























| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
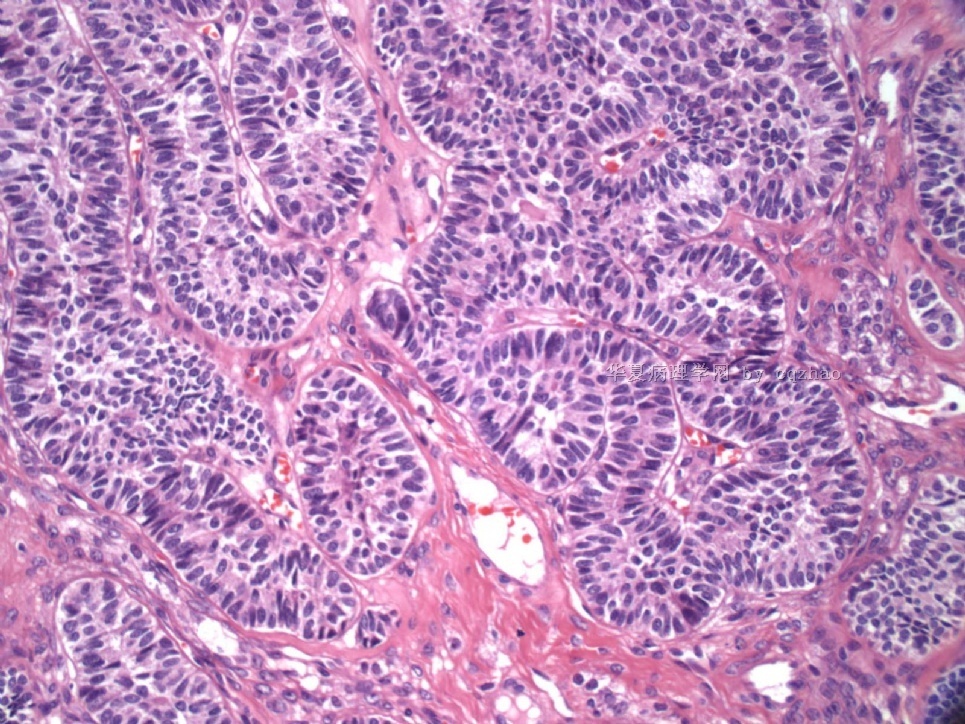
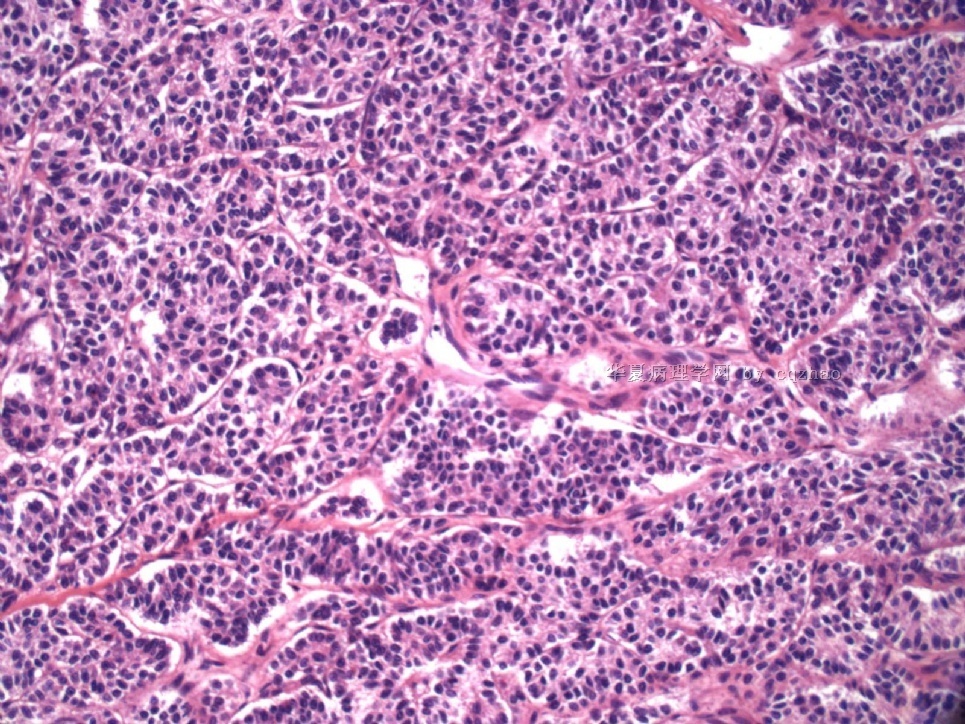
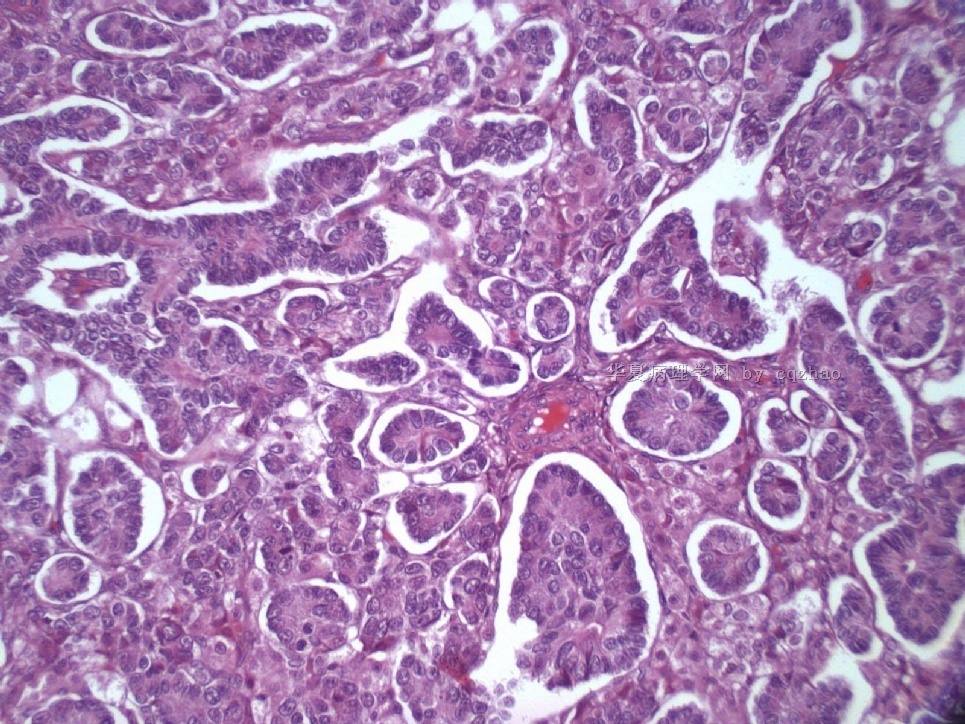
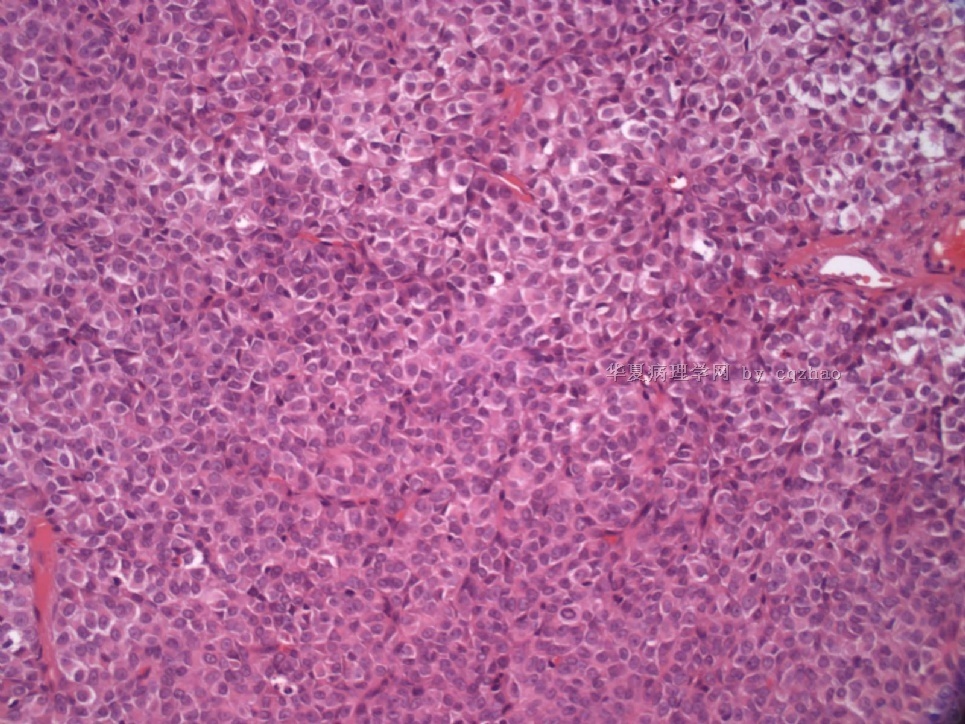
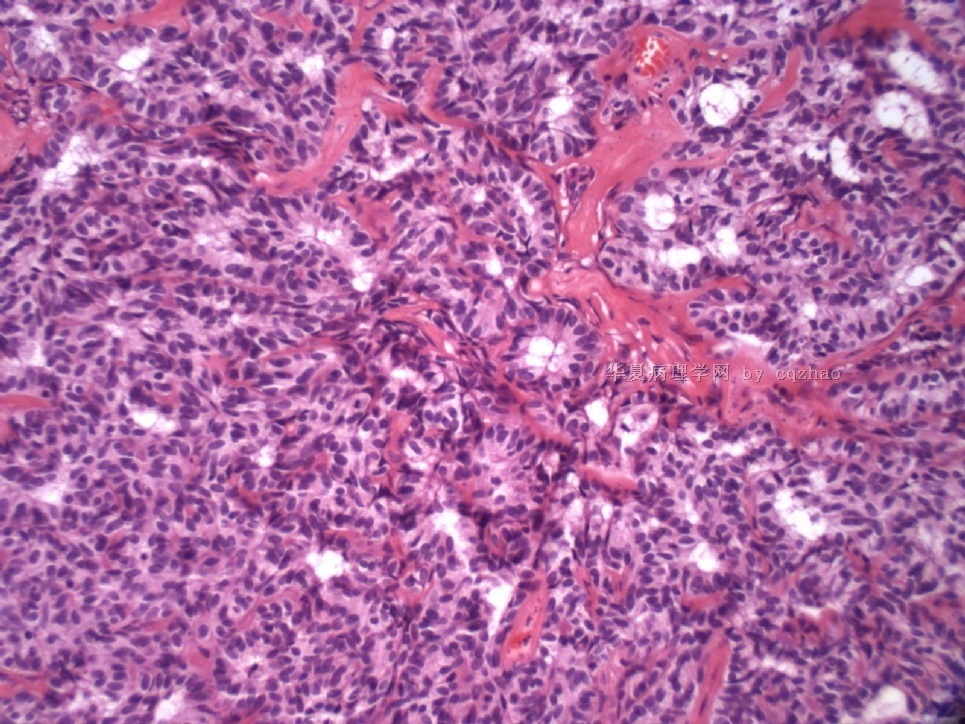
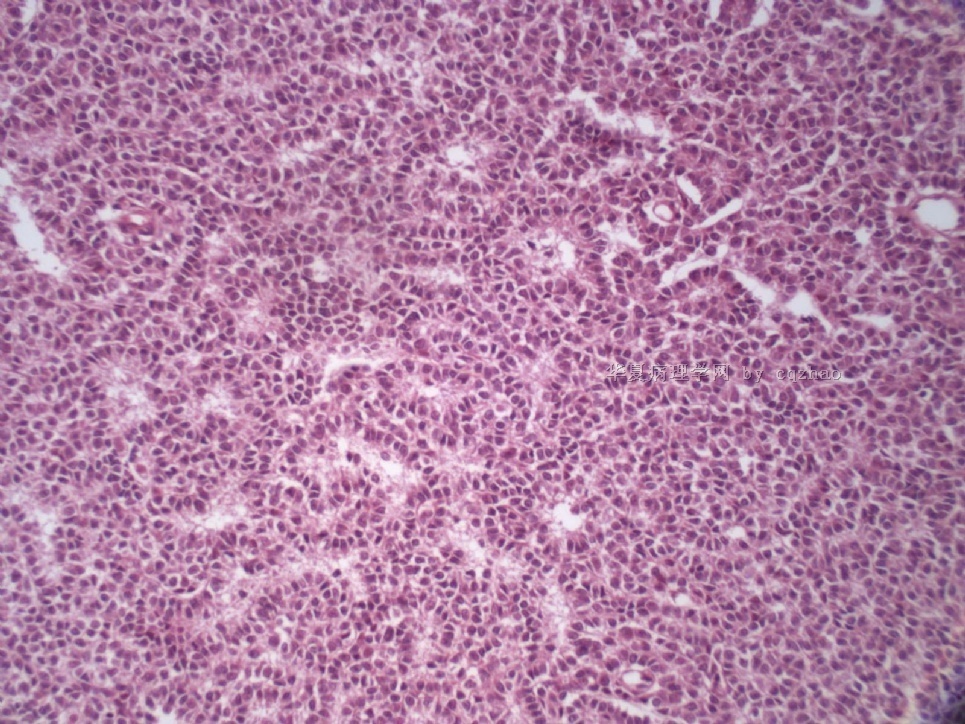
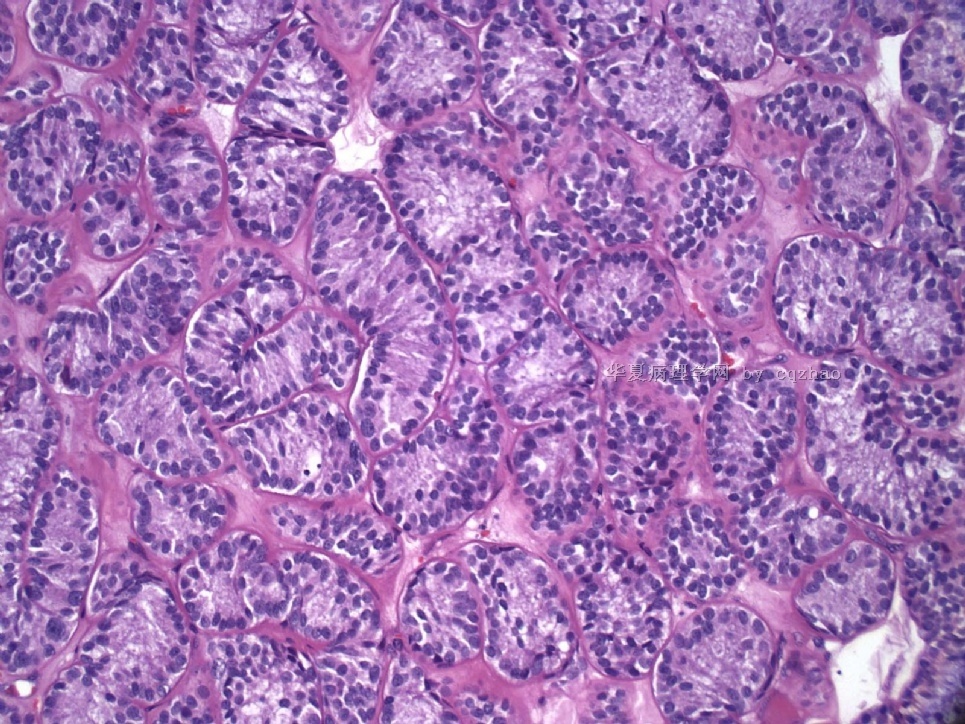
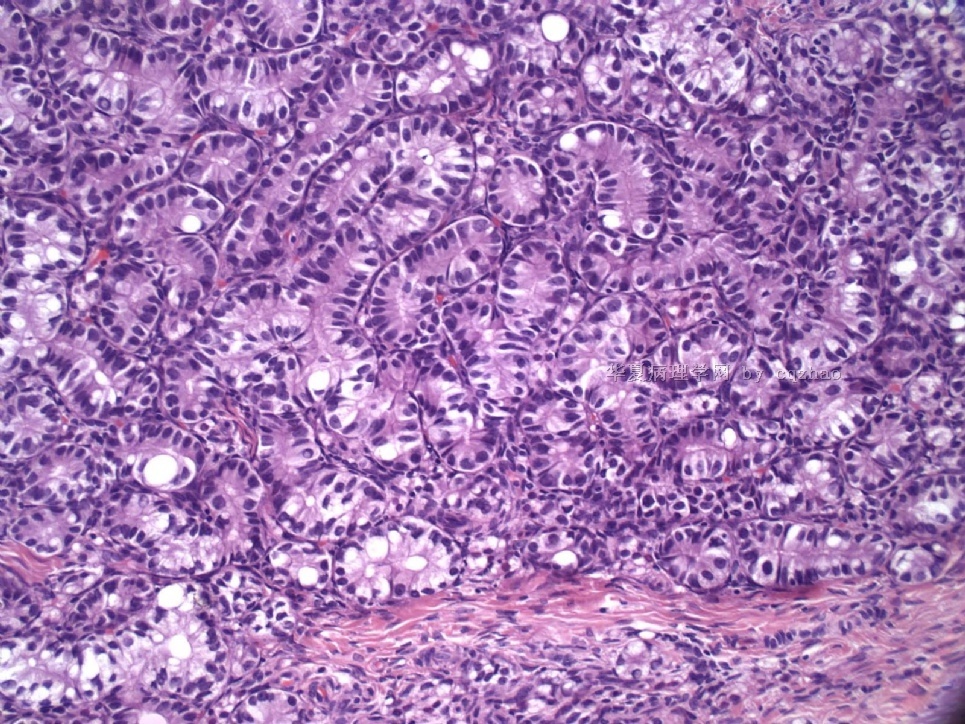
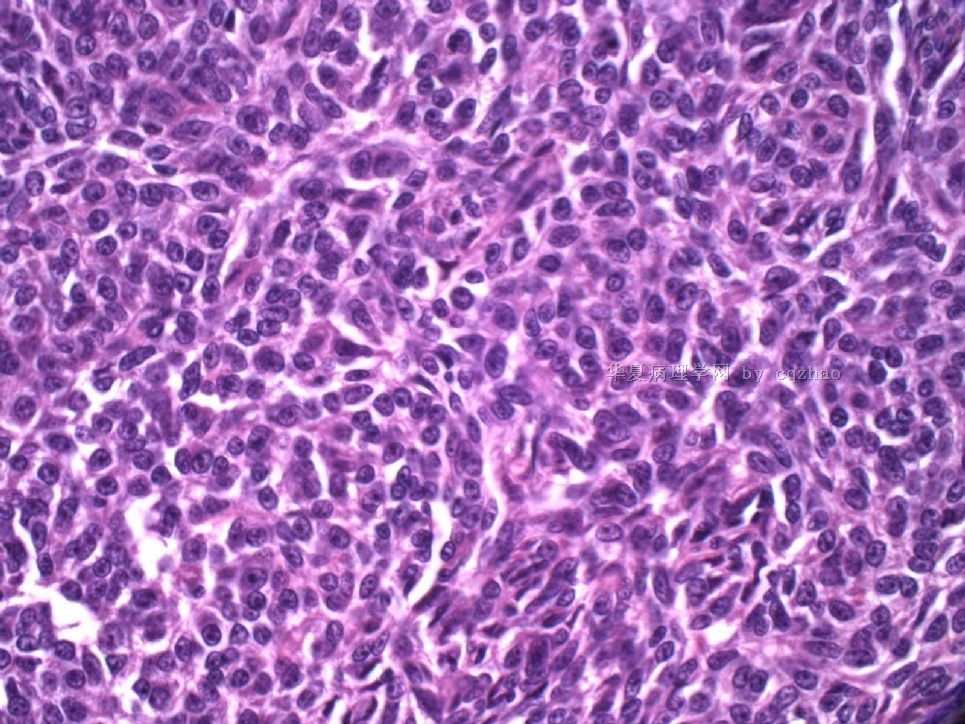
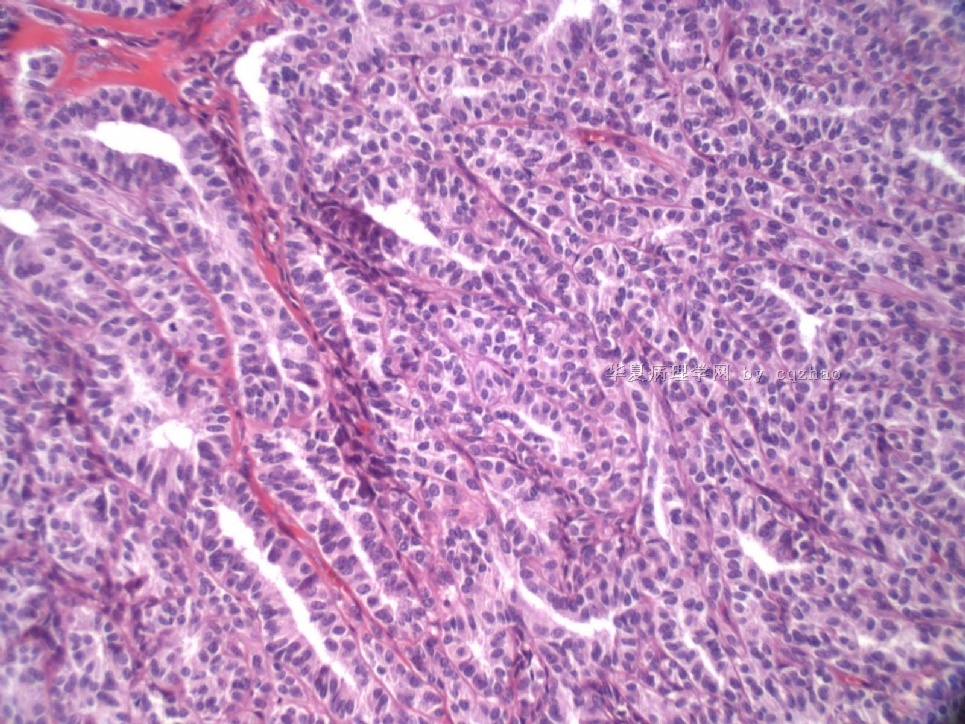
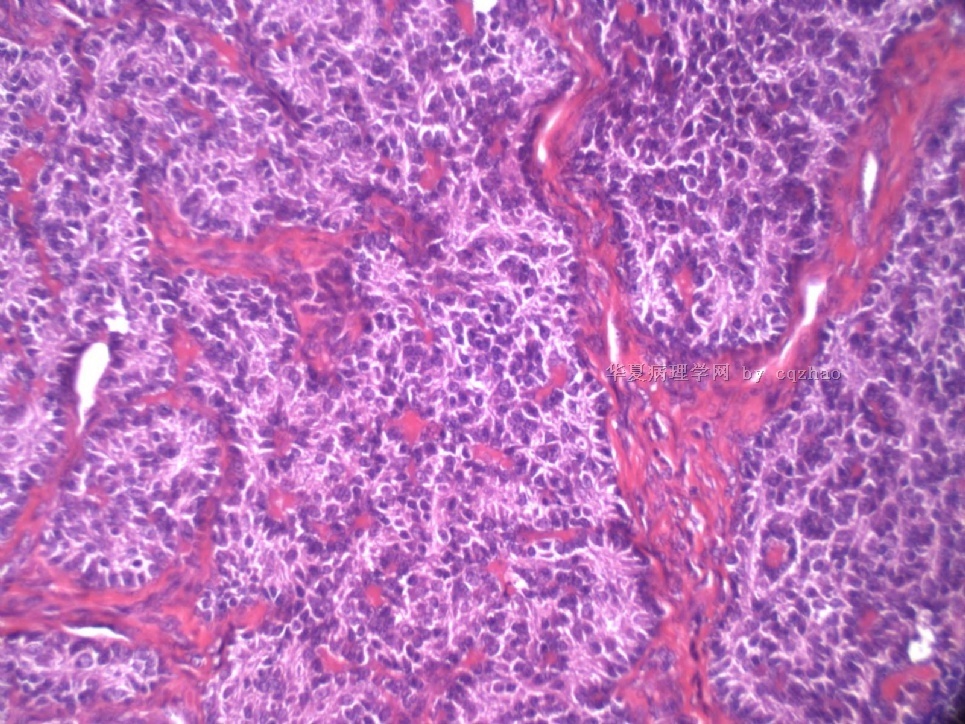
- Sharing some photos of ovarian pure sertoli cell tumors
-
