
 - WHO grade IV glioblastoma, granular cell variant图1")
 - WHO grade IV glioblastoma, granular cell variant图2")
 - WHO grade IV glioblastoma, granular cell variant图3")
 - WHO grade IV glioblastoma, granular cell variant图4")
 - WHO grade IV glioblastoma, granular cell variant图5")
 - WHO grade IV glioblastoma, granular cell variant图6")
 - WHO grade IV glioblastoma, granular cell variant图7")
 - WHO grade IV glioblastoma, granular cell variant图8")
 - WHO grade IV glioblastoma, granular cell variant图9")
 - WHO grade IV glioblastoma, granular cell variant图10")
 - WHO grade IV glioblastoma, granular cell variant图11")
 - WHO grade IV glioblastoma, granular cell variant图12")
 - WHO grade IV glioblastoma, granular cell variant图13")




| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- NP (4) - WHO grade IV glioblastoma, granular cell variant
-
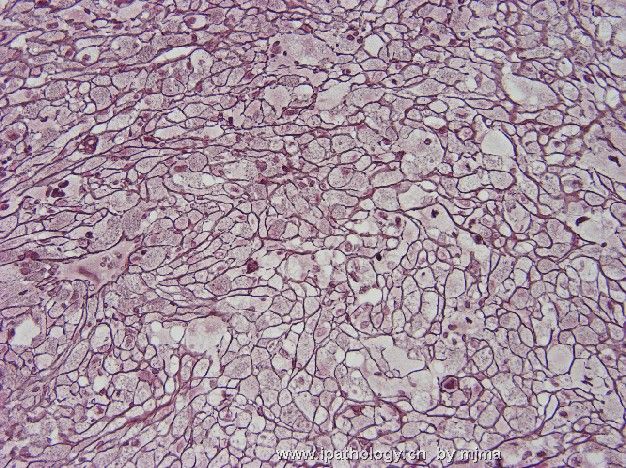
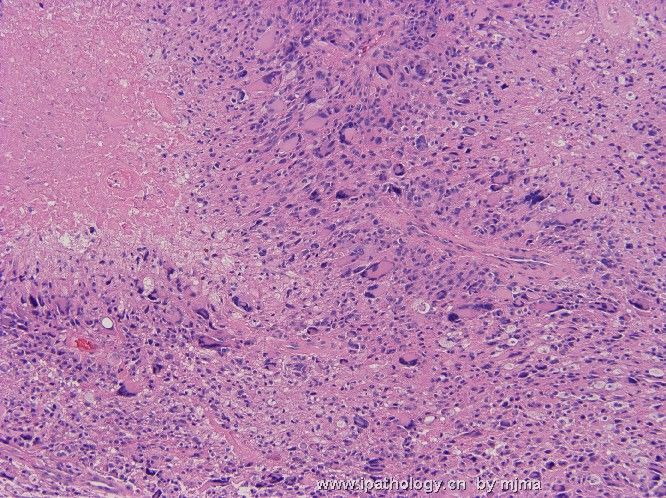
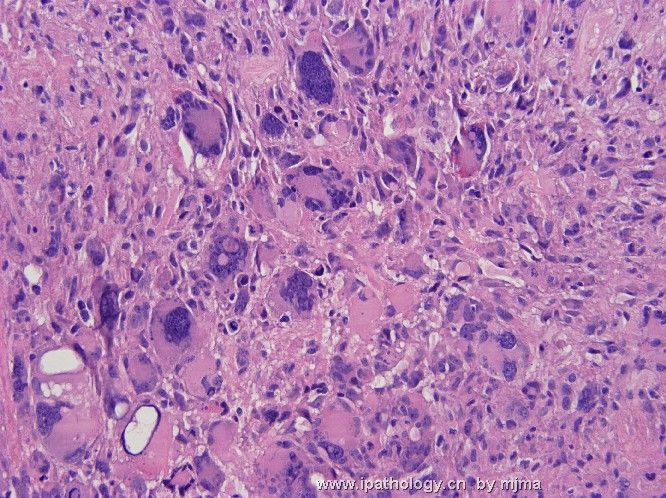
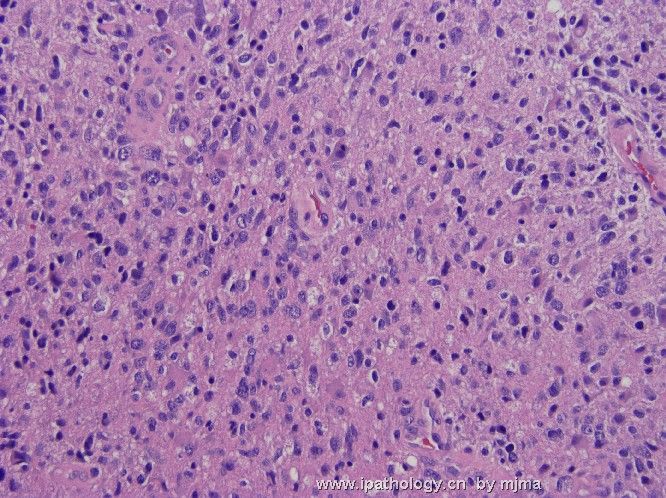
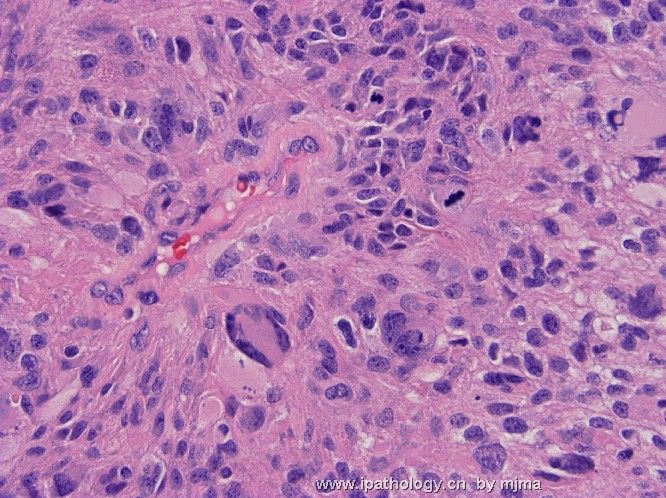
This is a resected supratentorial intra-axial focally enhancing brain tumor from a 50-year-old woman. Figures 1~5 are taken from the central portion of the resected tumor. Figures 6~12 are taken from the peripheral portion of the resected tumor. Figure 13 is taken from the interface between tumor and surrounding brain parenchyma. What is/are your diagnosis or your differential diagnoses? What stain(s) would help you?
