
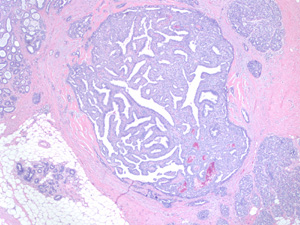
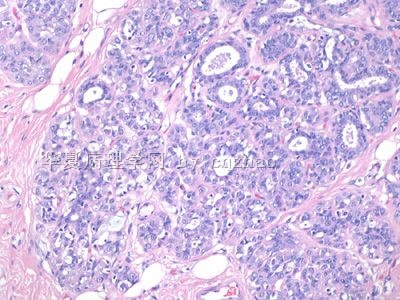
图1")
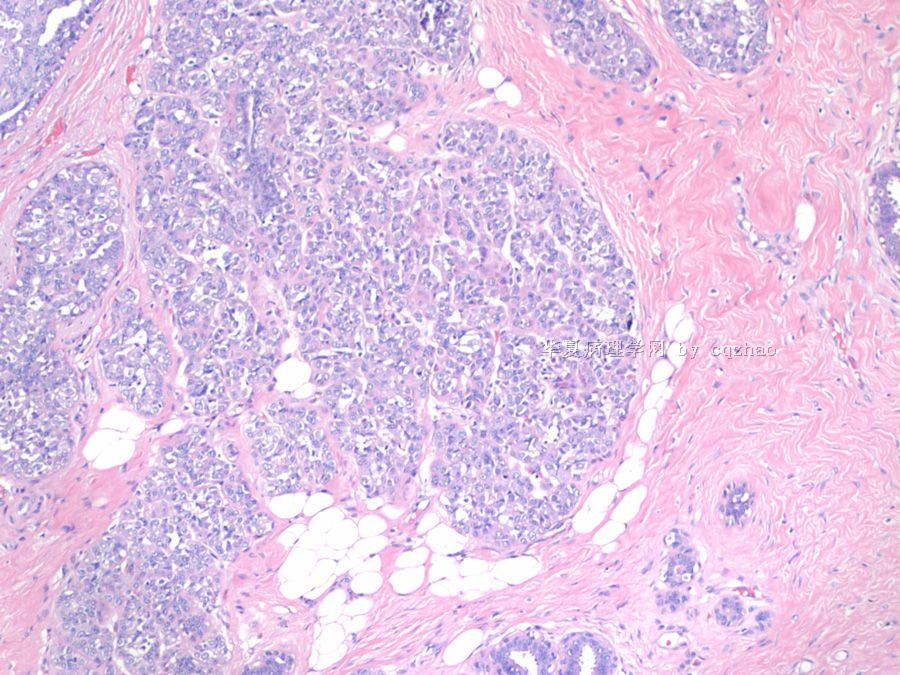
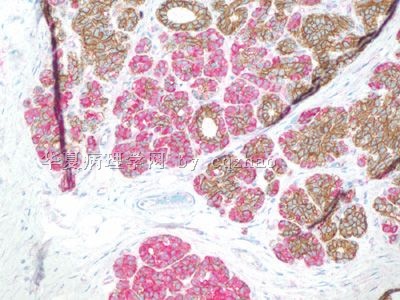
图2")
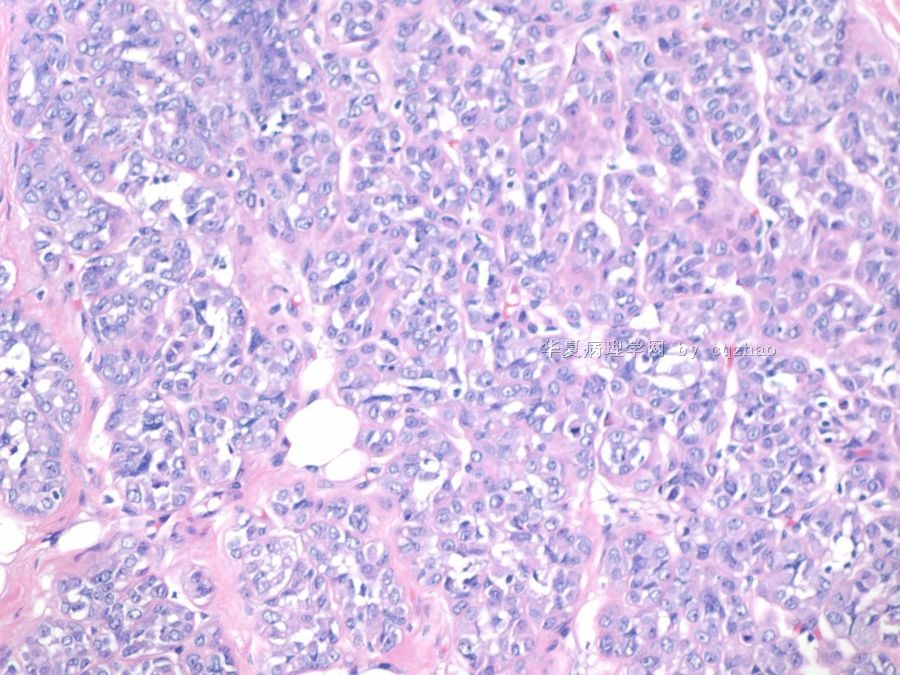
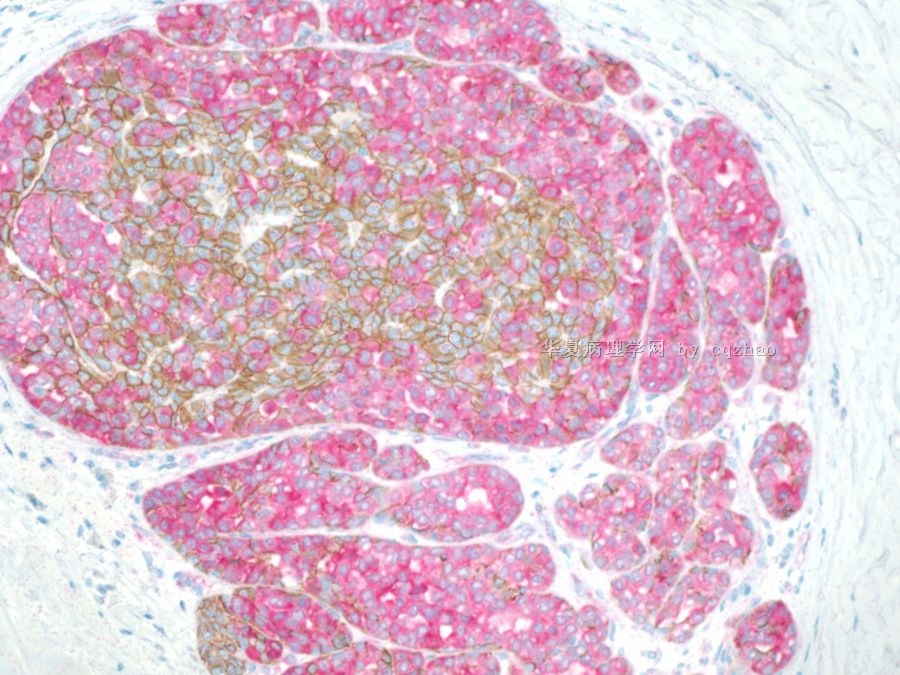
图3")





| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- B2230不典型小叶增生累及乳头状瘤(cqz-27)
Interested to ses above differential dx. This is a consult case. The primary pathologist (from a local hospital) thought it maight be a DCIS (papillary type). Some general pathologists in the usa are not good////.
One of our breast path fellow reviewed the case and thought it may be denomyoepithelioma as most of you.
-
ketty_wang 离线

- 帖子:366
- 粉蓝豆:12
- 经验:520
- 注册时间:2007-09-22
- 加关注 | 发消息
翻译
Interested to ses above differential dx. This is a consult case. The primary pathologist (from a local hospital) thought it maight be a DCIS (papillary type). Some general pathologists in the
One of our breast path fellow reviewed the case and thought it may be denomyoepithelioma as most of you.
很高兴看到上面这么多不同的诊断,这是一个会诊病例。最初的病理医生(地方医院)认为它可能是导管原位癌(乳头型)。
我们的一个乳腺病理医生看了片子后,和你们大多数人意见一致,认为它可能是腺肌上皮瘤。
P63 stain P63 染色
Now do you still think it is adenomyoepitheliona?
现在,你还认为是腺肌上皮瘤吗?

- 学无止境
Recently I am very busy with other things. Sorry I did not follow up this case on time. Anyway I will continue to work with your guys for this case.
1. 腺肌上皮瘤 is a differential dx. However the IHC did not support the dx
2. Now most of people think it is introductal papilloma. It is true it is introductal papilloma.
3. I would not show you a classic introductal papilloma case. So it must have some other lession related to the papilloma. Please check the photos more carefully, especially in high power.
