











 需要仔细看看,再回答。
需要仔细看看,再回答。 


| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
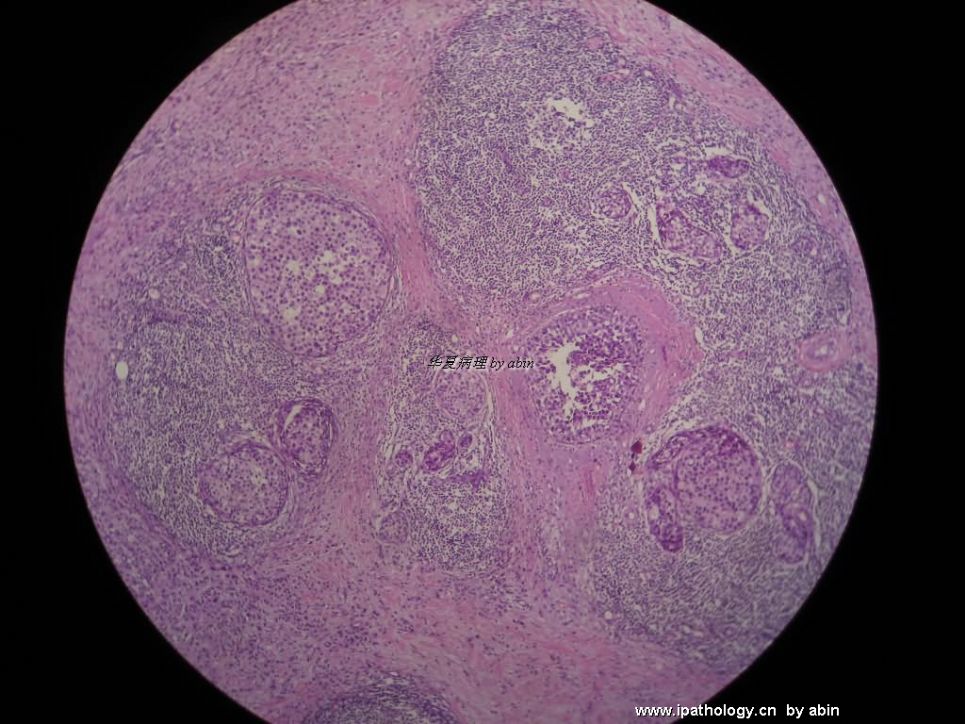
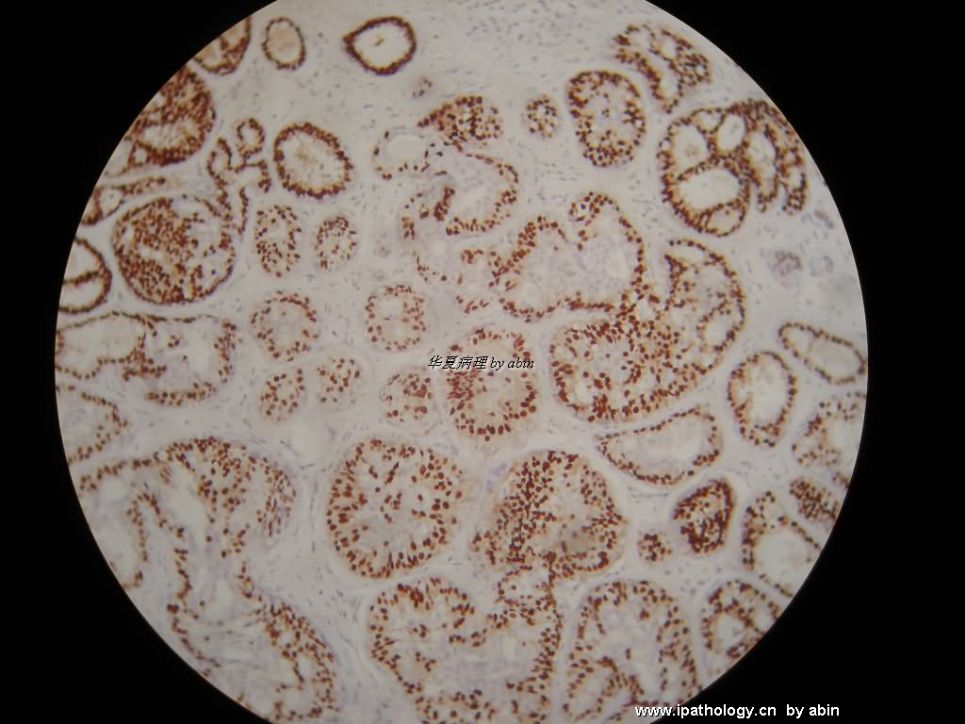
- B1575浸润性小叶癌中见到的