 - WHO grade IV glioblastoma, granular cell variant图1") 图1
图1 - WHO grade IV glioblastoma, granular cell variant图2") 图2
图2 - WHO grade IV glioblastoma, granular cell variant图3") 图3
图3 - WHO grade IV glioblastoma, granular cell variant图4") 图4
图4 - WHO grade IV glioblastoma, granular cell variant图5") 图5
图5 - WHO grade IV glioblastoma, granular cell variant图6") 图6
图6 - WHO grade IV glioblastoma, granular cell variant图7") 图7
图7 - WHO grade IV glioblastoma, granular cell variant图8") 图8
图8 - WHO grade IV glioblastoma, granular cell variant图9") 图9
图9 - WHO grade IV glioblastoma, granular cell variant图10") 图10
图10 - WHO grade IV glioblastoma, granular cell variant图11") 图11
图11 - WHO grade IV glioblastoma, granular cell variant图12") 图12
图12 - WHO grade IV glioblastoma, granular cell variant图13") 图13
图13
标签:
-
本帖最后由 于 2006-11-08 11:16:00 编辑

聞道有先後,術業有專攻
×参考诊断
| 以下是引用xiaohl 在2006-10-30 15:41:00的发言: I want to know the exact location of this tumor,Thanks a lot. |
聞道有先後,術業有專攻
-
The anatomic location of this tumor is very important for a accurate diagnosis. If this leision localized in the surfuce of cerebrum, PXA with anaplastic feature or a histocytic tumor is to be considered, but the intra-axial location, the relatively old age of the patient and the untypical histomorphology features don't support this diagnosis.