Department of Pathology, Magee-Womens Hospital, University of Pittsburgh Medical Center, Pittsburgh, PA 15213, USA. zhaoc@upmc.edu
Different immunohistochemical sex cord-stromal markers have been previously studied in various types of ovarian sex cord-stromal tumors; however, the sensitivity for sex cord-stromal lineage may vary between markers, and some markers may not be as sensitive in some types of sex cord-stromal tumors compared with other tumors in this spectrum of neoplasms. The goals of this study were to determine which immunohistochemical markers are the most sensitive and immunohistochemically robust for sex cord-stromal lineage within a given type of ovarian sex cord-stromal tumor, and to establish whether there are substantial differences of expression of these markers between different types of sex cord-stromal tumors. Immunohistochemical stains for markers which have known variable specificity for sex cord-stromal lineage [inhibin, calretinin, MART-1/melan-A, CD99, steroidogenic factor 1 (SF-1, adrenal 4-binding protein), and WT1], were performed in 127 cases of 5 different types of ovarian sex cord-stromal tumors: adult granulosa cell tumor (n=32), Sertoli cell tumor (n=27), Sertoli-Leydig cell tumor (n=18), steroid cell tumor (n=25), and fibroma/fibrothecoma (n=25). All cases in each type of sex cord-stromal tumor expressed SF-1. Inhibin and calretinin were expressed in all groups of tumors but with a lesser frequency (56% to 100% and 36% to 100% of cases, respectively). All types of tumors except steroid cell tumor expressed WT1. Fibroma/fibrothecoma was the only type of tumor that did not express CD99. The only tumor groups that showed expression of MART-1 were Sertoli-Leydig cell tumor (restricted to the Leydig cell component) and steroid cell tumor (94% and 96% of cases, respectively). The type of sex cord-stromal tumor that was least frequently positive for several of the different markers studied was