
图1")
图2")
图3")
图4")
| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
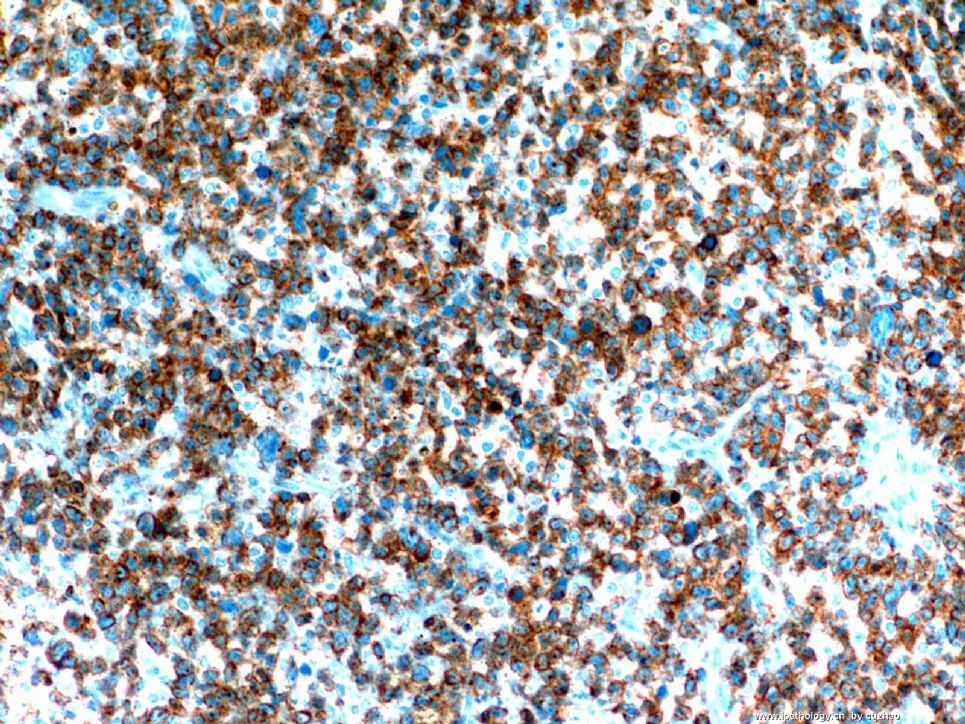
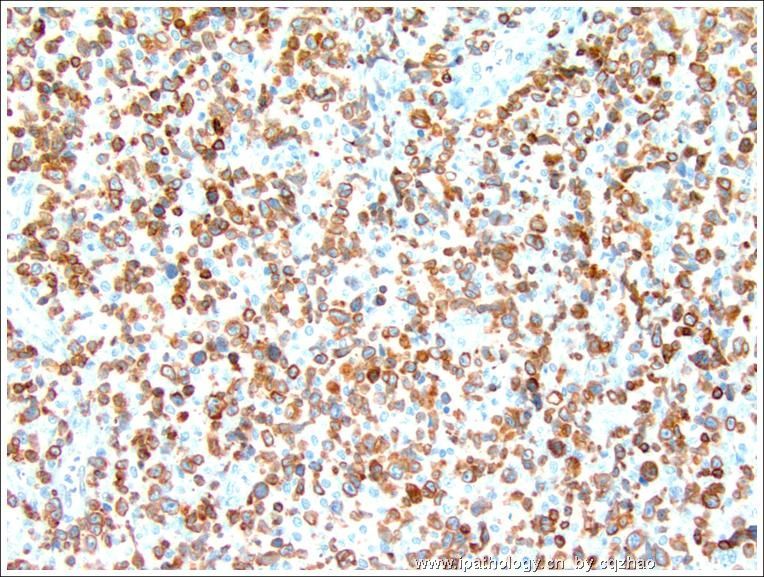
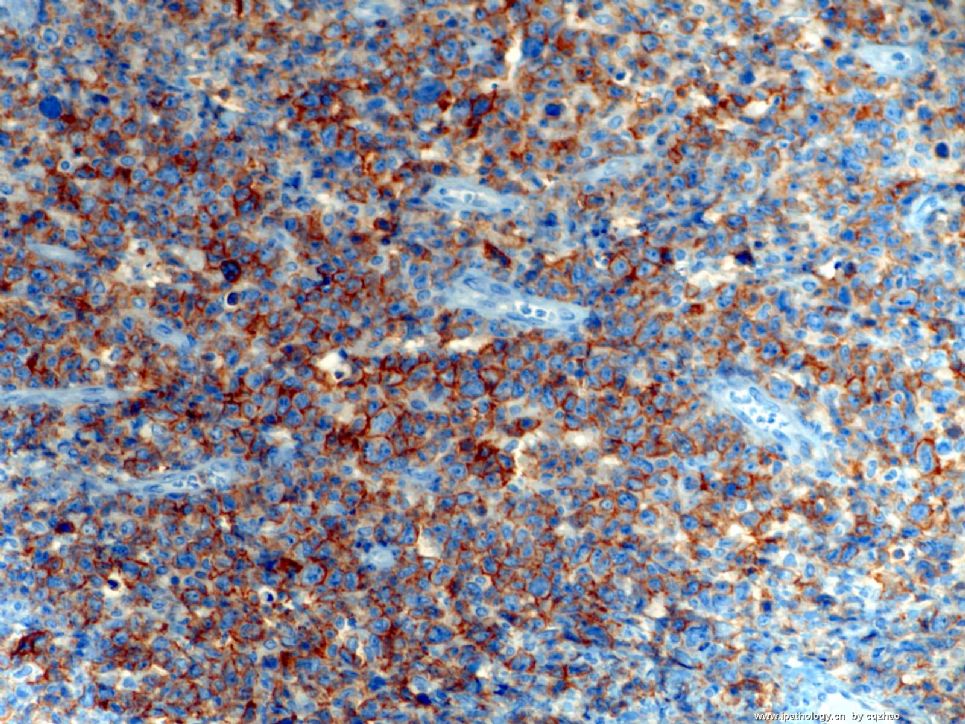
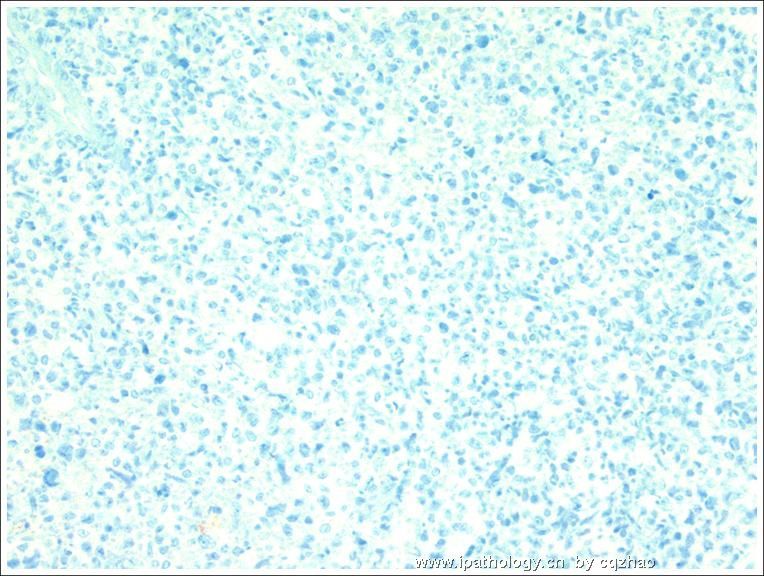
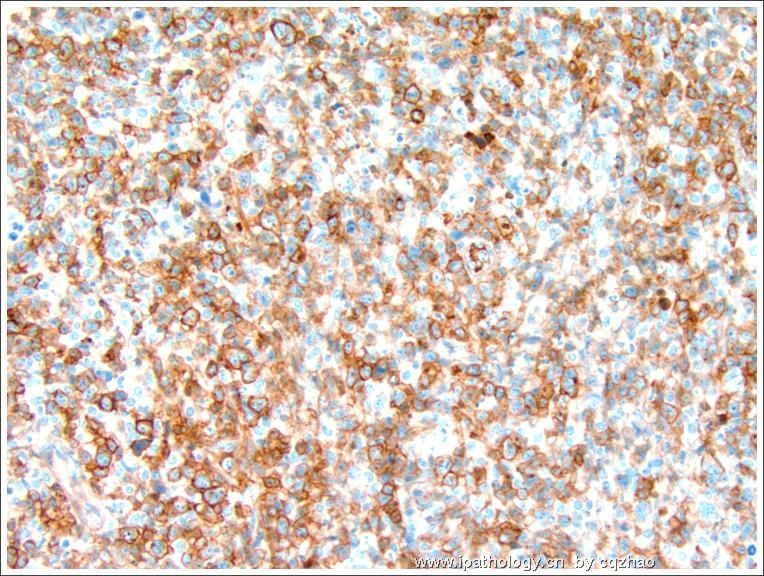
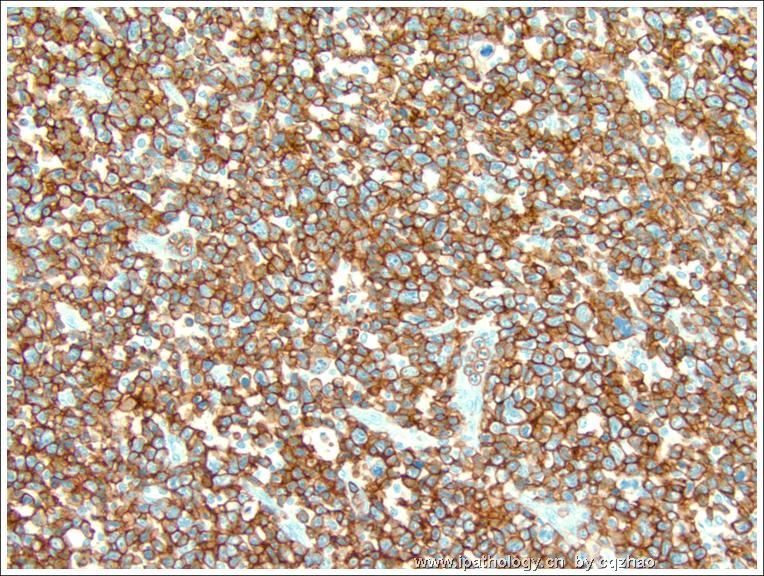
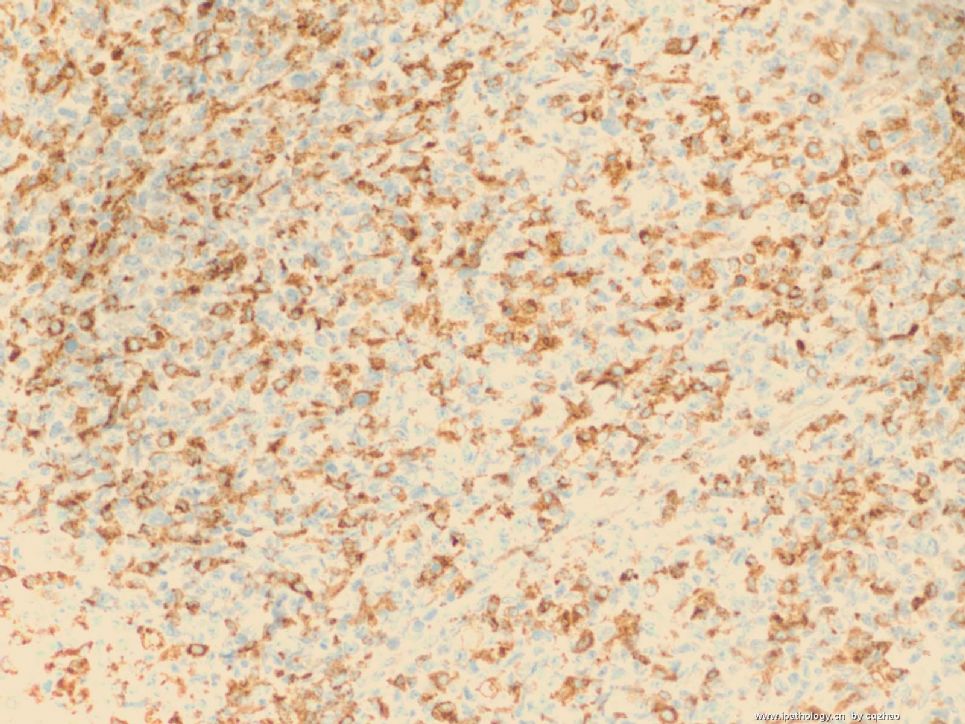
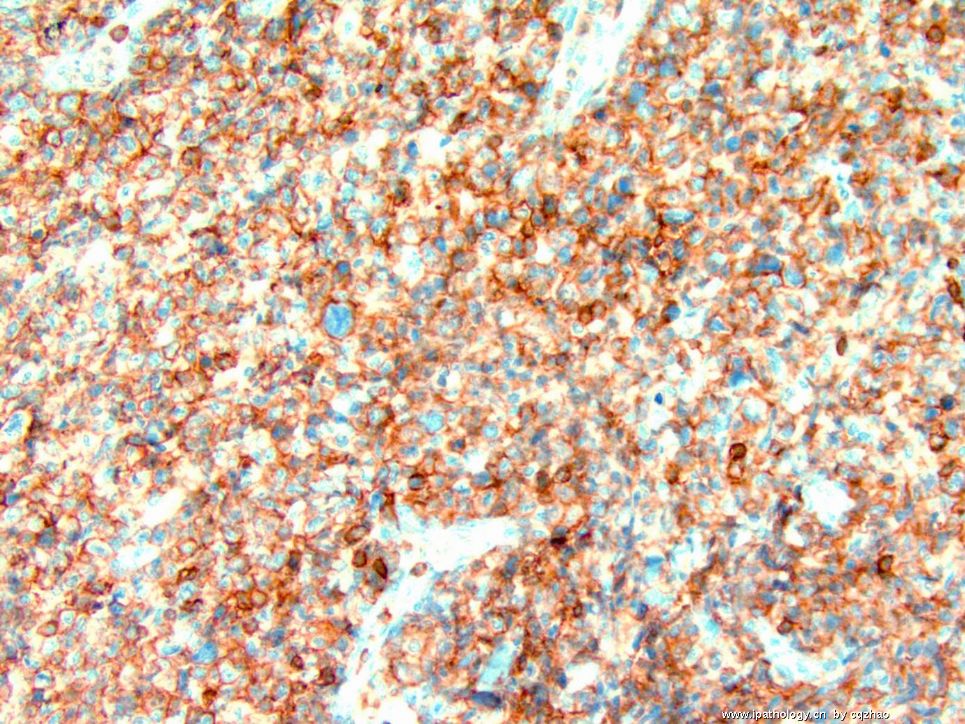
- B1278Vulvar anaplastic large T cell lymphoma ALK-1 negative (cqz1)
图1") 图1
图1图2") 图2
图2图3") 图3
图3图4") 图4
图4
| 姓 名: | ××× | 性别: | F | 年龄: | 65-70 |
| 标本名称: | Vulvar lesion | ||||
| 简要病史: | |||||
| 肉眼检查: | |||||
Just signed a case two weeks ago and like to share it with all friends here.
Vulvar mass 5 cm. No previous malignant history.
Fig Key:
Fig 1. 2x
Fig 2. 20x juction
