
图1")
图2")
图3")



| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
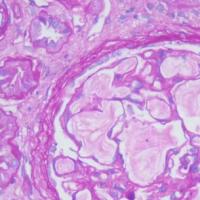
- B2230不典型小叶增生累及乳头状瘤(cqz-27)
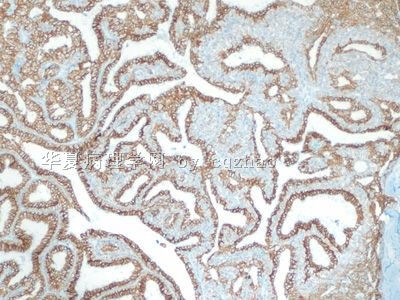
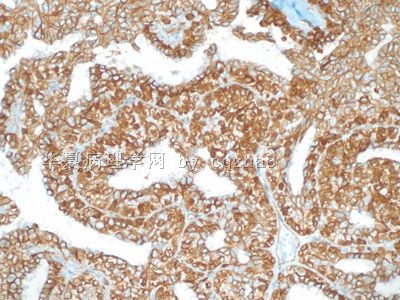
F1, E-cadherin
F2. P-120
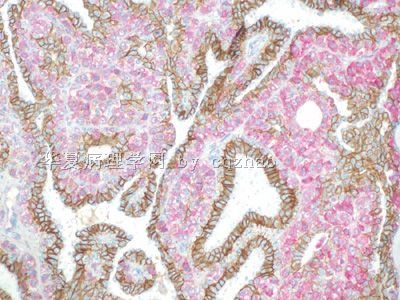
F3. dual stain 200x
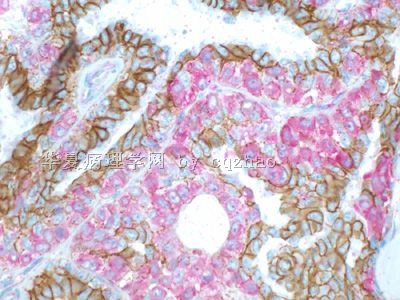
F4. dual stain 400x
So it is atypical lobular hyperplasia involving papilloma. I signed out this case as atypical papilloma with comment.
Important points for this case:
1. ALH can involve many different lesions, such as sclerosing adenosis, fibroadenoma, radial scar, papilloma......
2. Atypical papilloma can have different meaning.
-
shihong4699 离线
- 帖子:1024
- 粉蓝豆:43
- 经验:2917
- 注册时间:2009-01-20
- 加关注 | 发消息
-
ZQH19811029 离线
- 帖子:458
- 粉蓝豆:1
- 经验:458
- 注册时间:2009-11-15
- 加关注 | 发消息
-
1212121212 离线
- 帖子:37
- 粉蓝豆:1
- 经验:37
- 注册时间:2009-12-06
- 加关注 | 发消息
-
ketty_wang 离线

- 帖子:366
- 粉蓝豆:12
- 经验:520
- 注册时间:2007-09-22
- 加关注 | 发消息
|
翻译 Recently I am very busy with other things. Sorry I did not follow up this case on time. Anyway I will continue to work with your guys for this case. 1. 腺肌上皮瘤 is a differential dx. However the IHC did not support the dx 2. Now most of people think it is introductal papilloma. It is true it is introductal papilloma. 3. I would not show you a classic introductal papilloma case. So it must have some other lession related to the papilloma. Please check the photos more carefully, especially in high power. 4. In order to make it easy for you. I will paste some photos with areas close to the papilloma. |
|
最近我一直忙于其他的事情,很抱歉我没有及时跟踪这个病例。但是,无论如何,我将和你们一起继续探讨这个病例。 1腺肌上皮瘤 是个鉴别诊断。然而免疫组化不支持这个诊断。 2 现在很多人认为这例是导管内乳头状瘤。确实这是导管内乳头状瘤。 3 我不会展示给你们一个典型的导管内乳头状瘤。所以一定有和乳头相关的其他病变,请仔细看图片,特别是高倍视野。 4 为了看起来容易些,我将贴一些和乳头相邻病变的照片。 |
Some areas close to the papilloma
和乳头相邻的地方
what diagnosis will you made for these areas close to the papilloma?
这些和乳头结构相临地区的病变你诊断什么?
Forget the papilloma now. What is the diagnosis for the photos in floor 29?
现在忘记乳头状瘤,29层的图片你诊断什么?
Most netfriends are interested to the cancer cases, but not some uncertained cases.
Thank 青青子矜 for above reasonable analysis. Based on her instruction, I paste here dual IHC for p120 and E-cadherin for the lesions (floor 29), areas close to the large papilloma.
许多网友对诊断癌的病例感兴趣,而对不确定的病例不感兴趣。
感谢以上青青子矜的合理的分析。基于她的建议,我在这里贴上(29层)病变的p120 和 E-cadherin免疫组化照片,这个地方是和大乳头相邻的视野
If you do not know how to interpretate the stains, please check this topic
如果你不知道如何解释染色结果,请看链接:
http://www.ipathology.com.cn/forum/forum_display.asp?classcode=129&keyno=111923&pageno=2
1. It is 残存导管.
2. It is difficult to separate LCIS from ALH for some cases even though there are good calssification or definition. For this case it is ALH not LCIS
3. Lobular neoplasia (ALH and LCIS) is only an indicator of the risk for more severe lesions. In the
No need to treat lobular neoplasia.
1E-CA阳性为残存导管
2 虽然有很好的定义和分类,小叶原位癌和不典型小叶增生的区分仍然很困难这一例是不典型小叶增生,而不是小叶原位癌。
3. 小叶肿瘤(不典型小叶增生 和 小叶原位癌)只是一个衡量更严重病变的风险指标。在美国,许多人认为如果针刺活检诊断小叶肿瘤,这个病人应该做(肿块)切除活检
没有必要治疗小叶肿瘤
|
F1, E-cadherin F2. P-120 F3. dual stain(双染) 200x F4. dual stain(双染) 400x So it is atypical lobular hyperplasia involving papilloma. I signed out this case as atypical papilloma with comment.所以这例是不典型小叶增生累及乳头状瘤。我签发为不典型乳头状瘤并注解。 Important points for this case: 1. ALH can involve many different lesions, such as sclerosing adenosis, fibroadenoma, radial scar, papilloma...... 2. Atypical papilloma can have different meaning. |
|
这例的要点在于: 1不典型小叶增生可以包括很多不同的病变,比如硬化性腺病、纤维腺瘤、放射状瘢痕、乳头(状)瘤等等 2 不典型乳头状瘤可以有很多涵义。 |
|
If it was a breast core biopsy, patient should have excisional bx. This was excisional biopsy specimen. So follow up with mammogram is propriate. 如果病人是针刺活检(诊断小叶肿瘤),这个病人应该做(肿块)切除活检 这个是(肿块)切除活检,所以乳腺X线照片随访就可以了。
|
|
|

- 学无止境