 图1
图1 图2
图2 图3
图3 图4
图4 图5
图5 图6
图6 图7
图7
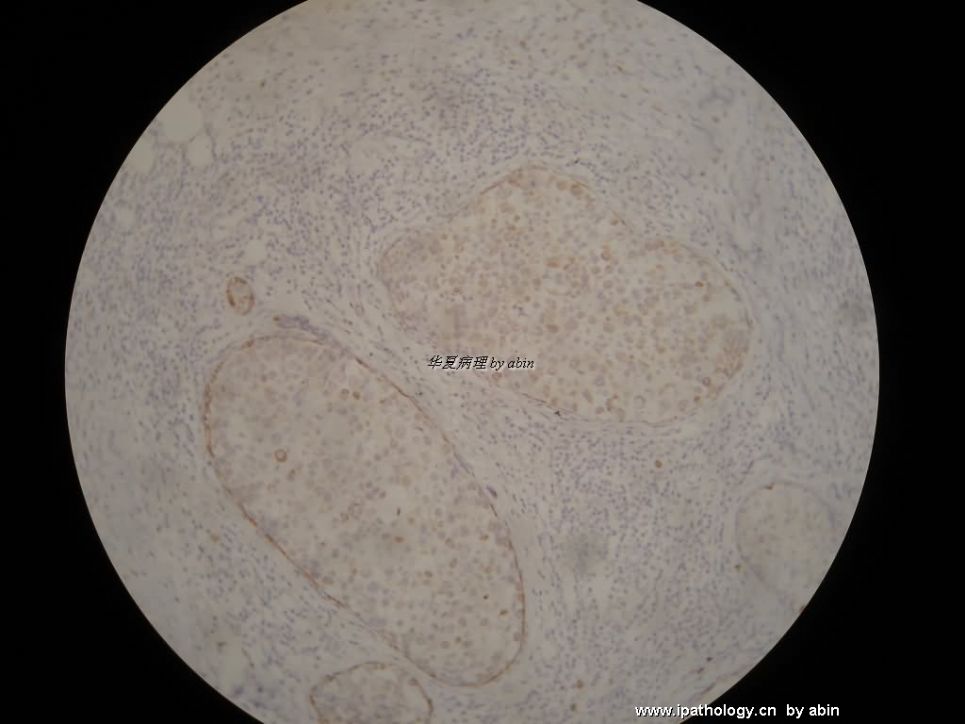
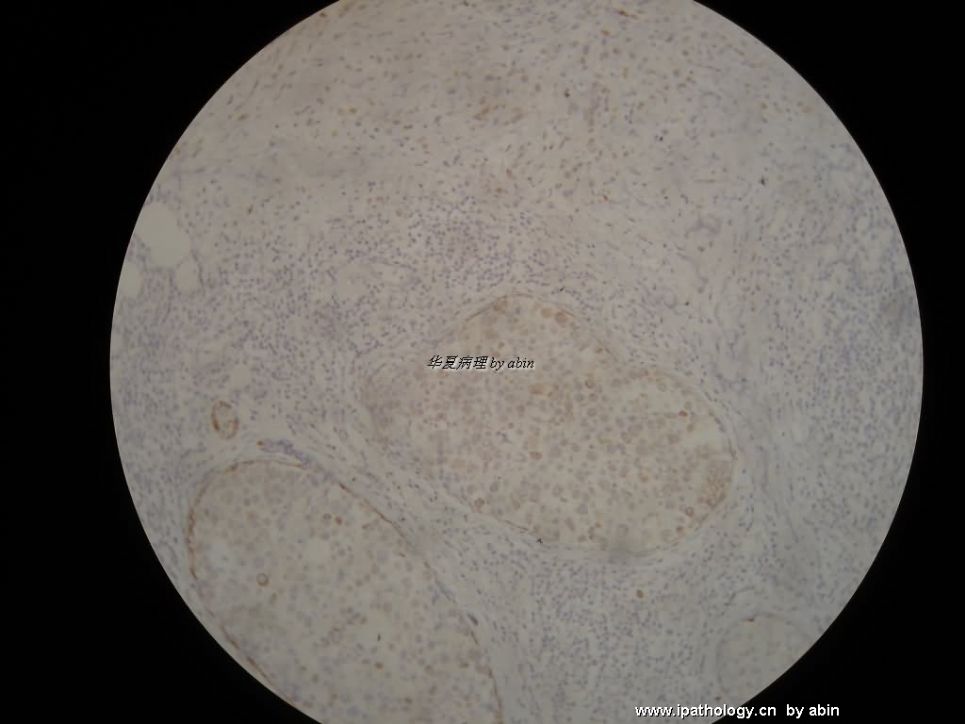
浸润性小叶癌中见到两个小叶/导管增生性病变。每个病变不超过一个4倍视野。拍摄时使用的最低倍为10倍。
它们出现在同一张切片中。
图1 HE 10X
