
FNA and its differential diagnosis (cqz 3)图1")
FNA and its differential diagnosis (cqz 3)图2")
FNA and its differential diagnosis (cqz 3)图3")

 ,我喜欢刨根问底
,我喜欢刨根问底 ,请专家赐教!谢谢!
,请专家赐教!谢谢!

| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- Neck 副节瘤 (paraganglioma )FNA and its differential diagnosis (cqz 3)
-
本帖最后由 于 2008-12-19 23:15:00 编辑
This case is difficult and rare. Maybe I should put the case here.
IHC: Chromogranin+, synaptophysin+, GFAP-, EMA-, Pan CK-, calcitonin-
few spindle cells are positive for S-100. Sorry I do not have IHC photos to show you.
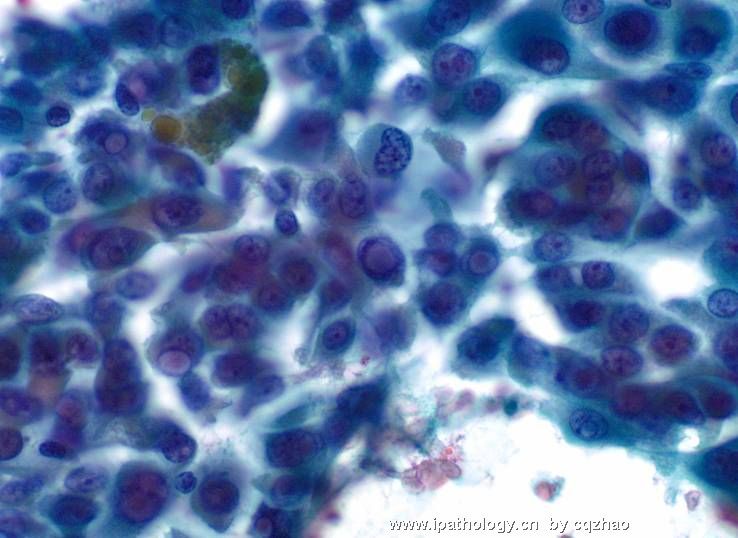
Also give you another photo from this case.
Now I hope every one know the dignosis
名称:图1
描述:图1
-
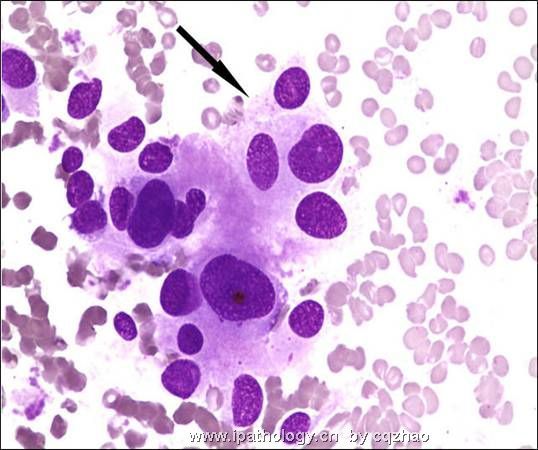
This is indeed a difficult case. I have to admit that I thought originally that this is going to be a medullary carcinoma of the thyroid. I would do the same immuno stains that Dr. Zhao has done. Now, calcitonin is negative, it pretty much exclude medullary ca. With neuroendocrine markers positive and few cells positive for S-100. I think I know what is the diagnosis. How about our chinese cytopathologists? By the way, I think the arrow in the above photo is pointing to neurosecretory granules, which are best appreciated on DF stain.
-
本帖最后由 于 2008-12-30 11:27:00 编辑
| 以下是引用陈隆文博士在2008-12-20 0:01:00的发言: This is indeed a difficult case.这的确是一例非常难的病例。 I have to admit that I thought originally that this is going to be a medullary carcinoma of the thyroid. 我必须回帖,我认为这可能是一例甲状腺的髓样癌,I would do the same immuno stains that Dr. Zhao has done.如果是我的病例,我也想赵老师那样做免疫组化, Now, calcitonin is negative, it pretty much exclude medullary ca. 虽然降钙素是阴性的,它有那么漂亮的图还是甲状腺髓样癌,With neuroendocrine markers positive and few cells positive for S-100. 神经内分泌标记阳性,极少数细胞S100阳性,I think I know what is the diagnosis.我能想到病理诊断。 How about our chinese cytopathologists?咱们中国的病理医生们考虑什么诊断? By the way, I think the arrow in the above photo is pointing to neurosecretory granules, which are best appreciated on DF stain.随便说一句,图上箭头所指是神经内分泌颗粒,如果用DF染色表达更好。 |
| 以下是引用cqzhao在2008-12-19 23:12:00的发言:
This case is difficult and rare. Maybe I should put the case here. IHC: Chromogranin+, synaptophysin+, GFAP-, EMA-, Pan CK-, calcitonin- few spindle cells are positive for S-100. Sorry I do not have IHC photos to show you. Also give you another photo from this case.