Fig 3. 20x tumor
Fig 4. 40x tumor
Tumor shows similar morphology in different areas.
Please give your differential dx and the requirement for IHC stains if it is your case. What is your favor diagnosis based on the H&E slides?
I will have few weeks vocation and will poster the immunostain photos or results after I come back.
Thnaks,
标签:ATCL ALK阴性
-
本帖最后由 于 2009-02-25 09:47:00 编辑
×参考诊断
ATCL,ALK阴性
-
本帖最后由 于 2008-11-14 20:10:00 编辑
| 以下是引用abin在2008-11-13 20:58:00的发言: 谢谢Dr.cqzhao纠正。我猜fellow是住院医师,fellowship training 是住院医师培训。说不定又猜错了,哈哈。期待Dr.cqzhao有空给我们谈谈这方面的中美差别。 |
住院医师=residents
Fellow: One year of subspecielty training after the residency training (now pathology 4 years), such as gynecologic pathology, hemato pathology, GI pathology et al. They are not attending pathologists. It is not a job. I am happy to talk about these in future on tele.
abin译:
Fellow: 住院医生培训之后的一年亚专业培训(现在病理专业的培训是4年),如妇科病理,血液病理,消化病理等。他们不是病理主治医生(?attending pathologists?汗,又要猜了),也不是一门职业。我很乐意以后远程谈谈这些。
Thank abin for the excellent translation.
Fellow does not mean colleaque. In the US you need four years of pathology residency training after the medical school. Most people will do one or two fellowship training in some subspecieties. It needs one year of fellow training. So fellow means one subspecilty training after residency training. Pathology fellows include many subspecieties, GI, gynecology, breast, derm, hematology, GU, ENT et al.
Above lymph node is inguinal LN.
This case was present by our GYN fellow in the dept conference. I share some of her summary with you.
¢ Primary extranodal lymphoma involving the female genital tract ranges from 0.2 to 1.1%.
l Cervix and ovaries most frequent, then uterine corpus and vagina, with vulva and fallopian tubes least common.
¢ Disseminated lymphoma secondarily involves the female genital tract in 7 to 30% of cases.
l Ovary most commonly, then uterus.
¢ Patients with vulvar lymphoma tend to be older than patients with lymphoma at other sites, mean 60 years.
¢ DLBCL is the most common lymphoma affecting the female genital tract (except in fallopian tube).
¢ In vulva, DLBCL is most frequent, with follicular lymphoma next.
ALCL, ALK Positive
¢ Accounts for approximately 3% of adult non-Hodgkin lymphomas.
l 10-20% of childhood.
¢ ALK-positive is most frequent first three decades of life, and shows male predominance.