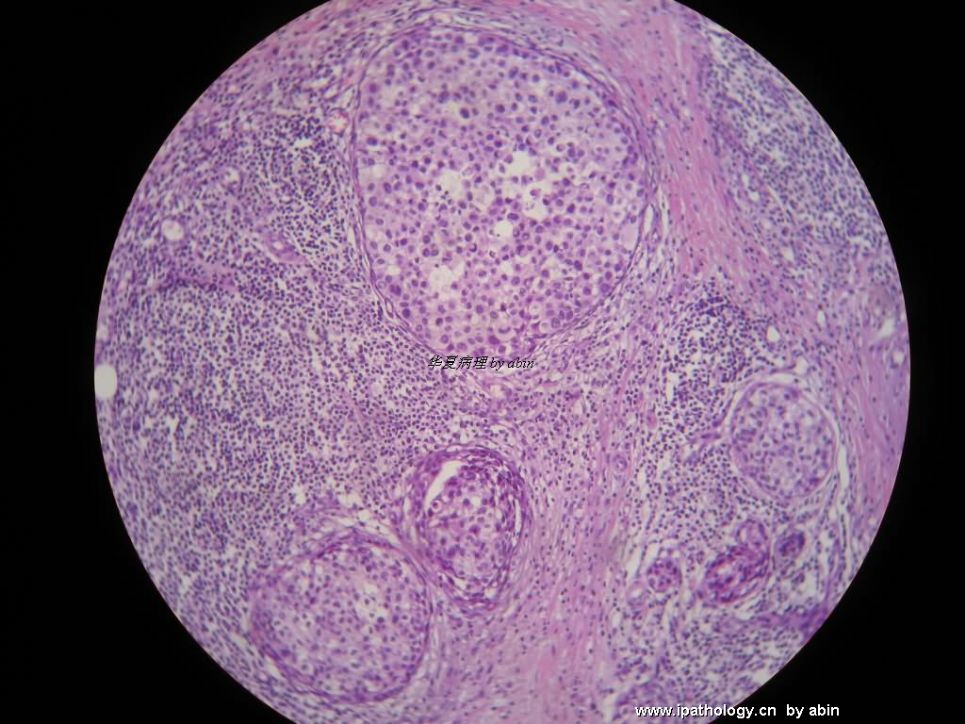
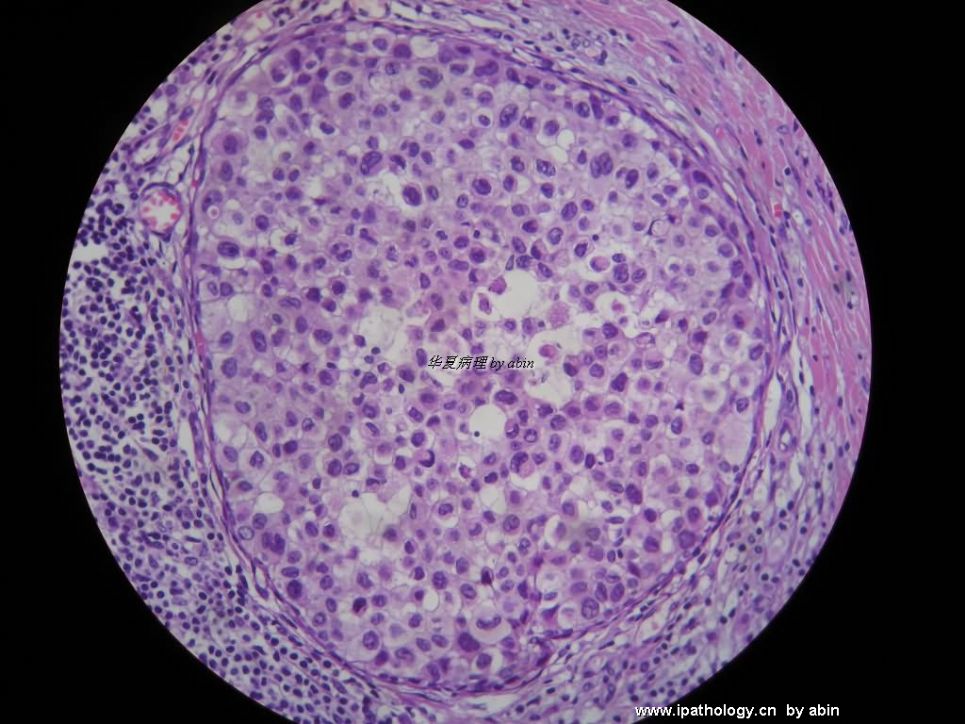
图2 HE 20X
图3 CK5/6 20X (背影太强,深棕色视为阳性,土黄色视为阴性)
图4 34BE12 20X
图5 E-Ca 20X
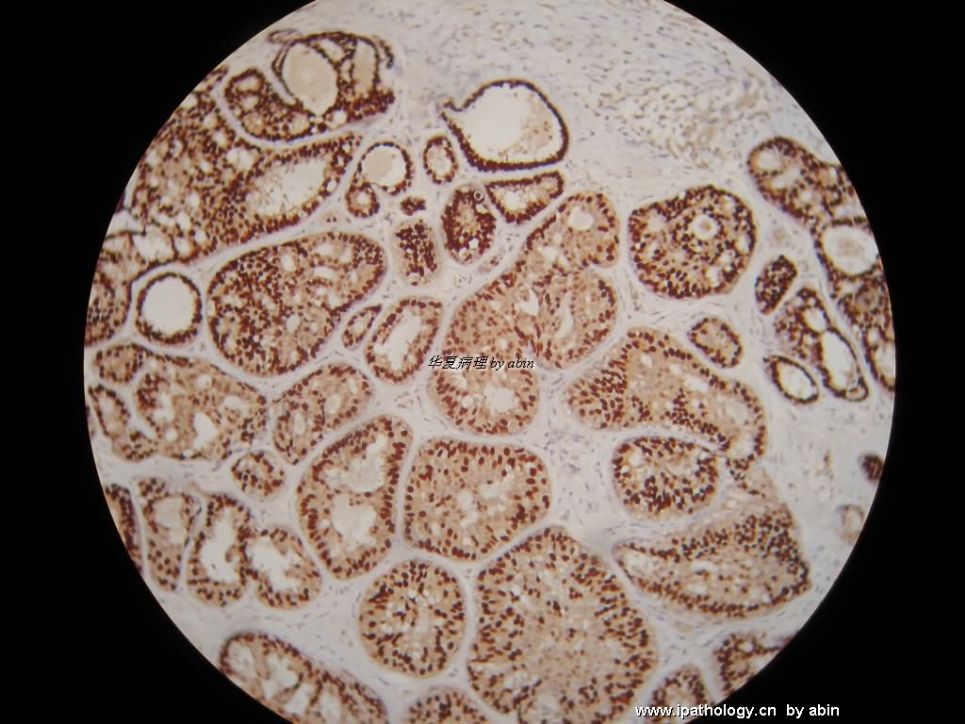
图6 ER 20X
图7 PR 20X
标签:UDH ADH DCIS LCIS P120 E-CAD
-
本帖最后由 于 2008-11-13 20:15:00 编辑

华夏病理/粉蓝医疗
为基层医院病理科提供全面解决方案,
努力让人人享有便捷准确可靠的病理诊断服务。
相关帖子
- • 乳腺包块。33岁
- • 乳腺肿物术后二年复发。
- • 乳腺穿刺
- • 浸润性小叶癌?
