


















| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
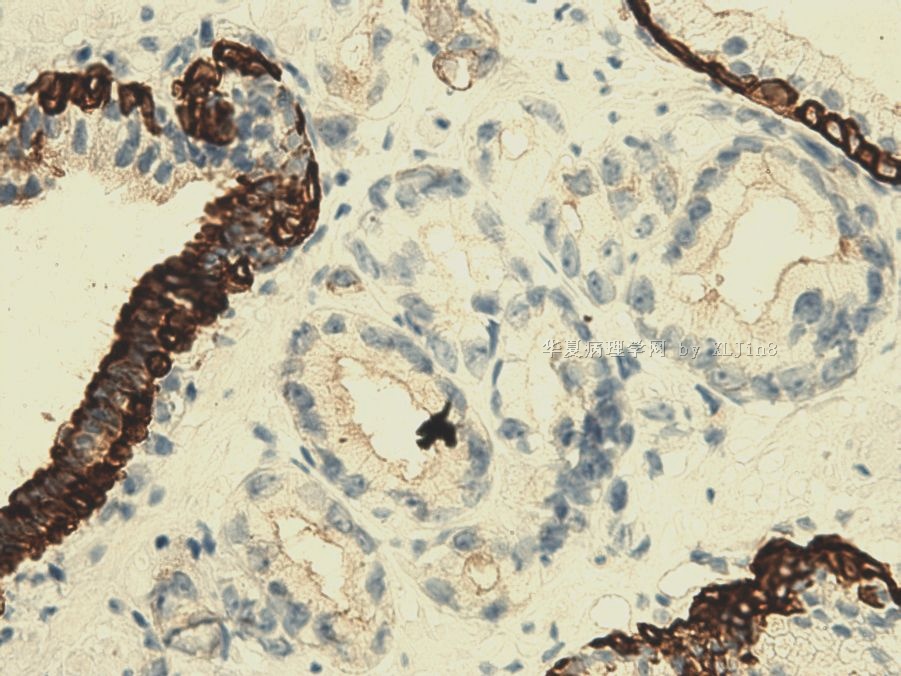