fibroma/fibrothecoma. Among all tumor groups combined, inhibin and WT1 were the 2 markers showing the most diffuse expression. Likewise, the single marker showing the most optimal combination of diffuse and strong staining (immunohistochemical composite score: possible range, 1 to 12) varied between tumors: adult granulosa cell tumor-inhibin (score 10.0); Sertoli cell tumor-WT1 (score 10.8); Sertoli-Leydig cell tumor (Sertoli cell component)-WT1 (score 10.4); steroid cell tumor-inhibin (score 11.2); and fibroma/fibrothecoma-WT1 (score 8.9). We conclude that most immunohistochemical sex cord-stromal markers have sufficient sensitivity for sex cord-stromal lineage. Although each of the different types of sex cord-stromal tumors has a slightly unique immunoprofile in terms of frequency and extent of expression, these differences are relatively minor for most types of tumors with certain exceptions (eg, WT1 is not diagnostically useful in steroid cell tumor; CD99 is not diagnostically useful in fibroma/fibrothecoma; the only sex cord-stromal tumor for which MART-1 is diagnostically useful is steroid cell tumor; inhibin and calretinin are less diagnostically useful in fibroma/fibrothecoma than in the other types of tumors, but expression in fibrothecoma was higher than in fibroma). SF-1 is the most sensitive sex cord-stromal marker among the most common types of sex cord-stromal tumors. Given the findings relating to sensitivity and extent of expression in this study, and known specificity in the literature, the most informative sex cord-stromal markers to be used for the distinction from nonsex cord-stromal tumors are inhibin, calretinin, SF-1, and WT1 (the exact number of markers to be used should be based on the degree of difficulty of the case and level of experience of the pathologist); however, the utility of immunohistochemistry for the diagnosis of fibroma/fibrothecoma is somewhat limited.