- • 乳腺腺瘤?
- • 左乳肿块,协助诊断
- • 女,42岁,切面实性,质硬,直径1厘米,边界不清,求会诊
- • 乳腺肿物
- • 乳腺肿物
- • 乳腺病理,会诊
×参考诊断
讨论意见:1楼为UDH+ADH,2楼为ILC+LCIS
First group photos: Main lesion is UDH. I am not sure if lobular lesion is present.
Second group photos: invasive lobular carcinoma and a lot of lobular carcinoma in situ.
For diagnosis purpose: IHC stains for E-cadherine and P-120 are good enough. CK5/6, 34be12 are useless.
For treatment purpose: ER, PR, Her2 should be done for invasive carcinoma.
-
stevenshen 离线
- 帖子:343
- 粉蓝豆:2
- 经验:343
- 注册时间:2008-06-03
- 加关注 | 发消息
-
本帖最后由 于 2008-11-16 21:42:00 编辑
I believe that there is ADH component in the 1st group; in 2nd group there is LCIS, possibly pleomorphic LCIS. Unless for teaching and research purpose, these immunostains are not particularly useful for diagnostic purpose. I believe that many people in this group are leaders in diagnostic pathology in China - communication about appropriate use of immunostains is important part of training and learning. Thanks.
abin译:我认为第一组图片存在ADH成分,第二组有LCIS,可能是多形性LCIS。除非为了教学和研究目的,这些免疫染色对诊断并无特别用途。我相信这里有很多国内病理科的领导,免疫组化的正确使用是培训和学习的重要内容。
-
zhoubingjuan 离线

- 帖子:261
- 粉蓝豆:366
- 经验:590
- 注册时间:2007-05-30
- 加关注 | 发消息
| 以下是引用天山望月在2008-11-16 20:22:00的发言: 2楼的图中,想请教abin免疫组化的问题: 图5 CK5/6 20X (背影太强,深棕色视为阳性,土黄色视为阴性),瘤细胞团周围是阳性肌上皮,瘤细胞也是黄色,算阳性还是阴性呢? 图6 34BE12 20X:是阳性还是阴性?(浅黄色) |
图5 CK5/6:肌上皮深棕色,阳性
图6 34BE12:原位成分和浸润成分均为弱阳性
这两项都做得不太好。
华夏病理/粉蓝医疗
为基层医院病理科提供全面解决方案,
努力让人人享有便捷准确可靠的病理诊断服务。
我们常用的乳腺癌标记物
ER,PR,HER2,p53,Ki67这些与预后和治疗目的有关。
E-Ca和34BE12用于鉴别导管癌或小叶癌。目前我们还没有p120。
CK5/6和34BE12,加上ER和PR,我们常用于帮助鉴别UDH/ADH/DCIS。
p63,SMA,calponin用于标记肌上皮。
估计国内大多数病理科都是这样在用的,不知道国外的使用情况?看来确实存在认识上的差别。
不当之处欢迎指出。谢谢!