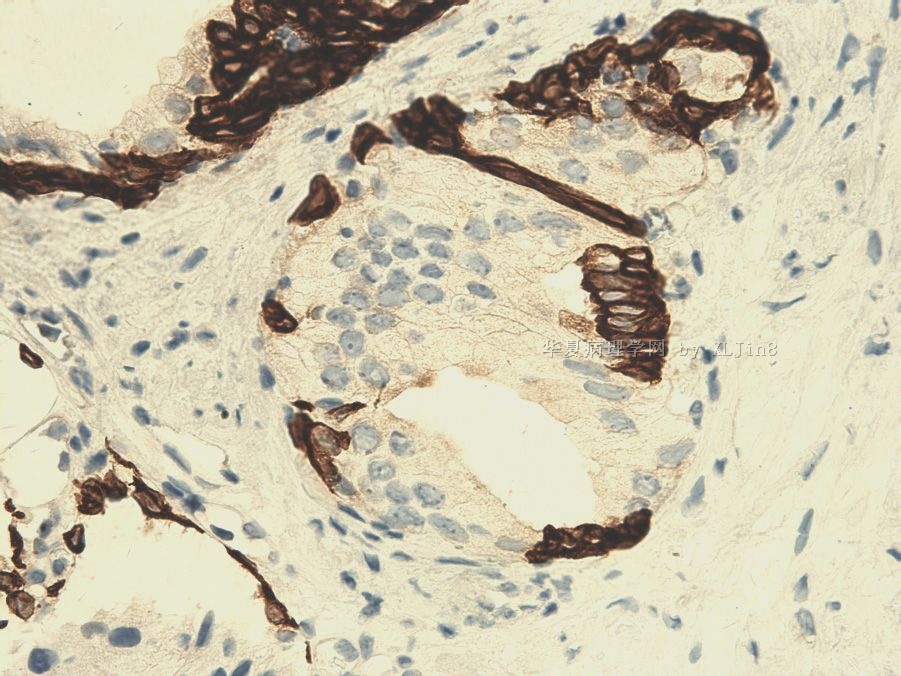
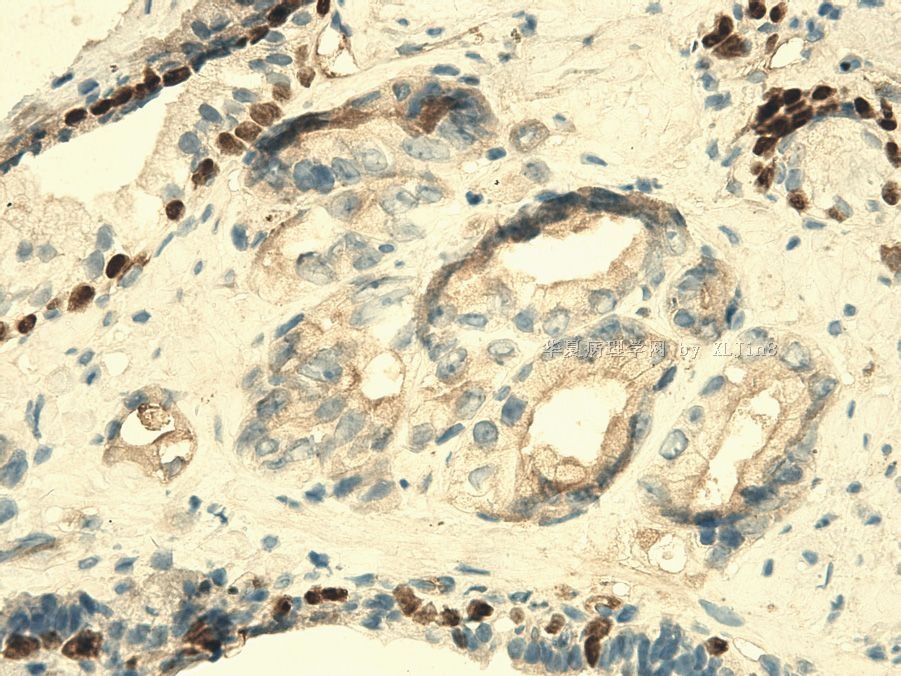
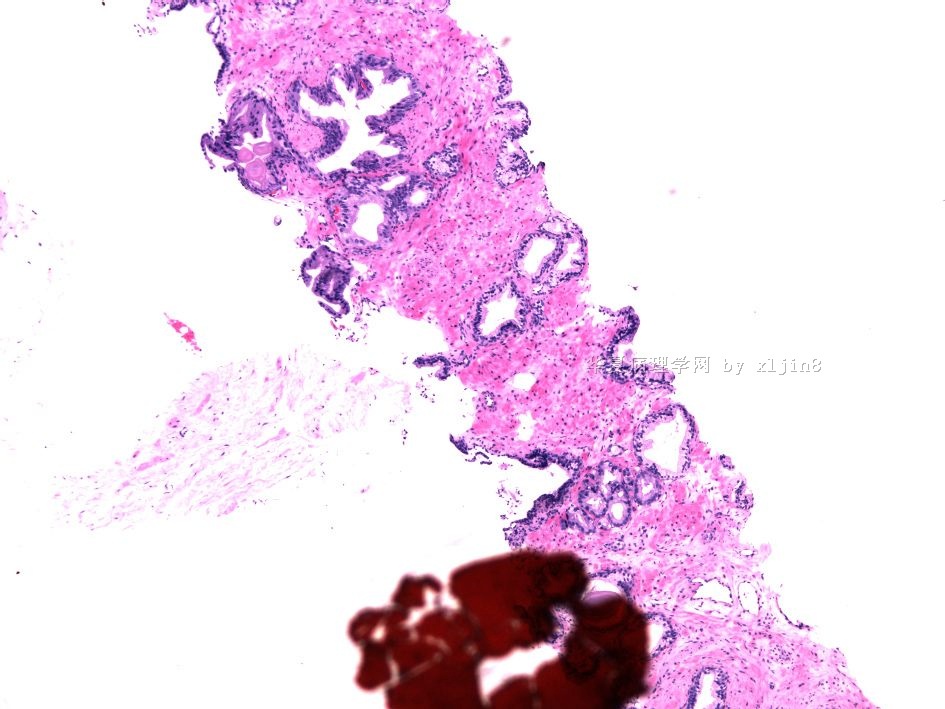