¢ Usually involves LN and extranodal sites.
l Most frequent skin (21%), bone (17%), soft tissue (17%), lung (11%), and liver (8%).
¢ Bone marrow involvement 10% with H&E.
l Increased to 30% when immunostains for CD30, EMA and/or ALK applied.
¢ Broad morphologic spectrum.
¢ All show cells with eccentric, horseshoe- or kidney-shaped nuclei = “hallmark cells”.
¢ Multiple nuclei may occur in a wreath-like pattern.
¢ In general, more abundant cytoplasm than most lymphomas.
¢ CD30 positive in a membranous pattern.
¢ Translocation t(2;5)-NPM/ALK is most frequent genetic alteration.
l Shows nuclear and cytoplasmic staining.
l Fusion of ALK protein, usually transmembrane with NPM, nuclear transport protein.
¢ ALK expression virtually specific for ALCL.
¢ Absent from most other human neoplasms.
l Rare DLBCL.
l Rare cases of rhabdomyosarcoma.
l Inflammatory myofibroblastic tumors.
¢ Majority positive for EMA.
¢ Vast majority express one or more T-cell antigens; CD4+/CD8-.
¢ Variably positive for CD45.
¢ Most positive for cytotoxic-associated antigens TIA1, granzyme B, and/or perforin.
¢ 90% show clonal rearrangement of T-cell receptor.
¢ EBV is always absent.
ALCL, ALK Negative
¢ Included as provisional entity in most recent WHO.
l “CD30+ T-cell neoplasm not reproducibly distinguishable on morphological grounds from ALCL, ALK+”.
l Older median age and more aggressive clinical course than ALK+ ALCL.
¢ Considered distinct from peripheral T-cell lymphoma, NOS, but distinction is not always straightforward.
¢ Peak incidence 40-65 years.
¢ Male predominance, 1.5:1.
¢ Involves lymph nodes and extranodal sites, but less commonly than ALCL, ALK+.
¢ Tumor cells larger and more pleomorphic.
¢ More than half of cases express one or more T-cell markers; CD4+/CD8-.
¢ More likely to be positive for CD2 and CD3.
¢ Fewer positive for EMA.
¢ Majority show cytotoxic-associated markers.
¢ Most show clonal rearrangement of T-cell receptor.
¢ No recurrent cytogenetic abnormalities.
ALCL, ALK Negative DDx
¢ Differential diagnosis
l Primary cutaneous ALCL
l Other primary cutaneous CD30+ lymphoproliferative disorders
• But lymphomatoid papulosis (LyP) is, by definition, limited to skin
l Peripheral T-cell lymphoma, NOS
¢ Primary cutaneous ALCL
l Disease is limited to skin at time of diagnosis.
l Extracutaneous dissemination may occur, mainly to regional lymph nodes.
l Predominantly in adults and elderly.
l T-cell phenotype with variable loss of CD2, CD5 and/or CD3; CD30 expression >75% cells.
l Most cases negative for EMA and ALK.
l Overall 5-year survival rate of 90%.
¢ Peripheral T-cell lymphoma, NOS
l May be nodal or extranodal; skin and GI tract most common.
l Abnormal medium to large lymphocytes often admixed with inflammatory cells.
l Sinus pattern of LN infiltration is absent.
l T-cell phenotype; CD4+/CD8-.
l More likely to be positive for CD2, CD3.
l CD30 may be seen, but usually with variable intensity, and not in strong, homogeneous, membranous pattern.
Conclusions
¢ Lymphoma, primary or secondary, is rare in the vulva.
¢ Most common type is DLBCL.
¢ Tend to occur in older women.
¢ ALCL, systemic and primary cutaneous types.
l ALCL, ALK-negative provisional entity in new WHO.
l Evidence that ALK+ ALCL, ALK- ALCL, and PTCL, NOS are distinct entities.
¢ Lymphoma should be included in the differential diagnosis of vulvar mass.
We did not find valvar ALCL report in literature serach. I asked the fellow to write a case report.
Now you see all of the case already.
Thank for discussion and reviewing of this case.
