
图1")
图2")
图3")
图4")








| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
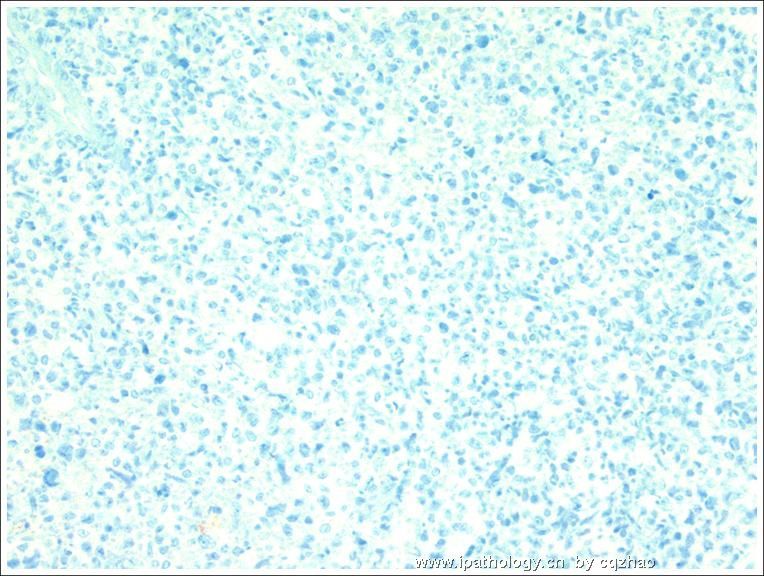
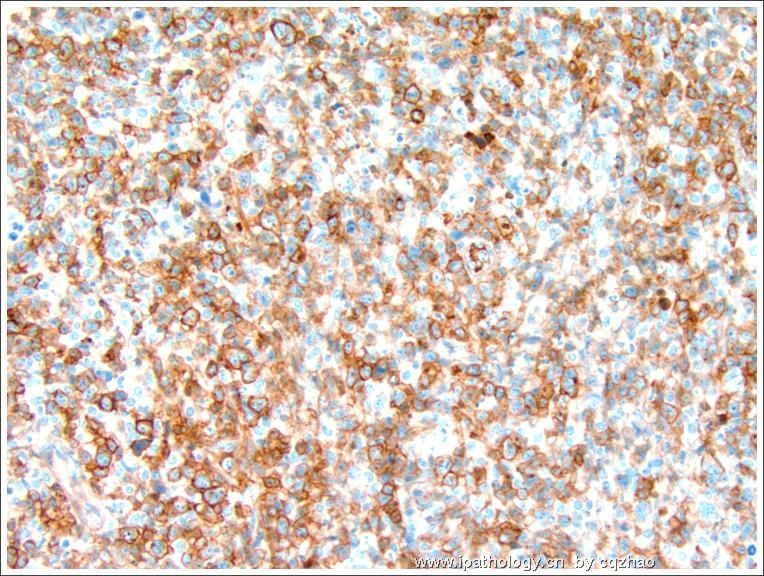
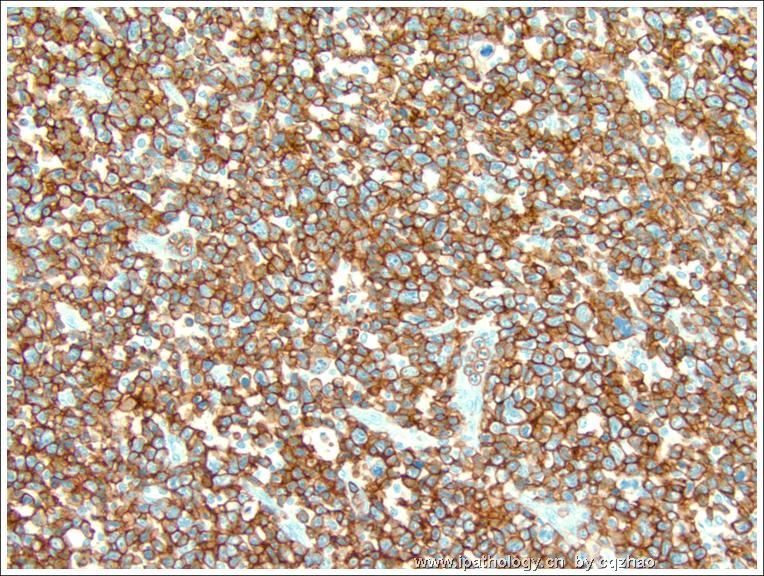
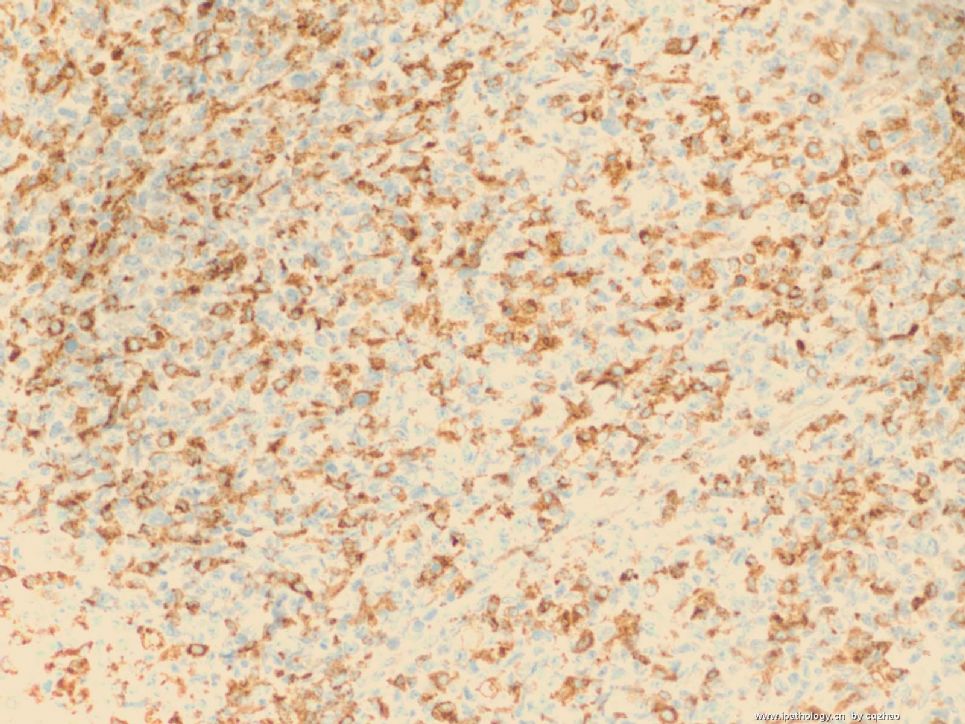
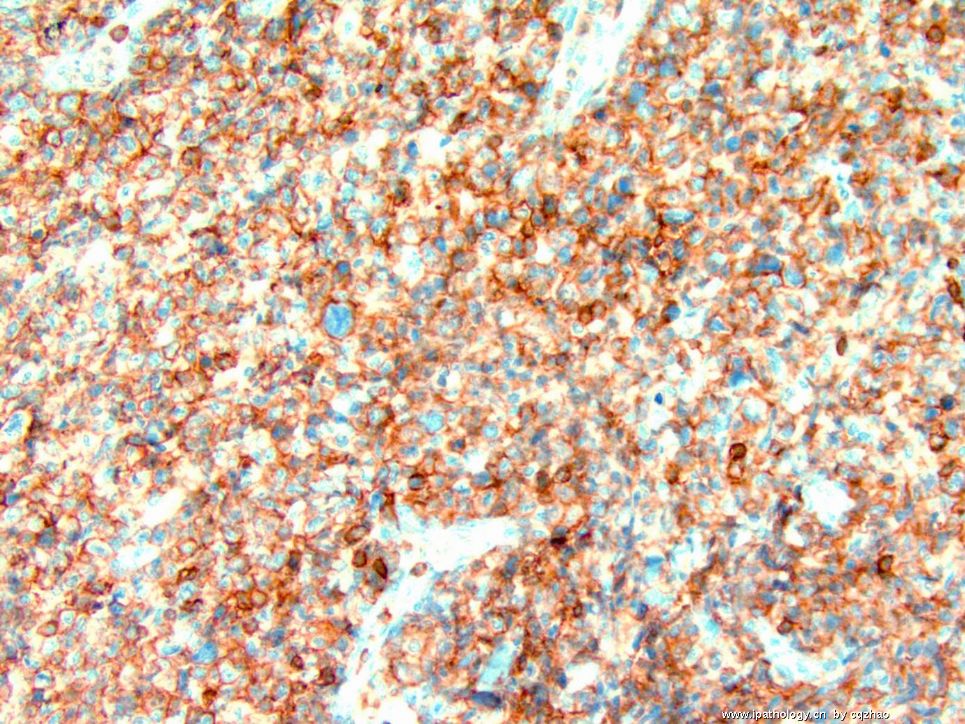
- B1278Vulvar anaplastic large T cell lymphoma ALK-1 negative (cqz1)
