














 染色结果太好了,谢谢金老师!
染色结果太好了,谢谢金老师!
 .......。您有什么高见,请赐教,谢谢!
.......。您有什么高见,请赐教,谢谢!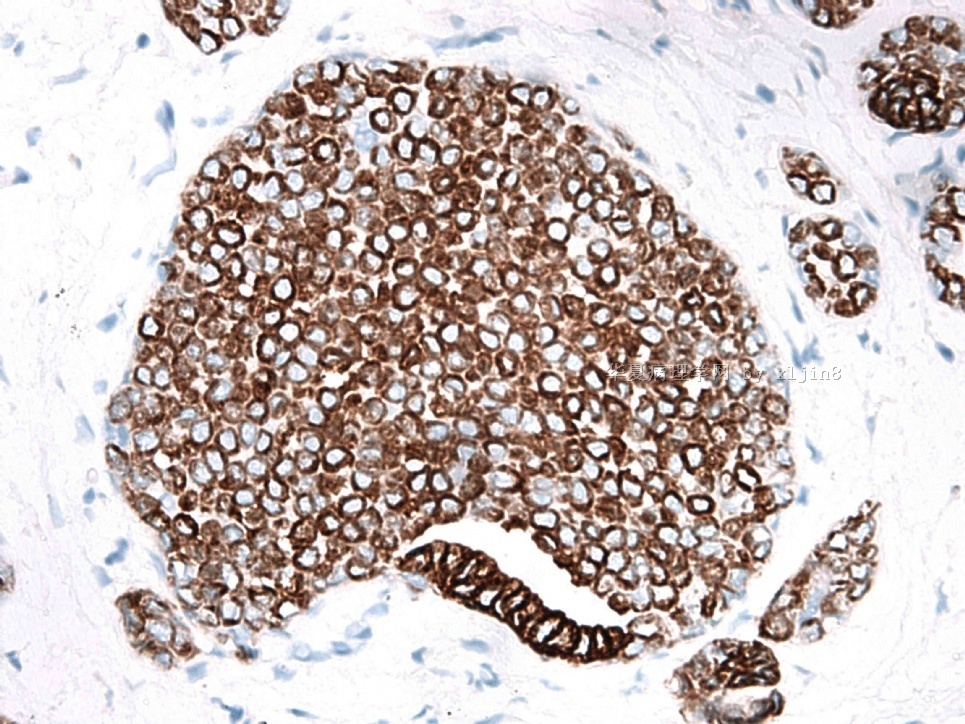



| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- B2855女性/49岁,右乳房肿块,2.8cm
综合cqzhao老师的回复意见如下:
1。根据HE及免疫组化染色,加之个人经验,赵老师判读为:浸润性导管癌伴小管癌特征(此处顺及各位老师讨论的到底是小管癌还是浸导?小管癌是浸导的一个亚型);浸润性小叶癌;原位小叶癌(LCIS)。
2。为了简单化,报告会这样发:混有导管癌和小叶癌的浸润性癌(详见后附建议);同时具有LCIS成分。
3。文献中对小管小叶癌的描述:主要是导管癌,伴有局灶性管状及小叶特征。现在这个名称已经不用
4。至于印戒细胞的来源,赵老师认为是小叶来源

- 赚点散碎银子养家,乐呵呵的穿衣吃饭
Coplicated case. Abin and Dr. Jin had good discussion. Learning.
Based on H&E and stains, the my interpretation:
Invasive ductal carcinoma with tubual feature.
Invasive lobular carcinoma.
LCIS
Make it simple, just call invasive mixed ductal and lobular ca (see comment); LCIS.