: Am J Surg Pathol. 2009 Mar;33(3):354-66.
Identification of the most sensitive and robust immunohistochemical markers in different categories of ovarian sex cord-stromal tumors.
-
cqzhao老师回复:
以上都是支持细胞瘤,是我从AFIP的存档中找出来的,我曾经做过免疫组化(每一例都做了20种左右的染色)。在AFIP的时候我曾经复习了150例的SCT病例,40例做了免疫组化。
对于第四例有人认为是性索间质肿瘤伴环状小管(SCTAT),但是也有称作SCT,复杂管状型(Tavassoli)。其实二者可能是对相同的肿瘤不同作者的不同叫法。认为是SCTAT的可能将之与Peutz-Jeghers综合症联系起来了。实际上Dr。Young的文章发现有11%(6/54)的SCT患者具有该综合症。
第五例是SCT,梭形细胞样生长的组织结构。如果仔细观察的话还是可以看到管状的结构的。
以下是相关文献,有意者自译

- 赚点散碎银子养家,乐呵呵的穿衣吃饭
-
本帖最后由 于 2009-07-30 02:13:00 编辑
Pure ovarian sertoli cell tumors are rare. I am pasting here another 22 cases of pure sertoli cell tumors. All of these cases are AFIP consult cases since 1970 years. I choose them from my study files. Please enjoy different growth patterns of the tumors and do not question the dx. All of these cases were reviewed by at least three gyncologic pathologists and were stained for more than 20 immuno markers.
I am sure that you are the one of a few pathologists in the world who have seen so many cases of ovarian pure sertoli cell tumors.
Each photo represents one case with 100 or 200 x or 400x
-
本帖最后由 于 2009-08-03 07:45:00 编辑
Ovarian sex cord stromal tumors are rare and may be difficult to make dx. Pure sertoli cell tumors (SCTs) may have variable growth patherns, such as open or solid tubules (most common), cords, trabeculae, solid or diffuse, retiform, pseudopapillary, alveolar, islands, spindled, glandular, lipid, oxyphilic et al. The common differential dx include endometrioid carcinoma, especially sertoli form endometrioid carcinoma, carcinoid tumor (primary or metastatic), metastatic tubular Krukenberg tumor, mesonephric tumor, sepcially female adnexal tumors of probably Wolffian origin (FATWO), Yolk sak carcinoma, and other ovarian epithelial tumors et al.
IHC stains are very important for the dx of ovarian sex cord stromal tumors.
-
本帖最后由 于 2009-08-03 07:53:00 编辑
Wish every one who read these photos understand that one category of ovarian sex cord stromal tumor (SCST) can have many different growth patterns, also various ovarian SCST can share similar growth pattern. Of cause this 现象can occur in almost all other tumors also. I may paste the web some cases with IHC in future.
-
本帖最后由 于 2009-08-03 07:43:00 编辑
You cannot make your dx based on the photos. The purposes that I shared the photos here are I hope people can know the rare tumors like sertoli cell tumors can have variable growth patterns, but not only some clssic patterns. For the true cases you need to know patients' clinical information, tumor gross features, many sections of H@E slides, immunostains, even some molecular methods.
Thanks, cz