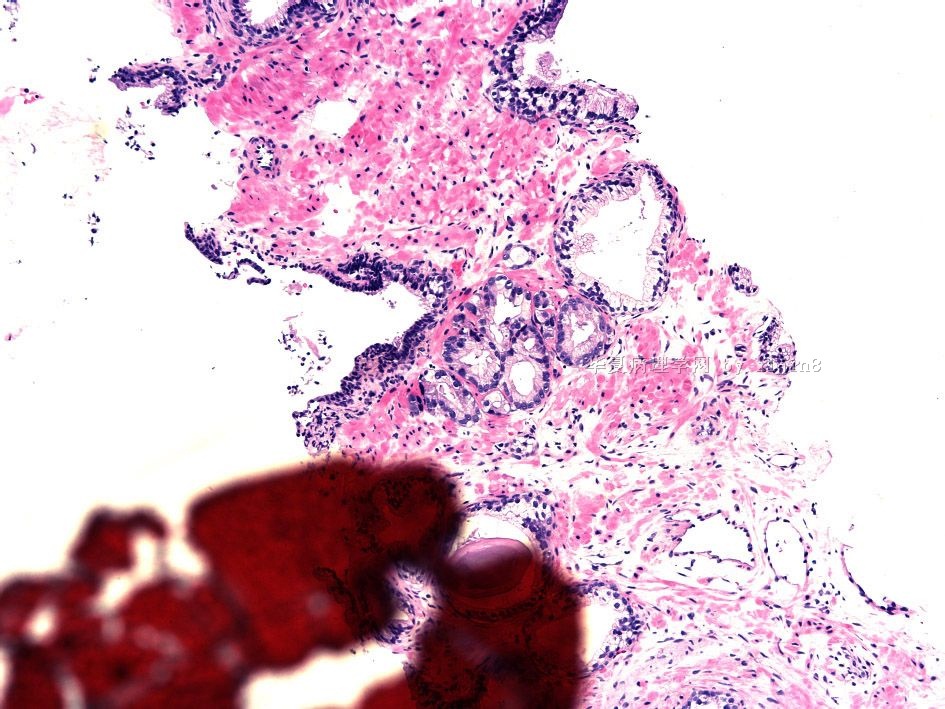
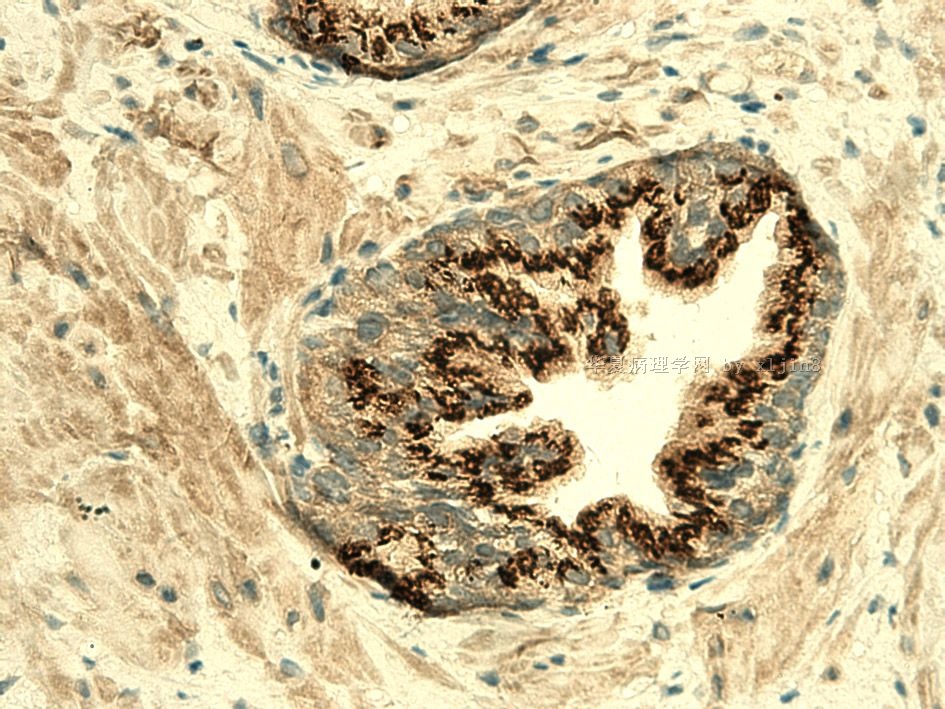
- 男/52岁 前列腺穿刺 诊断?