-
本帖最后由 于 2010-08-30 20:51:00 编辑
谢谢金老师提供的好病例,以及挑战性的提问,再次学习,并对24楼作少许更正和补充:
肿瘤有三种成分:原位癌,浸润的单细胞(包括印戒细胞),浸润的小管成分
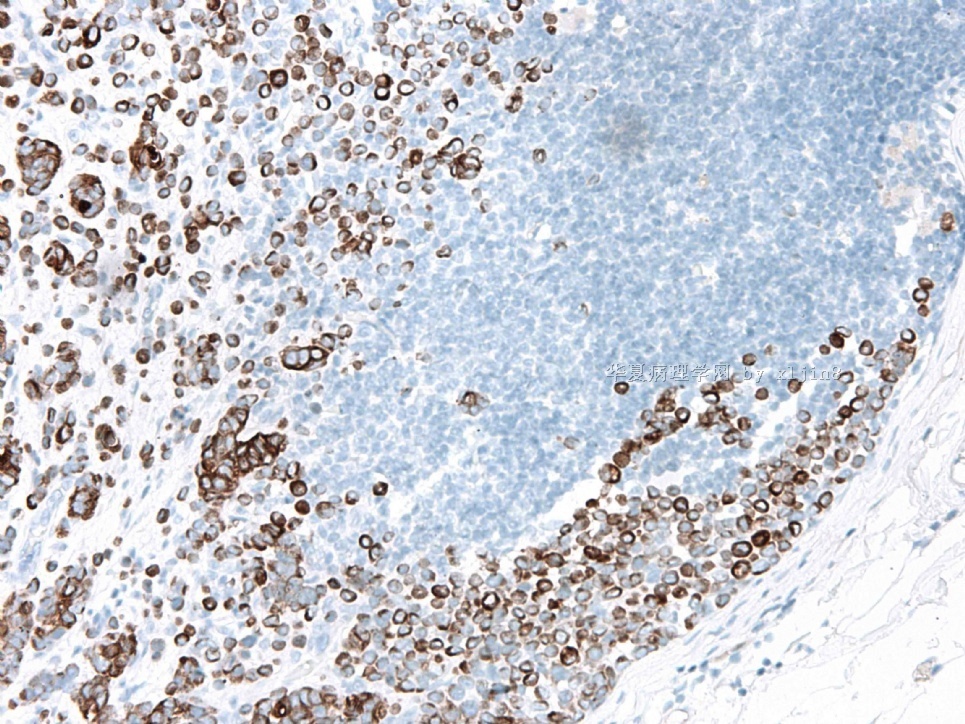