图1") 图1
图1图2") 图2
图2图3") 图3
图3图4") 图4
图4
| 姓 名: | ××× | 性别: | F | 年龄: | 65-70 |
| 标本名称: | Vulvar lesion | ||||
| 简要病史: | |||||
| 肉眼检查: | |||||
Just signed a case two weeks ago and like to share it with all friends here.
Vulvar mass 5 cm. No previous malignant history.
Fig Key:
Fig 1. 2x
Fig 2. 20x juction
Fig 3. 20x tumor
Fig 4. 40x tumor
Tumor shows similar morphology in different areas.
Please give your differential dx and the requirement for IHC stains if it is your case. What is your favor diagnosis based on the H&E slides?
I will have few weeks vocation and will poster the immunostain photos or results after I come back.
Thnaks,
标签:ATCL ALK阴性
-
本帖最后由 于 2009-02-25 09:47:00 编辑
×参考诊断
ATCL,ALK阴性
-
本帖最后由 于 2008-11-12 22:27:00 编辑
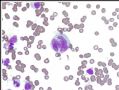 图1
图1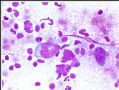 图2
图2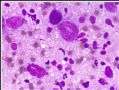 图3
图3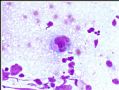 图4
图4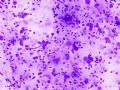 图5
图5 图6
图6 图7
图7 图8
图8
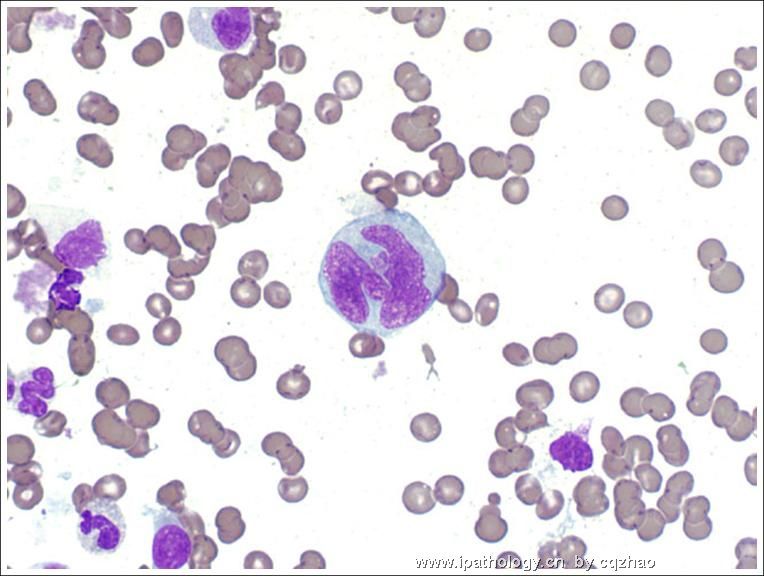
