclei are usually small, centrally located, and hyperchromatic (2). Features that are suggestive of malignancy include large tumor size (greater than 5 cm), cellular and nuclear pleomorphism, prominent nucleoli, increased mitotic activity, presence of necrosis, and local recurrence (6). On cytologic examination, GCT consists of sheets of large granular cells intersected by arborizing thin-walled blood vessels. The cells have round to oval nuclei, inconspicuous nucleoli, and abundant, often ill-defined granular cytoplasm (18).
|
Figure 2. (a) Mammogram shows an area of indistinct density. (b) Ultrasound shows well-circumscribed, nonechogenic mass in the breast. |
Correct diagnosis can be made by aspiration cytology, but in most cases histologic examination is necessary to establish the true nature of the lesion. Raju et al. (3), in their immunohistochemical study of eight cases of GCT demonstrated that in all the lesions, GCT cells showed strong cytoplasmic and nuclear staining for S-100 protein. One of the eight GCTs in that series, the only breast GCT, stained positive for alpha
The 17.6% incidence of multiple tumors in our series contrasts with the 5.4% noted by Lack et al. (2) in their large clinical series. They had 10 breast cases as part of their series but the proportion involved by multiple tumors cannot be ascertained. The cases of colocalization and coexistence of this tumor described in the literature were seen in patients with relatively advanced ages compared with the average age of patients with GCT (5,11). Treatment for this condition is wide local excision because local recurrence has been reported in a few instances.
Surg Oncol. 2010 Jan 12. [Epub ahead of print]
Granular cell tumour of the breast.
Brown AC, Audisio RA, Regitnig P.
Royal Sussex County Hospital, Eastern Road, Brighton, BN2 5BE, UK.
Granular cell tumour of the breast (GCTB) is a rare tumour which arises from Schwann cells. It is a largely benign tumour but in extremely rare cases can exhibit malignant characteristics. It posses a particular problem as it's characteristics can mimic breast carcinoma clinically, radiologically and macroscopically. This results in the potential misdiagnosis of breast carcinoma and over treatment of patients. Typically GCTBs are benign, solitary lesions but variations include malignant GCTBs, colocalisation with breast malignancies and multicentricity. These tumours can be investigated using mammography, ultrasound and magnetic resonance imaging. However none of these modalities have yet identified any GCTB specific characteristics. On pathological examination they can be identified using both microscopic and immunohistochemical features. The cells have a distinctive granular eosinophilic cytoplasm associated with typical nuclei and abundant lysosomes. Immunohistochemically they are positive for S100 protein, CD68 and neuron specific endolase (NSE). They are treated with wide local excision and while they may reoccur, are associated with a good prognosis.