华夏病理/粉蓝医疗
为基层医院病理科提供全面解决方案,
努力让人人享有便捷准确可靠的病理诊断服务。
-
stevenshen 离线
- 帖子:343
- 粉蓝豆:2
- 经验:343
- 注册时间:2008-06-03
- 加关注 | 发消息
To Abin: These are very helpful information. The most important thing is share experience and knowledge. We might have small differenences, and you might be correct. We all agress that immunostains are very helpful and necessary in practice of pathology. These stains have to provide useful information that can be used diagnostically, prognositically or to guide treatment choices. Whether these stains are useful or not will based on evidence (clinical trials), well designed studies and practice standard, and our experience. We all learn from our teachers, our colleagues, meetings, books, and publications.
Our experience may only represent a larger academic and private hospitals:
ER,PR,HER2,p53,Ki67这些与预后和治疗目的有关:
(We do ER, PR, Her2/neu, and Ki67 for invasive carcinoma, ER and PR for DCIS)
E-Ca和34BE12用于鉴别导管癌或小叶癌。目前我们还没有p120。
(E-Ca rarely used to differentiate DCIS or LCIS, no experience with 34BE12 and p120)
CK5/6和34BE12,加上ER和PR,我们常用于帮助鉴别UDH/ADH/DCIS。
(We do not use these stains for differentiate UDH/ADH/DCIS, should be morphologic diagnosis, if you summarize your data and prove that they are useful, I am sure that it will be publishable)
p63,SMA,calponin用于标记肌上皮。
(Only in situations that need to prove microinvasion or SUSPICIOUS for invasion - DCIS or LCIS involving sclerosing adenosis, papillary lesion, small area suspicious for tubular carcinoma, invasive cribriform carcinoma etc.)
谢谢Dr. Stevenshen!
翻译如下:
abin,你提供了很有帮助的信息。最重要的是分享经验和知识。(在免疫组化使用方面)我们可能存在一点差别,你也可能是对的。我们都认为免疫染色在病理实际工作中很有帮助很必要。这些染色可以提供有用的信息,用于诊断、预后或指导治疗。这些染色是否有用,要有依据,如临床试验、精心设计的研究和实际标准,以及我们的经验。我们都是从老师、同事、书本和出版物上学来的。
我们的经验可能只代表一些较大的学术机构和私人医院:
我们对浸润癌做ER, PR, Her2/neu, and Ki67,对DCIS做ER and PR。
很少用E-Ca鉴别DCIS或LCIS,没有使用34BE12 and p120的经验。
我们不用CK5/6和34BE12,加上ER和PR来鉴别UDH/ADH/DCIS,而是根据形态诊断。如果你总结数据并且证明它们有用,我相信是可以发表的。
p63,SMA,calponin用于标记肌上皮:仅在需要证明微小浸润或可疑浸润的情形下使用,如:DCIS或LCIS累及硬化性腺病,乳头状病变,小区可能小管癌,浸润性筛状癌等。
华夏病理/粉蓝医疗
为基层医院病理科提供全面解决方案,
努力让人人享有便捷准确可靠的病理诊断服务。
Agree with Dr. Shen:
Inv ca: ER, PR, Her2 must be done for treatment. Some hospitals do ki67, some not. We do it now.
DCIS: ER, PR
we do e-cadherin and/or p120 for almost all lobular carcinoma. We learned the lession from clinical practice that some cases look like ductal ca and turn out to be lobular ca, and some look like lobular ca and turn out to be ductal ca. Of cause you do not need to do it if you feel ok. In fact the treatment is similar.
Again, IHC can not help you for dx of udh, adh, dcis. I used them a lot before and confirm they are useless.
| 以下是引用cqzhao在2008-11-18 9:03:00的发言并翻译:
同意Dr. Shen: 浸润癌:ER, PR, Her2是治疗目的必须的检测项目。一些医院做ki67,另一些不做。我们现在做。 DCIS: ER, PR 几乎所有小叶癌,我们都做E-Cadherin and/or p120。 有些看似导管癌结果变成小叶癌,也有相反情况。当然如果你很有把握,可以不做。实际上,它们的治疗相似。 重复一下,IHC对UDH、ADH、DCIS的诊断无帮助。我以前做过很多,确信它们没有用途。 |
华夏病理/粉蓝医疗
为基层医院病理科提供全面解决方案,
努力让人人享有便捷准确可靠的病理诊断服务。











