

















| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- 左胫骨近端肿块-上海市骨与关节肿瘤读片2013(2-4)-上海交大附属市六院提供
-
-上海交大附属市六院提供图1") 图1
图1 -
-上海交大附属市六院提供图2") 图2
图2 -
-上海交大附属市六院提供图3") 图3
图3 -
-上海交大附属市六院提供图4") 图4
图4 -
-上海交大附属市六院提供图5") 图5
图5 -
-上海交大附属市六院提供图6") 图6
图6 -
-上海交大附属市六院提供图7") 图7
图7 -
-上海交大附属市六院提供图8") 图8
图8 -
-上海交大附属市六院提供图9") 图9
图9 -
-上海交大附属市六院提供图10") 图10
图10 -
-上海交大附属市六院提供图11") 图11
图11 -
-上海交大附属市六院提供图12") 图12
图12 -
-上海交大附属市六院提供图13") 图13
图13
| 性别 | 女 | 年龄 | 22 | 临床诊断 | 骨巨细胞瘤? |
|---|---|---|---|---|---|
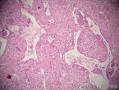
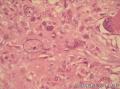
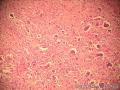
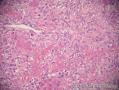
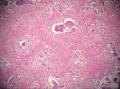
| 一般病史 | 患者无明显诱因下出现左膝肿胀、疼痛6月,活动受限。影像学:左胫骨近端偏心性椭圆形低密度病灶,中间有分隔,周围有硬化。考虑骨巨细胞瘤。入院行穿刺活检。 | ||||
| 标本名称 | 左胫骨近端肿块活检。 | ||||
| 大体所见 | 如低倍镜下所见大小碎组织。 | ||||
标签:胫骨 肿瘤
-
本帖最后由 海上明月 于 2013-10-09 15:51:09 编辑

- 王军臣
相关帖子
×参考诊断
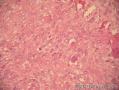
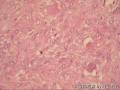
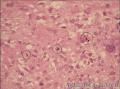
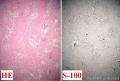
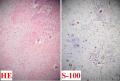
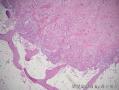
(左胫骨近端):富于巨细胞性髓内高分化骨肉瘤,肿瘤局部侵犯骨皮质。
Radiol Med. 2013 May 28. [Epub ahead of
print]
Giant cell-rich osteosarcoma in long
bones: clinical, radiological and pathological features.
Wang CS, Yin QH, Liao JS, Lou JH, Ding XY, Zhu YB.
Source
Department of Radiology, Ruijin
Hospital, Shanghai Jiao Tong University School of Medicine, No.197, Ruijin 2nd
Road, Shanghai, 200025, China.
Abstract
PURPOSE:
The purpose of
this study was to review the clinical presentation, imaging, pathology and
outcome of patients withgiant cell-rich osteosarcoma (GCRO) of
long bones.
MATERIALS AND METHODS:
Radiography (n=9),
magnetic resonance imaging (MRI) (n=6), computed tomography (CT) (n=3) and
clinical course of nine patients (five males and four females; mean age, 26
years) with pathologically confirmed GCRO were retrospectively reviewed.
Specific imaging findings, including size, eccentricity, ossification, lysis,
cystic change, expansile growth, periosteal reaction, cortical destruction,
soft tissue extension and joint involvement were documented.
RESULTS:
Presenting
symptoms were pain in six patients and pain and palpable mass in three. An
ill-defined margin surrounding a predominantly osteolytic lesion was detected
at the proximal tibia (n=7) or femur (n=2) on imaging studies. Seven cases
showed limited ossification. Three cases had tumours in the metaphysis and six
in the metaepiphysis. The average maximum tumour dimension was 4.7 cm×5.2
cm×7.8 cm. Microscopically, tumours were composed of atypical cells with scanty
osteoid formation and multinucleated giant cells. All patients
received chemotherapy, and surgery was performed in eight patients. Three
patients were dead and six were alive at the last follow-up.
CONCLUSIONS:
GCRO is a rarer
variant that has very close resemblance to giant cell tumour.
Patients usually present nonspecific symptoms of pain and palpable mass. It
usually shows an osteolytic lesion with locally spared new bone formation in
the metaphysis and/or metaepiphysis on imaging. Histologically, the atypical
tumour cells with osteoid formation and multinucleatedgiant cells are the
key factor in the diagnosis and differential diagnosis.
- 王军臣