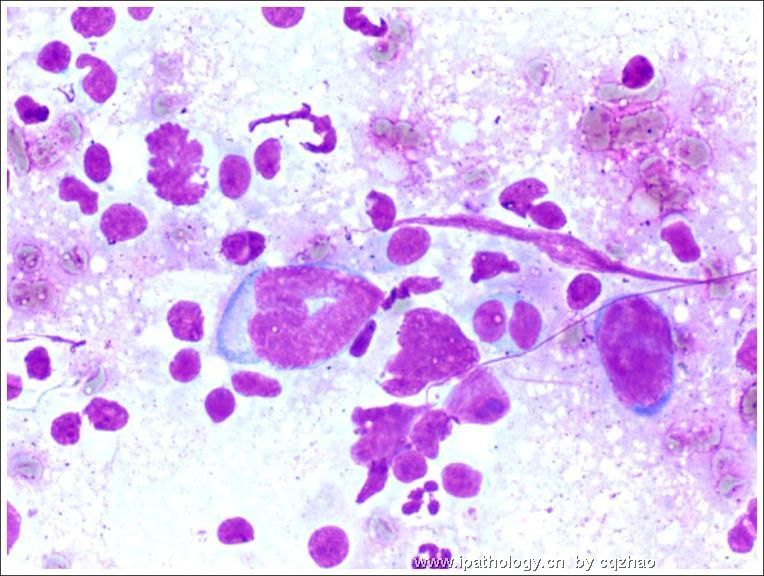
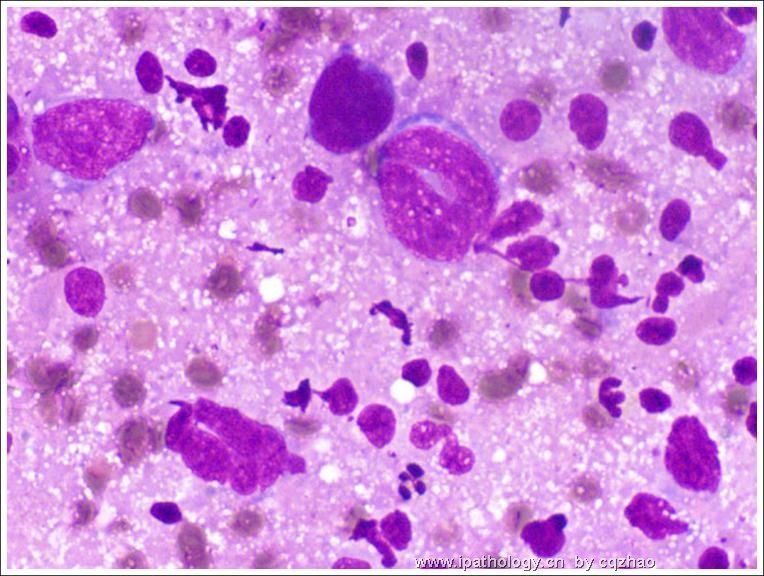
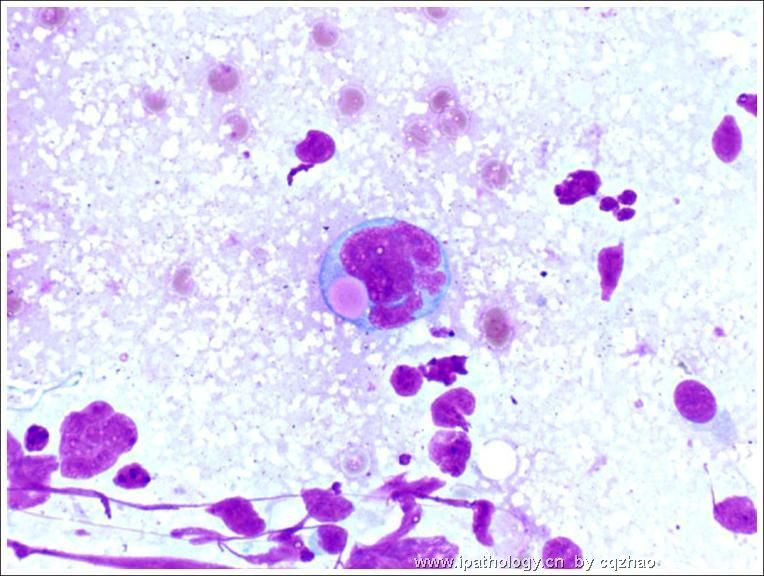
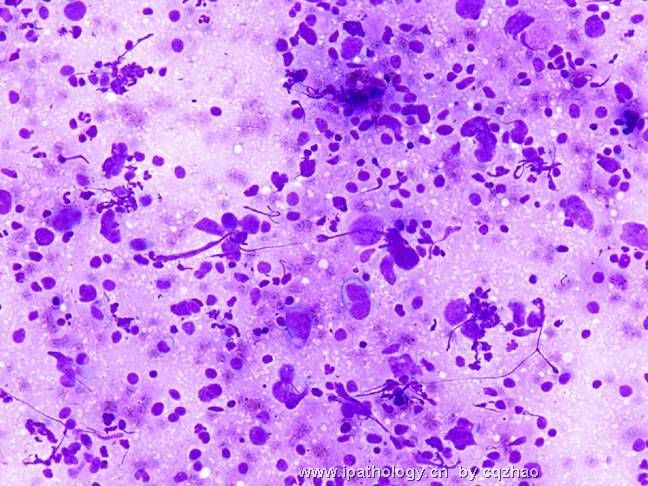
After the original dx of valvar lesion, an enlarged LN was found in pelvic area. FNA was performed.(外阴病变诊断后,发现盆部肿大淋巴结1枚,行FNA)
Fig 1-5 cytology of lymph node FNA. (图1-5为淋巴结FNA细胞学)