4. In order to make it easy for you. I will paste some photos with areas close to the papilloma.
小叶膨大,小叶内尚可以看到残存正常腺管,腺管周围可见细胞增生呈巢团或腺泡状,但具体细胞看不太清楚。
我怀疑有LCIS或DCIS和LCIS并存。需要标记的支持,尤其是CK5/6\E-cad\34BE12的表达情况
以下是我们刚刚翻译的乳腺病理书中一段,先秀出来大家共享:
DCIS和LCIS:绝大多数DCIS和LCIS的区分比较简单,但部分病例仍有麻烦,原因主要有以下两方面:(1) DCIS和LCIS累及的导管-小叶内的病变模式有重叠(即LCIS 可能出现管状,而DCIS也可能包含有可以辨认的小叶);(2)部分DCIS病变特征和LCIS有重叠(例如:小细胞且胞核单调一致、胞质内空泡及实性生长方式)或部分LCIS具有和DCIS相重叠的特征(例如:胞核的多型性、粉刺样坏死、顶浆分泌及假筛状结构)。此外,DCIS和LCIS的诊断并不是相互排斥的,这两种病变在同一乳腺中可以并存,位于同一末梢导管-小叶单位内甚至同一部位(Fig. 3.46)。细胞间黏附性差及胞质内空泡倾向诊断为LCIS,而紧密性生长、无胞质内空泡、病变外围细胞的极化以及微腺泡结构更支持DCIS的诊断。对于有争议的病例,E-cadherin染色有一定价值,因为LCIS的E-cadherin失表达而DCIS瘤细胞表达阳性
Most netfriends are interested to the cancer cases, but not some uncertained cases.
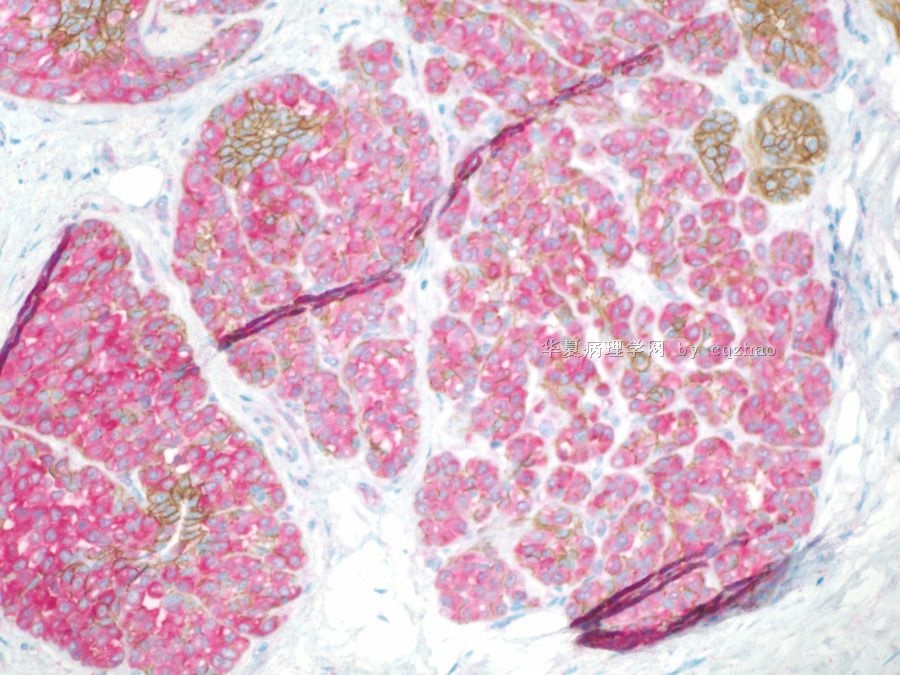
Thank 青青子矜 for above reasonable analysis. Based on her instruction, I paste here dual IHC for p120 and E-cadherin for the lesions (floor 29), areas close to the large papilloma.
1. It is 残存导管.
2. It is difficult to separate LCIS from ALH for some cases even though there are good calssification or definition. For this case it is ALH not LCIS
3. Lobular neoplasia (ALH and LCIS) is only an indicator of the risk for more severe lesions. In the USA most people think if lobular neoplasia is present in the core bx, the patients should have excisional biopsy.
No need to treat lobular neoplasia.