-
本帖最后由 于 2010-10-13 15:41:00 编辑
对于活检组织中有少量异常腺体时要给予一个非常肯定的诊断有时是非常困难的, 这不仅在前列腺活检、同样包括乳腺、GI、呼吸道等器官的活检。
解决疑难的方法:
1)密切联系临床, 与临床医生沟通;
2)详细分析对病理诊断有帮助的实验室数据和影像学资料等;
3)仔细的镜下观察,与其他病理医生讨论;
4)完善病理诊断必须的临床资料;
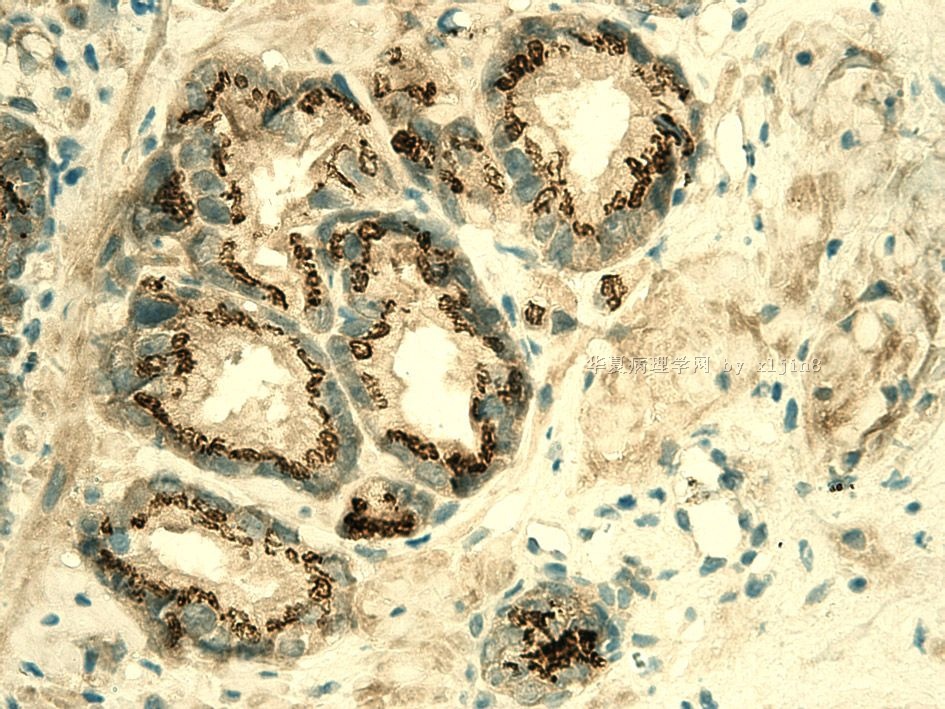
5)合理选择IHC标记;
6)如不能明确诊断,与病家沟通,建议随访、重复活检、专家会诊。
病理医生要区分活检组织中的少量可疑病变可能存在的二种基本情况:
1)患有是进展期癌,只不过活检组织中存在微量的癌(冰山一角);
2)患者是局灶性癌前期病变(高级别PIN/上皮内瘤变)或微量早癌。
病理医师要了解自己的诊断对临床处理产生的影响、了解对病人疾病预后与生活质量产生的影响。不要拒绝请专家会诊, “Second Lock” 有助于病人、有助于初诊医生的业务提高,何乐而不为? 病理诊断是艺术!有时退一步(不勉强诊断和过诊断)海阔天空。

- xljin8
- 文章:4828
- 积分:24255
- 经验:4910
- 注册:2009-8-29 13:59
|
| |||||||||
- 王军臣
-
本帖最后由 于 2010-10-08 08:15:00 编辑
Epstein JI & Netto GJ.
Biopsy interpretation of the prostate, 4th edtion,2008,p74.
表6-2 前列腺癌与PIN的鉴别诊断。
|
支持诊断癌 (Favoring Cancer) |
反对诊断癌 (Against Cancer) |
|
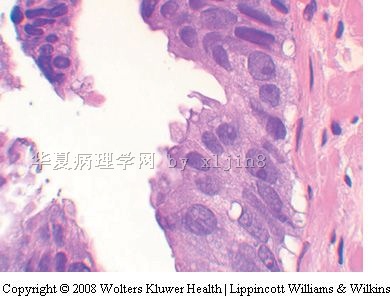
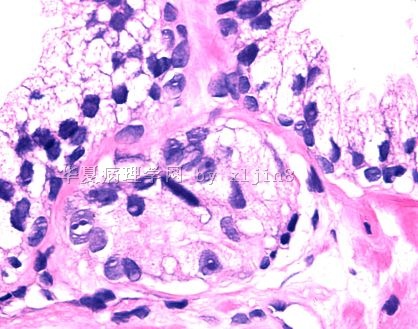
结构(Architectural) 浸润性构型 小腺体 腺体拥挤 细胞核(Nuclear) 核仁明显 核增大 核分裂 凋亡小体 细胞质(Cytoplasmic) 无定形细胞质 腔缘胞质整齐 管腔内容物 蓝色黏液性分泌物 粉红色无定形分泌物 结晶体 |
结构(Architectural) 小叶状结构 大腺体 分支腺体 细胞核(Nuclear) 核仁明显但是临近有PIN 核改变与邻近良性腺体相似 核不典型伴有炎症反应
细胞质(Cytoplasmic) 淡然-透明胞质 腔缘波纹状或乳头状突起 管腔内容物
淀粉样小体 |
- xljin8