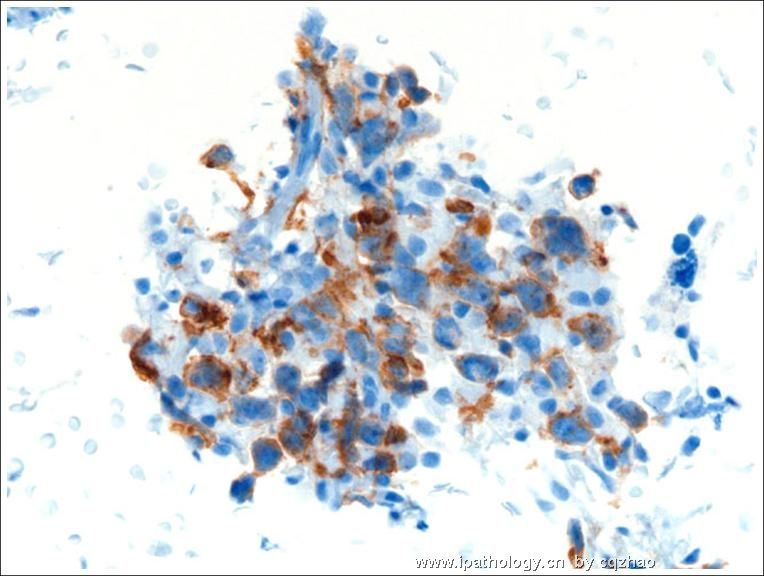
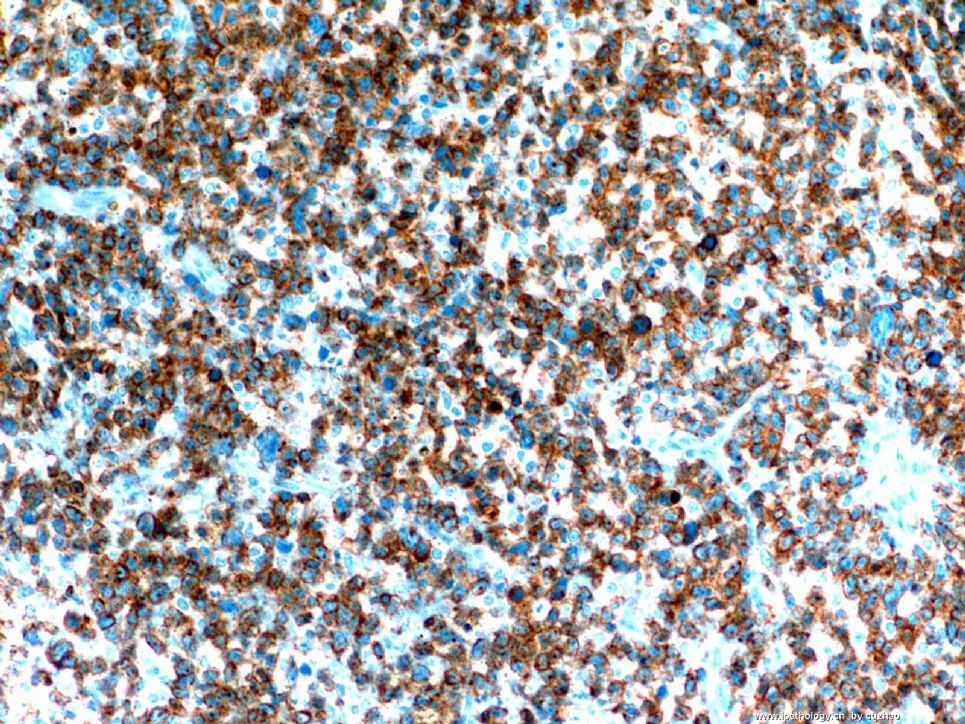
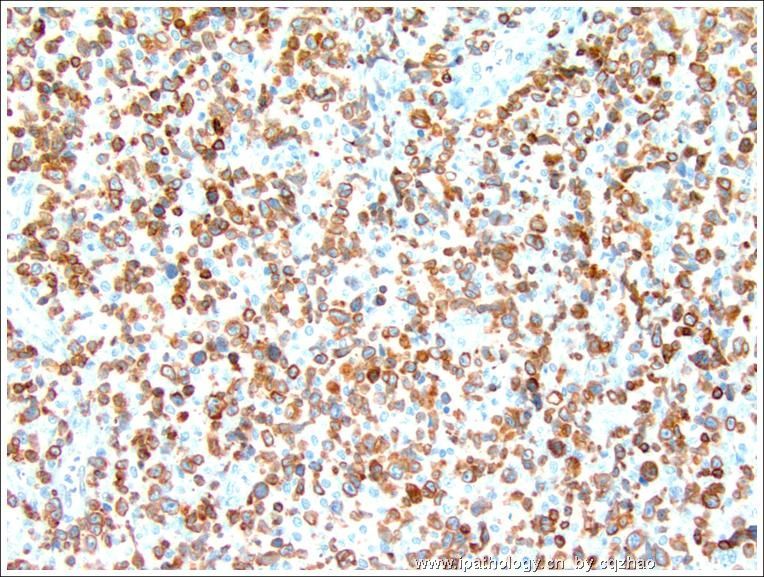
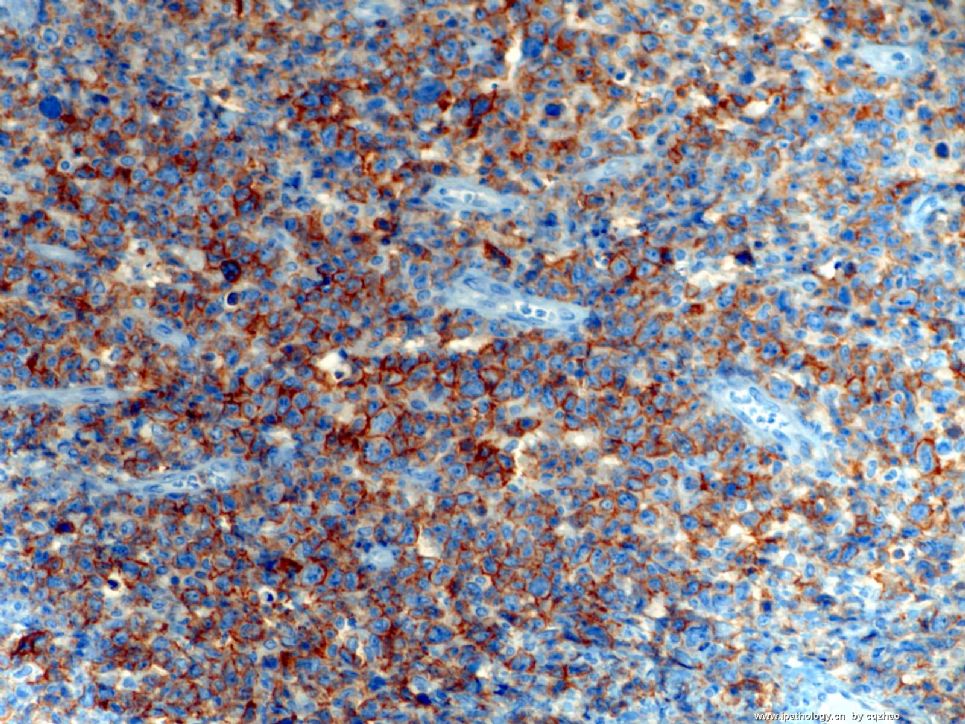
Fig 6: CD3
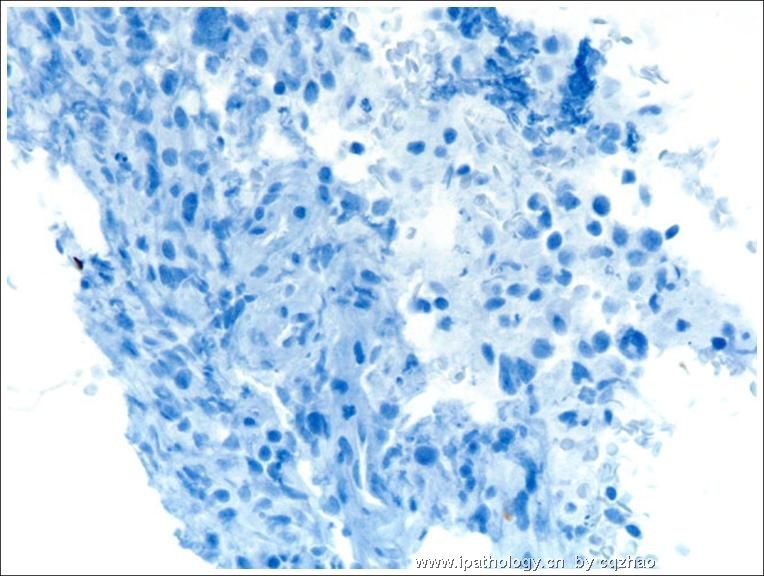
Fig 7: CD20
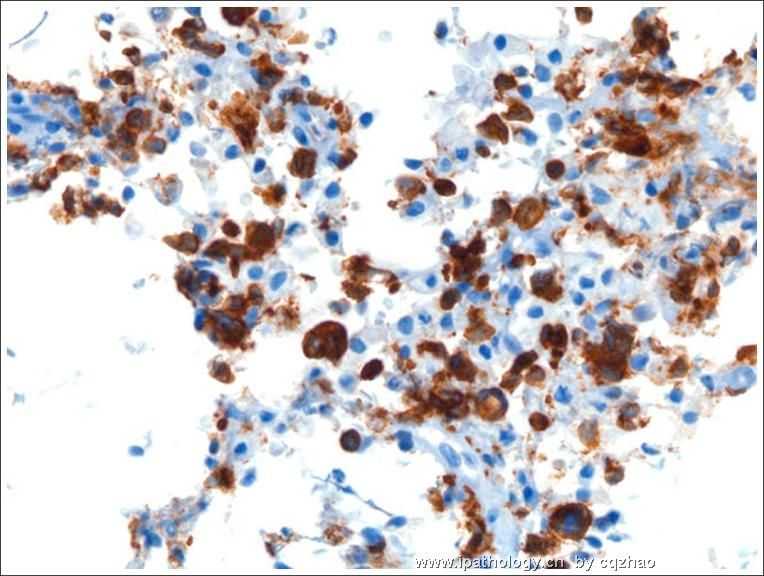
Fig 8: CD30
All other IHC results in cell block are the same as that in valvar lesion.
molecular analysis of ALK is negative. (细胞块其余IHC结果与外阴病变相同。分子学检测ALK阴性)
-
本帖最后由 于 2008-11-11 17:58:00 编辑
thank all of you for your discussion. After I got the first IHC results, I sign-out the case as hemologic/lymphocytic malignancy and sent the case to our hemotopathologist for further evaluation. The final dx is ATCL , ALK neg.