Now I hope every one know the dignosis |
谢谢赵博士!
大致翻译如下:
此例是疑难和罕见的。可能是我放到这里原因。
免疫组化:Chromogranin+, synaptophysin+, GFAP-, EMA-, Pan CK-, calcitonin-
少数梭形细胞S - 100 是阳性。很抱歉我没有免疫组化的照片向您展示。
也给你此例的另一张照片。
现在,我希望大家都知道这个诊断。
免疫组化:Chromogranin+, synaptophysin+, GFAP-, EMA-, Pan CK-, calcitonin-
少数梭形细胞S - 100 是阳性。很抱歉我没有免疫组化的照片向您展示。
也给你此例的另一张照片。
现在,我希望大家都知道这个诊断。

- 广州金域病理
-
Some facts about paraganglioma:
n Mostly benign tumors, up to 12% malignant
n Composed of cells derived from the primitive neural crest
n Found in different locations;
n middle ear
n skull base
n pelvic floor
n Others
n Head and neck area, located near along the cranial nerves and the arterial vasculature
n Found commonly in association with the carotid body
n Rarely seen in :orbit, paranasal sinuses or thyroid
n Average age 50-60yrs
n M:F =(1:4)
n Presentation
n enlarging masses that are asymptomatic or associated with symptoms of mass effects
Some facts about paraganglioma:
n Mostly benign tumors, up to 12% malignant
n Composed of cells derived from the primitive neural crest
n Found in different locations;
n middle ear
n skull base
n pelvic floor
n Others
n Head and neck area, located near along the cranial nerves and the arterial vasculature
n Found commonly in association with the carotid body
n Rarely seen in :orbit, paranasal sinuses or thyroid
n Average age 50-60yrs
n M:F =(1:4)
n Presentation
n enlarging masses that are asymptomatic or associated with symptoms of mass effects
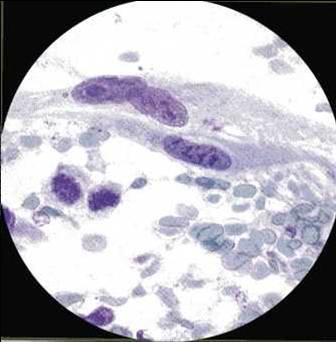
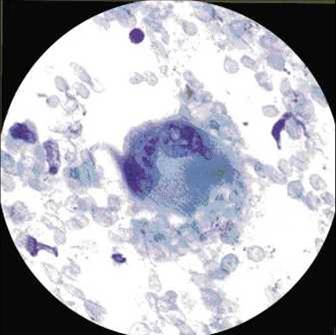
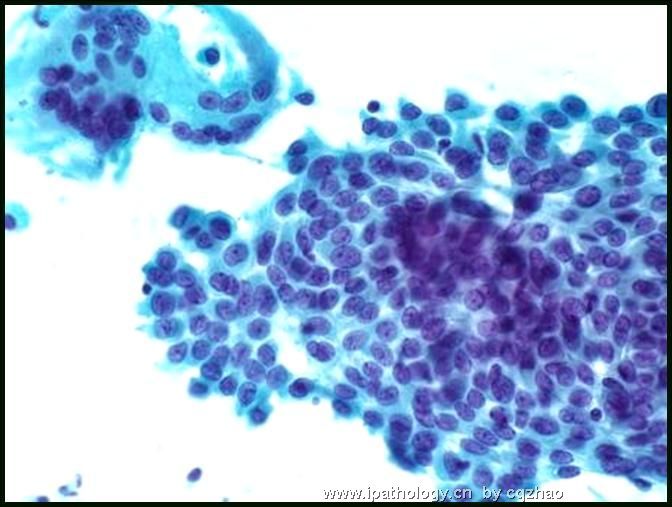
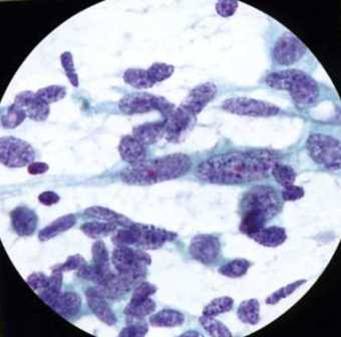
Paraganglioma-Cytomorphology
n Cellular/bloody
n Loosely cohesive, epitheloid and spindle cells
n Varies from uniform to pleomorphic
n Rosettes, Zellballen structures
n Reddish cytoplasmic granules on DQ
n Round/oval /spindle nuclei
n “Salt and pepper chromatin”