If the leision localized intrasellarly and/or suprasellayly, I would prefer the diagnosis of granular cell tumor of the neurohypophysis.
If the tumor arise from the parenchyma of the cerebrum, the diagnosis of giant cell glioblastoma must be considered. So, I think the exact location of this tumor is the utmost important for its correct diagnosis, then, some kinds of antibodies,such as GFAP,Ki67,NSE,SYN,S-100,CD68,α1-AT,and so on,will do some help for our diagnosis.
| 以下是引用xiaohl 在2006-10-31 23:46:00的发言:The anatomic location of this tumor is very important for a accurate diagnosis. If this leision localized in the surfuce of cerebrum, PXA with anaplastic feature or a histocytic tumor is to be considered, but the intra-axial location, the relatively old age of the patient and the untypical histomorphology features don't support this diagnosis. If the leision localized intrasellarly and/or suprasellayly, I would prefer the diagnosis of granular cell tumor of the neurohypophysis. If the tumor arise from the parenchyma of the cerebrum, the diagnosis of giant cell glioblastoma must be considered. So, I think the exact location of this tumor is the utmost important for its correct diagnosis, then, some kinds of antibodies,such as GFAP,Ki67,NSE,SYN,S-100,CD68,α1-AT,and so on,will do some help for our diagnosis. |
聞道有先後,術業有專攻
-
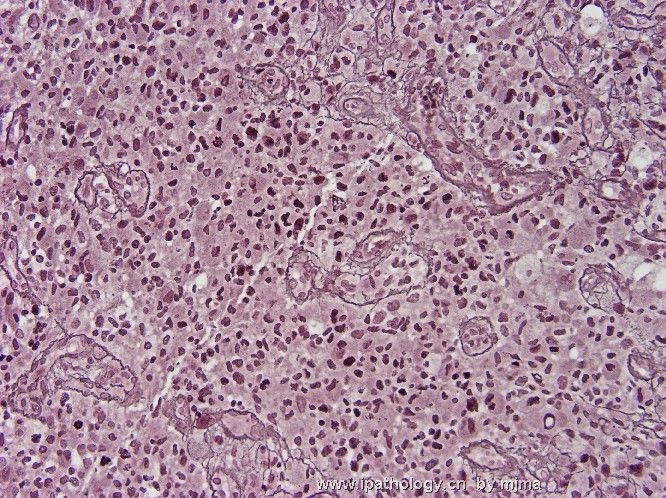
Figures 1~2 are taken from reticulin silver stain, with 1 from the center and 2 from the periphery of the tumor.
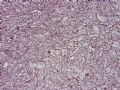 图1
图1 图2
图2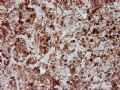 图3
图3 图4
图4 图5
图5 图6
图6 图7
图7
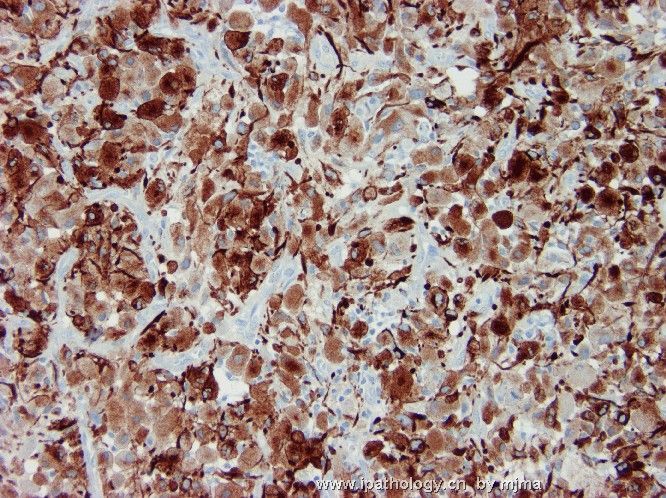
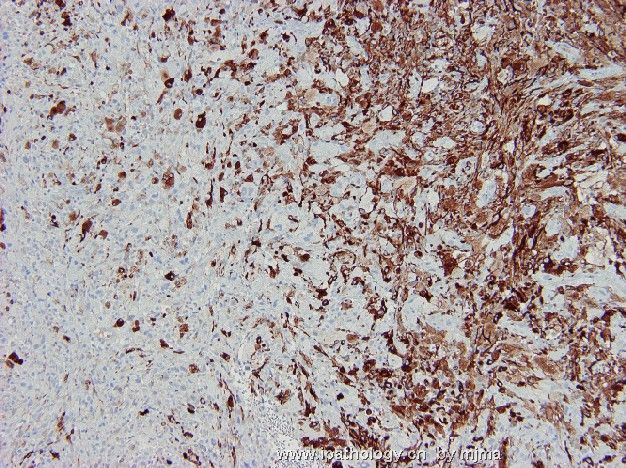
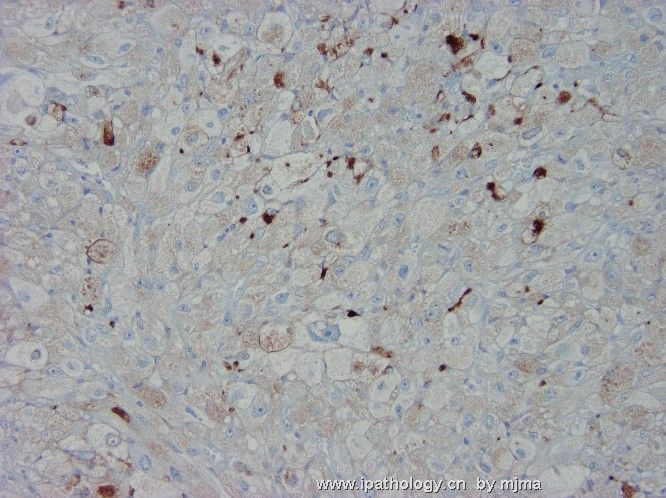
Figures 3~5 are taken from GFAP immunohistochemical stain, with 3 from the periphery, 4 from the interface, and 5 from the center of the tumor.
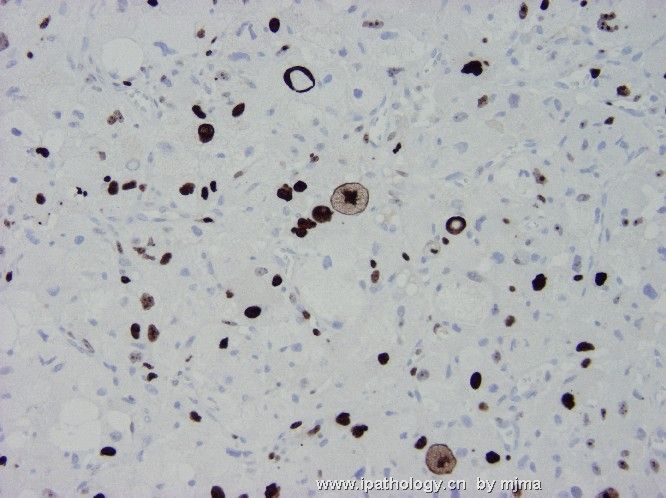
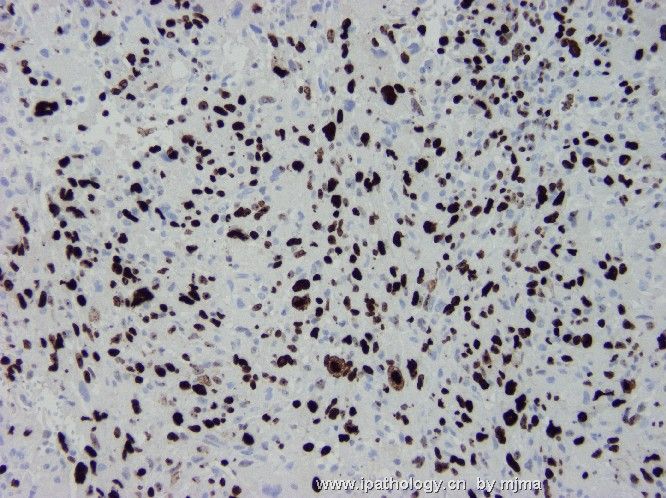
Figures 6~7 are taken from MIB-1 immunohistochemical stain, with 6 from the center and 7 from the periphery of the tumor.