Thank Abin's excellent analysis. I especially appreciate the first reviewer WY1992. You are great you can consider T cell lymphoma immediately. In fact Lymphoma is my last consideration. Ha ha.
I will present more follow-up data soon.
abin译:谢谢大家参与讨论。第一批IHC结果,我签发了造血/淋巴系统恶性肿瘤,然后转给我们的血液病理医生进一步分型。
最后诊断:ATCL,ALK阴性。
谢谢abin,分析非常好。特别赞赏第一个发表意见的WY1992,能立即考虑到T细胞淋巴瘤。实际上淋巴瘤是我的最后考虑,哈哈。我将提供更多随访资料。
-
本帖最后由 于 2008-11-11 17:53:00 编辑
-
Peripheral T-cell Lymphoma With Follicular T-cell Markers.
To: Shiyan:
I am an gyn/breast pathologists and cytopathologist, very short of knowledge in hematopath. I am sure that you know much more than I know. I find a good paper PTCL. I can email you the full paper if you want to and told me your email.
Am J Surg Pathol. 2008 Sep 5. [Epub ahead of print]
那Granzyme B,EMA,CD56呢?从T细胞的表达上,我认为CD20应该是真阴性,但是在所提供的图片中没有见到阳性信号,好像这个染色不是很漂亮了,呵呵。
这个部位的T细胞淋巴瘤还真是少见。我前一段时间总结了80多例ALCL,没有一例是在宫颈的。现在的免疫表型确实可以诊断ALCL,但是还是想知道其他的免疫表型。还有一个问题就是:ALK-ALCL和PTCL-NOS怎么鉴别?PTCL也是可以表达CD30的。不知道老师在美国是怎么鉴别的?
谢谢老师提供的好病例。不过现在回过头来重新看病例,我还是会首先想到DLBCL,不会马上定位到ALCL,即使一些细胞形态很像,我仍然会首先想到这个部位常见的肿瘤(有点死脑筋噢),呵呵。再次感谢老师!
| 以下是引用abin在2008-10-29 18:32:00的发言:
再次学习,并参考了陈国璋教授的讲课资料。 如果是淋巴造血系统肿瘤: LARGE CELL HEMATOLYMPHOID NEOPLASMS: Main considerations
Abundant pink cytoplasm: Histiocytic/ dendritic cell tumor
 |
Abin has done great job on this case and I am with him for differential diagnoses.
澄泉兄,别掉我们的胃口了,给个结果吧,我们都望眼欲穿了。
于北京机场等机厅

- 不坠青云之志,长怀赤子之心
Thank all of you who read the case and wrote your differential dx. I just came back from China last weekend and sorry for the delay.
IHC:
Vimentin Positive
Epithelial markers negaative: AE1/AE3, Cam 5.2, CK7, CK20
Melanoma markers negative: Melan-A, HMB-45, S-100
Muscle markers negative: SMA, Desmin,
LCA (CD45) See photo
-
本帖最后由 于 2008-10-29 18:42:00 编辑
再次学习,并参考了陈国璋教授的讲课资料。
如果是淋巴造血系统肿瘤:
LARGE CELL HEMATOLYMPHOID NEOPLASMS: Main considerations
--Diffuse large B-cell lymphoma
--Anaplastic large cell lymphoma
--T or NK cell lymphoma predominated by large cells
--Anaplastic plasmacytoma / plasmablastic lymphoma
--Classical Hodgkin lymphoma predominated by large cells
==Histiocytic / dendritic cell neoplasm
==Pleomorphic variant of mantle cell lymphoma
Abundant pink cytoplasm: Histiocytic/ dendritic cell tumor
华夏病理/粉蓝医疗
为基层医院病理科提供全面解决方案,
努力让人人享有便捷准确可靠的病理诊断服务。