, then uterus
-
本帖最后由 于 2008-11-12 22:27:00 编辑
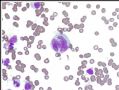 图1
图1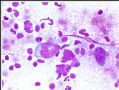 图2
图2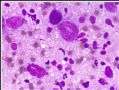 图3
图3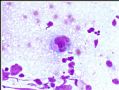 图4
图4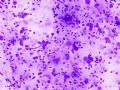 图5
图5 图6
图6 图7
图7 图8
图8
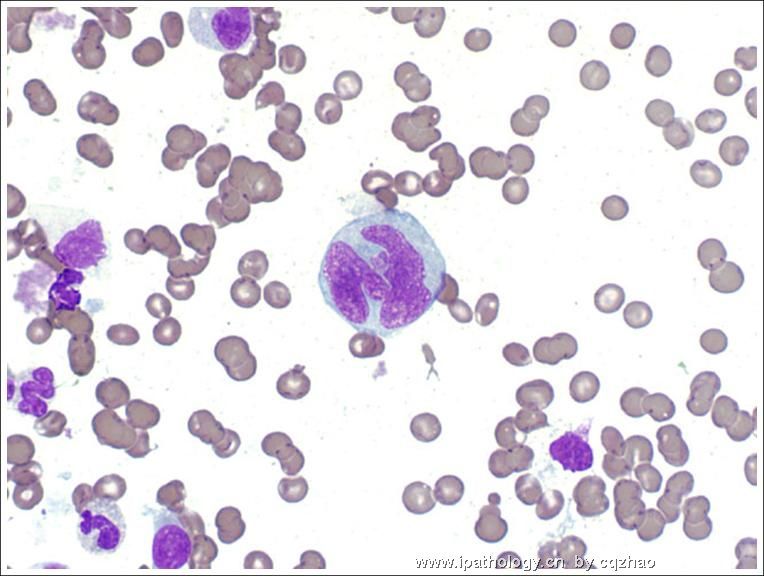
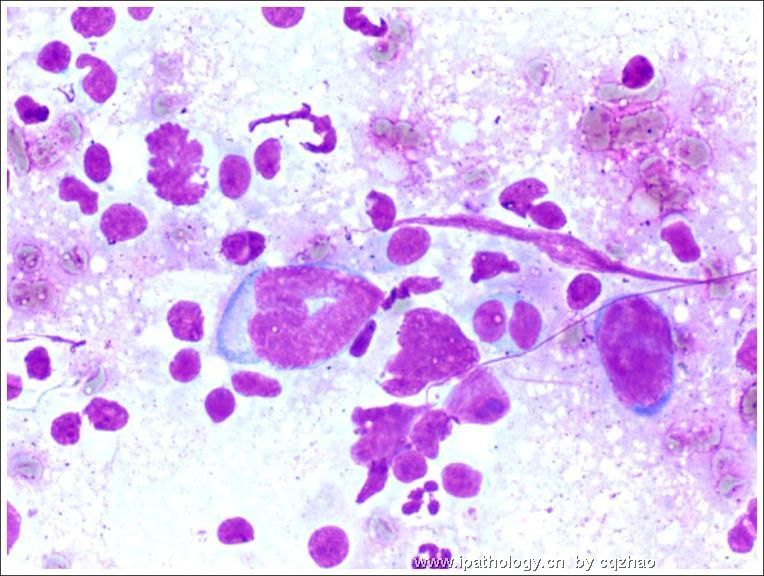
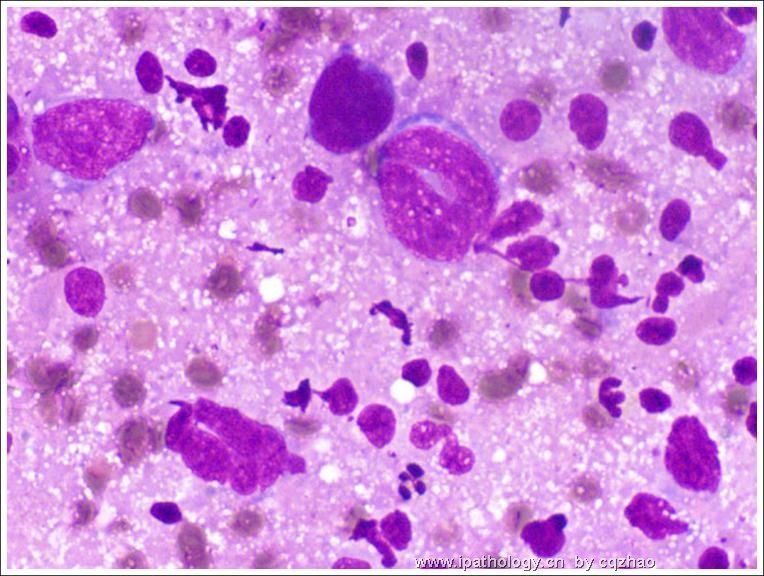
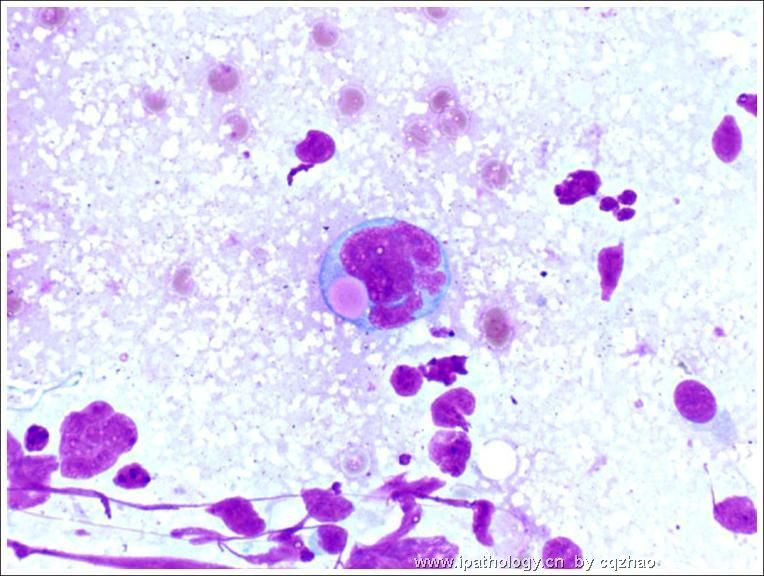
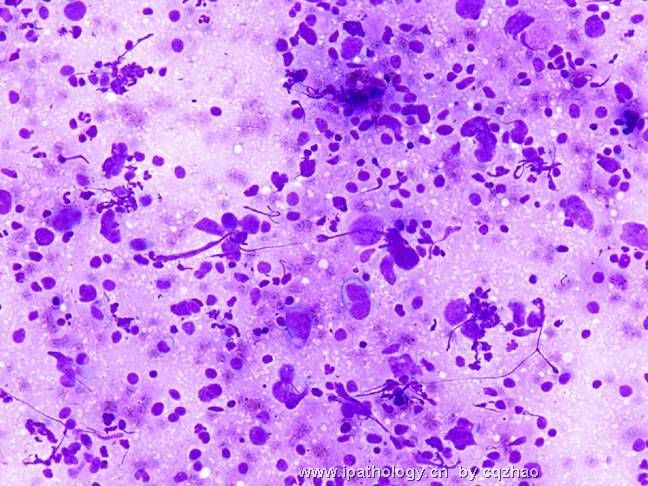
After the original dx of valvar lesion, an enlarged LN was found in pelvic area. FNA was performed.(外阴病变诊断后,发现盆部肿大淋巴结1枚,行FNA)
Fig 1-5 cytology of lymph node FNA. (图1-5为淋巴结FNA细胞学)
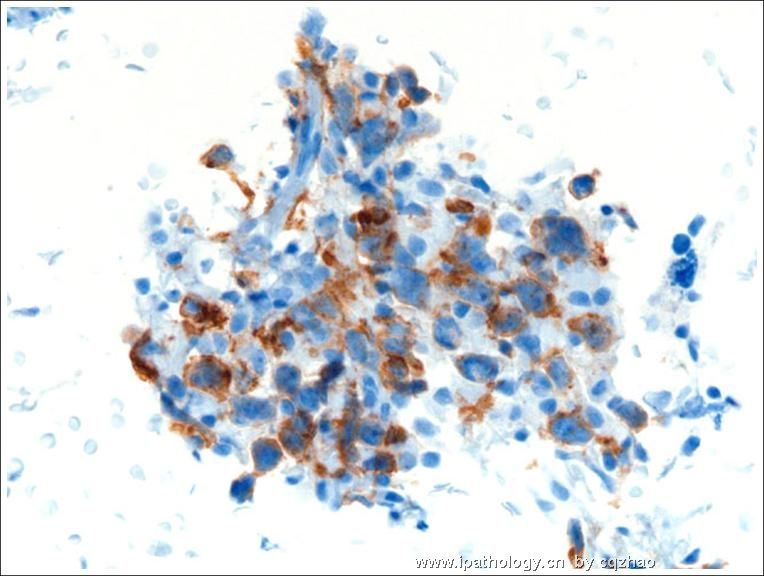
Fig 6: CD3
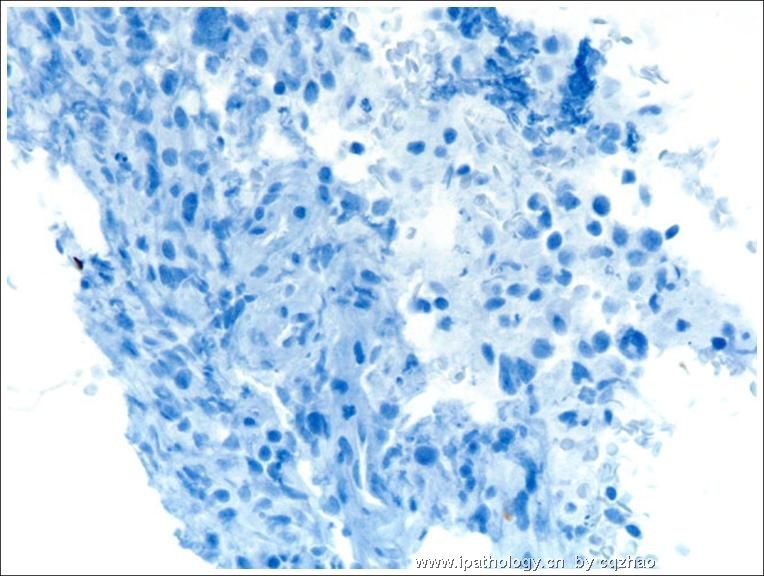
Fig 7: CD20