聞道有先後,術業有專攻
-
Thanks a lot for your presentation. The staining of reticulin fiber , GFAP and MIB-1
are very beautiful. There exist obvious differences of these stainings between the center and the periphery of the tumor.Histologically,we can also noticed 2 distinct areas of the tumor. In the center, there are a lot of xanthomaous-like cells and some spindle cells arranged in faciculation,but in the periphery of the tumor, we can see many anaplastic astrocytes and the cell density increases obviously. According to these histologic features and helpful staining, what is your diagnosis?
-
This is a rare case of WHO grade IV, granular cell variant of glioblastoma. The granular cells in this case are very prominent and occupy the central bulk of the resected tumor. They faithfully illustrate this variant of almost always high grade (WHO grade III~IV) astrocytoma. The granular cytoplasm is moderately positive on PAS stain (not shown), and there is very distinctive pericellular reticulin fibrils on silver stain. Intratumoral inflammatory infiltrates have been listed as a characteristic feature, but I have not seen enough of this variant to say this is true. There are many characteristic neoplastic astrocytes in the periphery of this resected tumor with features consistent with glioblastoma. This is usually the case, and astrocytomas consisting purely of granular cells are extremely rare. there is no quantitative criterion (?percentage of cells to be granular cells) for assigning an astrocytoma this particular variant. In general, I follow the 50% rule.
 图1
图1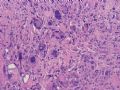 图2
图2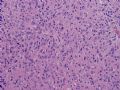 图3
图3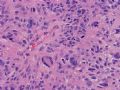 图4
图4
Differential diagnoses of this rare tumor include pleomorphic xanthoastrocytoma (PXA) with anaplastic features, giant cell variant of glioblastoma, benign granular cell tumor of dura/leptomeninges or of pituitary gland, macrophages or histiocytes (infarct, demyelinating lesion, Erdheim-Chester disease), and metastases (alveolar soft part sarcoma, renal cell carcinoma, adrenal cortical carcinoma). Perhaps the most critical key to rule these out is, as xiaohl pointed out earlier, is the anatomic location of the lesion. With resection specimens, these are not that difficult to distinguish. If, unfortunately, you do not have this important information and only have a small biopsy to examine, it can be very difficult to reach the correct diagnosis.
At first glance, the granular cells may appear histiocytic, but their malignant nature is evidenced by atypical nuclear features (size and shape variations with scattered very large and hyperchromatic nuclei, irregular nuclear shape, and occasional mitoses). Granular cell tumors (considered a special type of schwannomas) of dura/meninges are extremely rare. Granular cell tumor of pituitary gland and hypothalamus are also rare. These two tumors are benign and cells do not have malignant features. Like granular cell astrocytoma, PXA and giant cell glioblastoma show pericellular reticulin fibrils and, usually, prominent perivascular inflammation. The giant cells in these two tumors, however, are usually much larger in size with a much greater cellular size variation. PXA almost always occurs at a superficial cerebral cortical location. Giant cell glioblastomas usually contain very small neoplastic cells between giant cells. All these are helpful points.
Nine month after gross tumor resection and post-surgical irradiation of tumor bed, the tumor was found to have recurred by MRI and a second resection was undertaken. The resected tissue shows a mitotically active and focally necrotic glioblastoma of the usual type (see Figures 1~4 below).