n Intranuclear cytoplasmic inclusions
n Cytology hardly recommended by surgeons because of risk of complications:
n Hemorrhage, damage to carotid body
n Distinction between benign and malignant CANNOT be made on cytology
n Require surgical excision with demonstration of metastases and NOT local invasion
-
本帖最后由 于 2008-12-30 11:25:00 编辑
Metastatic Adenocarcinoma-Cytomorphology
n Hypercellular, clusters and isolated cells
n Gland formation
n Nuclear pleomorphism, overlapping nuclei
n Nuclear hyperchromasia
n Irregular nuclear membranes
n Vacuolated cytoplasm
n IHC: Keratin +
名称:图1
描述:图1
-
本帖最后由 于 2008-12-31 02:26:00 编辑
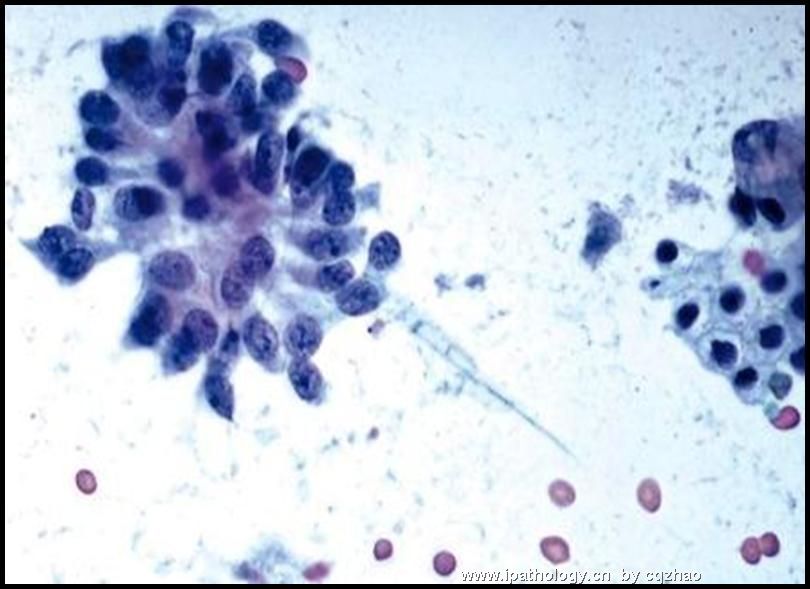
Metastatic papillary thyroid carcinoma
n Hypercellular, sheets, papillae, microfollicles
n Nuclear crowding, powdery chromatin
n Nuclei grooves, pseudoinclusions, nucleoli
n Cytoplasm-scant, squamoid, Hurthle-like or vacuolated
n Psammoma bodies, multinucleated giant cells,
n IHC: Thyroglobulin, TTF-1 +
名称:图1
描述:图1
名称:图2
描述:图2
-
本帖最后由 于 2008-12-30 11:31:00 编辑
Metastatic medullary thyroid carcinoma-Cytomorphology
n Numerous single cells or loose clusters
n Epitheloid/plasmacytoid/spindle
n Round nuclei
n Fine to coarse chromatin
n Inconspicuous nucleoli
n Nuclear pseudoinclusions
n Binucleation/multinucleation
n Amyloid
n IHC: Calcitonin, CEA,TTF-1, Thyroglobulin
名称:图1
描述:图1
Dr. Chen and I sent here some interesting and classical FNA cases here. It seems that people here are not very interested to these cases. I assume that most pathologists here do not do or sign out FNA cases in your clinical practice.
You have to attend the discussion if you want to learn sth from online. People are more likely to see one photo and give a guess diagnosis especially for Pap smears. I think it will not be very useful.
Anyway I conclude this case in the end of 2008. Happy New Year for every one.
cz