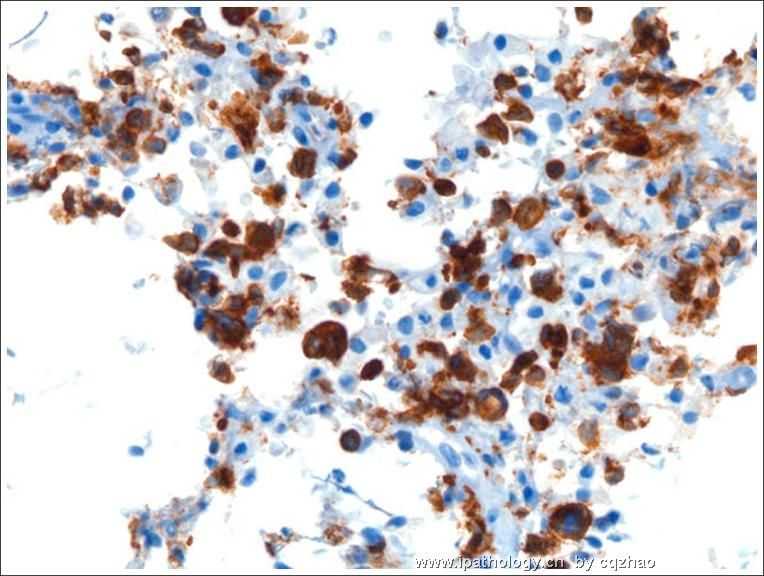
Fig 8: CD30
All other IHC results in cell block are the same as that in valvar lesion.
molecular analysis of ALK is negative. (细胞块其余IHC结果与外阴病变相同。分子学检测ALK阴性)
-
本帖最后由 于 2008-11-11 17:58:00 编辑
thank all of you for your discussion. After I got the first IHC results, I sign-out the case as hemologic/lymphocytic malignancy and sent the case to our hemotopathologist for further evaluation. The final dx is ATCL , ALK neg.
Thank Abin's excellent analysis. I especially appreciate the first reviewer WY1992. You are great you can consider T cell lymphoma immediately. In fact Lymphoma is my last consideration. Ha ha.
I will present more follow-up data soon.
abin译:谢谢大家参与讨论。第一批IHC结果,我签发了造血/淋巴系统恶性肿瘤,然后转给我们的血液病理医生进一步分型。
最后诊断:ATCL,ALK阴性。
谢谢abin,分析非常好。特别赞赏第一个发表意见的WY1992,能立即考虑到T细胞淋巴瘤。实际上淋巴瘤是我的最后考虑,哈哈。我将提供更多随访资料。
-
本帖最后由 于 2008-11-11 17:53:00 编辑
-
Peripheral T-cell Lymphoma With Follicular T-cell Markers.
To: Shiyan:
I am an gyn/breast pathologists and cytopathologist, very short of knowledge in hematopath. I am sure that you know much more than I know. I find a good paper PTCL. I can email you the full paper if you want to and told me your email.
Am J Surg Pathol. 2008 Sep 5. [Epub ahead of print]
Thank all of you who read the case and wrote your differential dx. I just came back from China last weekend and sorry for the delay.
IHC:
Vimentin Positive
Epithelial markers negaative: AE1/AE3, Cam 5.2, CK7, CK20
Melanoma markers negative: Melan-A, HMB-45, S-100
Muscle markers negative: SMA, Desmin,
LCA (CD45) See photo