聞道有先後,術業有專攻
-
zhongshihua 离线

- 帖子:1608
- 粉蓝豆:0
- 经验:1651
- 注册时间:2006-09-11
- 加关注 | 发消息
-
简单翻译一下:
这是一例少见的胶质母细胞-颗粒细胞变型(WHO4级).本例的颗粒状细胞非常明显,主要位于肿瘤的中央部位.这表明这种变型往往是高级别的星形细胞瘤.颗粒状细胞胞质PAS阳性,银染显示瘤细胞周围丰富的网状纤维.瘤内炎细胞浸润被认为是该变型的特征之一,但是由于所见的病例较少,不便下定论.本例在肿瘤外周可见到许多肿瘤性星形细胞,具备胶质母细胞瘤的特征.事实情况也确实如此,单纯由颗粒状细胞构成的星形细胞瘤是极其罕见的.至于颗粒状细胞应达到多少比例才能归为该亚型,目前尚无量化的标准,本人认为50%较为合适.
鉴别诊断包括伴间变特征的PXA,巨细胞性胶质母细胞瘤,硬/软脑膜或垂体发生的良性颗粒细胞瘤,巨噬细胞或组织细胞病变(梗死,脱髓鞘病变或Erdheim-Chester 病)以及转移性肿瘤(腺泡状软组织肿瘤,肾细胞癌,肾上腺皮质癌).最为重要的鉴别点应是病变的部位所在.在切除的标本中,上述病变并不难以鉴别,但是,如果缺乏关于肿瘤部位部位的准确信息,而且标本很小的时候,诊断是极其困难的.
初看起来,这些颗粒状细胞容易被当成组织细胞,但其核的间变特征(如大小形态不一,大而深染的核,核形不规则,核分裂像)表明其恶性本质.硬/软脑膜的颗粒细胞瘤很少见,被认为是雪旺氏细胞瘤的特殊类型,垂体的颗粒细胞瘤也非常少见,这两种肿瘤是良性的,细胞没有间变特征.PXA和巨细胞性胶质母细胞瘤具有与颗粒细胞型星形细胞瘤相似的一些特点,如围细胞的网纤以及血管周围的炎细胞浸润等,但这两种肿瘤中的巨细胞往往体积更大,而且大小很不一致.PXA一般发生于大脑皮层浅表部位,而巨细胞性胶质母细胞瘤在巨细胞之间往往存在小的肿瘤细胞.上述各点都有助于我们去判断.
肿瘤切除并术后局部放疗后9个月,MRI证实肿瘤复发,遂进行了第二次手术切除,术后病理为常见的胶质母细胞瘤形态,细胞核分裂活跃,局灶性坏死.
鉴别诊断包括伴间变特征的PXA,巨细胞性胶质母细胞瘤,硬/软脑膜或垂体发生的良性颗粒细胞瘤,巨噬细胞或组织细胞病变(梗死,脱髓鞘病变或Erdheim-Chester 病)以及转移性肿瘤(腺泡状软组织肿瘤,肾细胞癌,肾上腺皮质癌).最为重要的鉴别点应是病变的部位所在.在切除的标本中,上述病变并不难以鉴别,但是,如果缺乏关于肿瘤部位部位的准确信息,而且标本很小的时候,诊断是极其困难的.
初看起来,这些颗粒状细胞容易被当成组织细胞,但其核的间变特征(如大小形态不一,大而深染的核,核形不规则,核分裂像)表明其恶性本质.硬/软脑膜的颗粒细胞瘤很少见,被认为是雪旺氏细胞瘤的特殊类型,垂体的颗粒细胞瘤也非常少见,这两种肿瘤是良性的,细胞没有间变特征.PXA和巨细胞性胶质母细胞瘤具有与颗粒细胞型星形细胞瘤相似的一些特点,如围细胞的网纤以及血管周围的炎细胞浸润等,但这两种肿瘤中的巨细胞往往体积更大,而且大小很不一致.PXA一般发生于大脑皮层浅表部位,而巨细胞性胶质母细胞瘤在巨细胞之间往往存在小的肿瘤细胞.上述各点都有助于我们去判断.
肿瘤切除并术后局部放疗后9个月,MRI证实肿瘤复发,遂进行了第二次手术切除,术后病理为常见的胶质母细胞瘤形态,细胞核分裂活跃,局灶性坏死.