1、根据HE和免疫组化,原位癌和浸润的单细胞(包括印戒细胞)都是小叶癌性质。
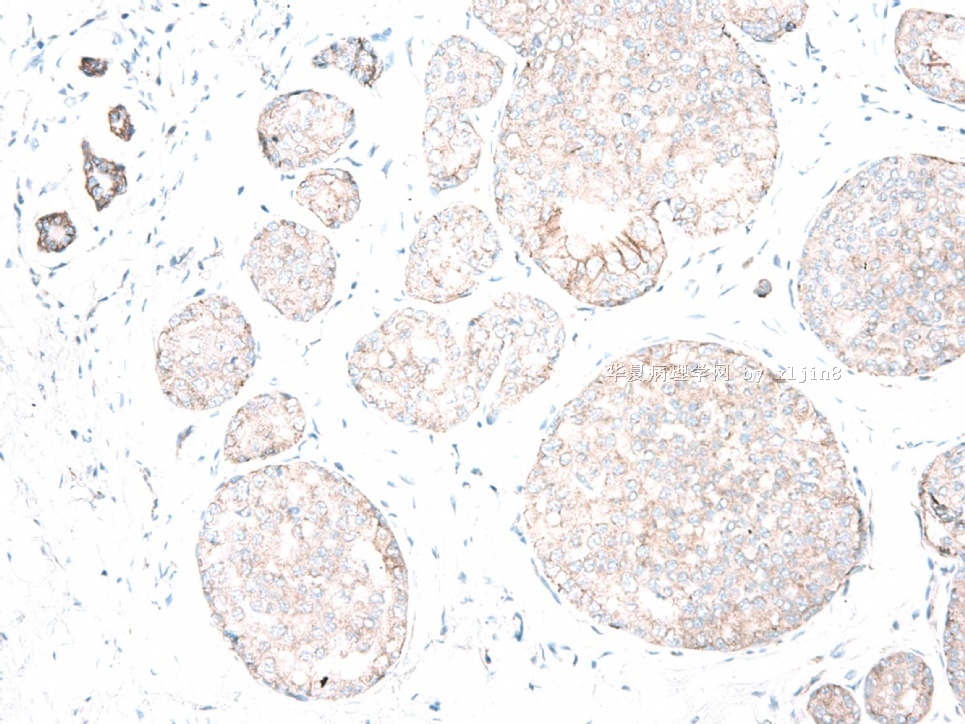
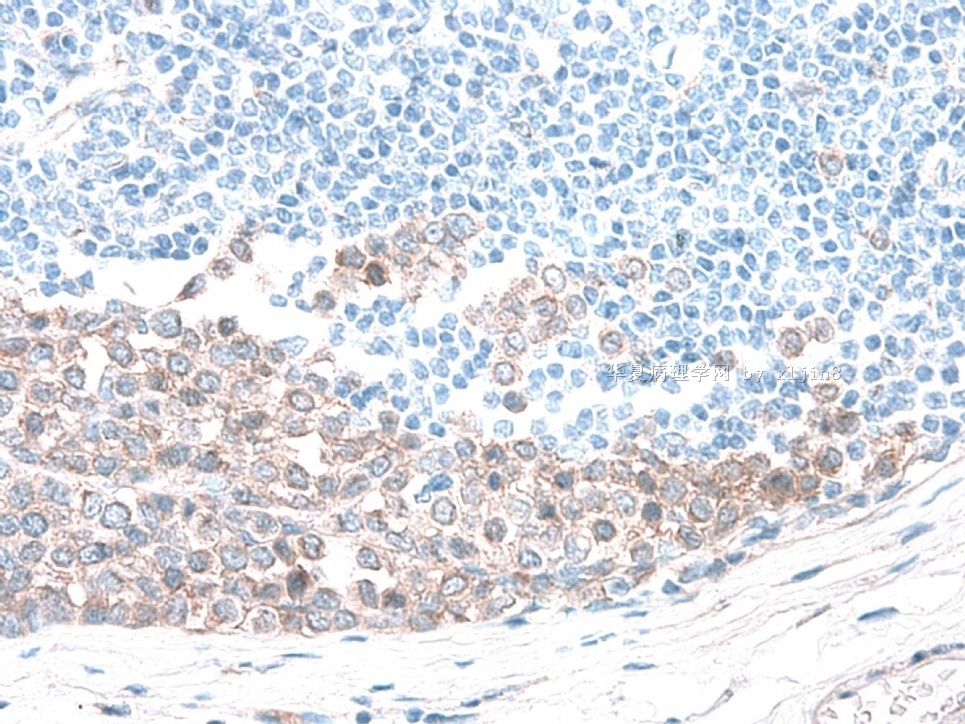
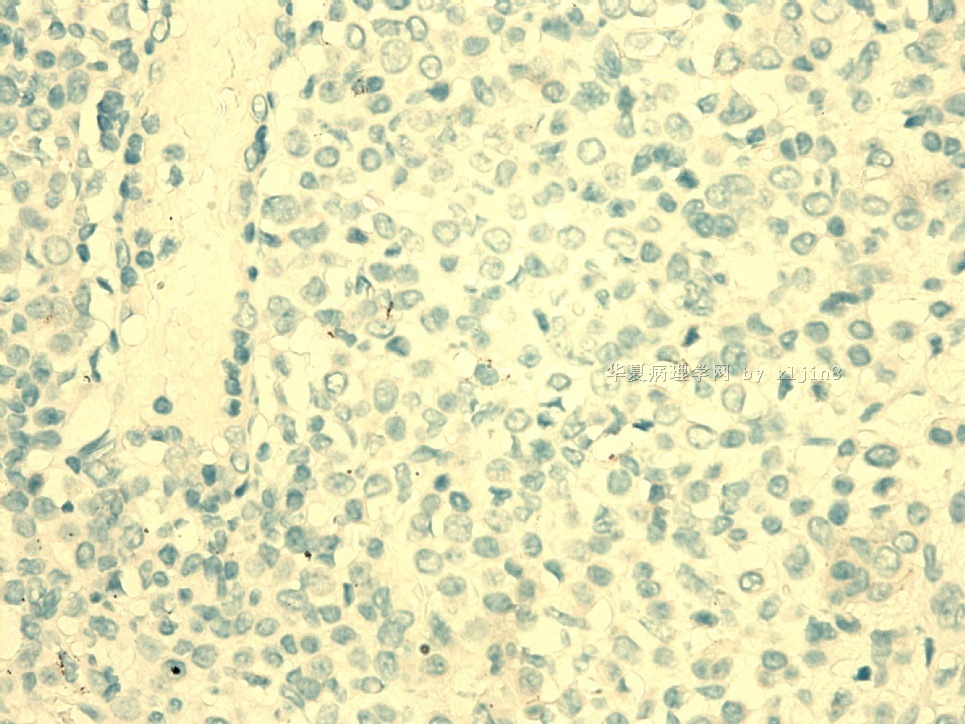
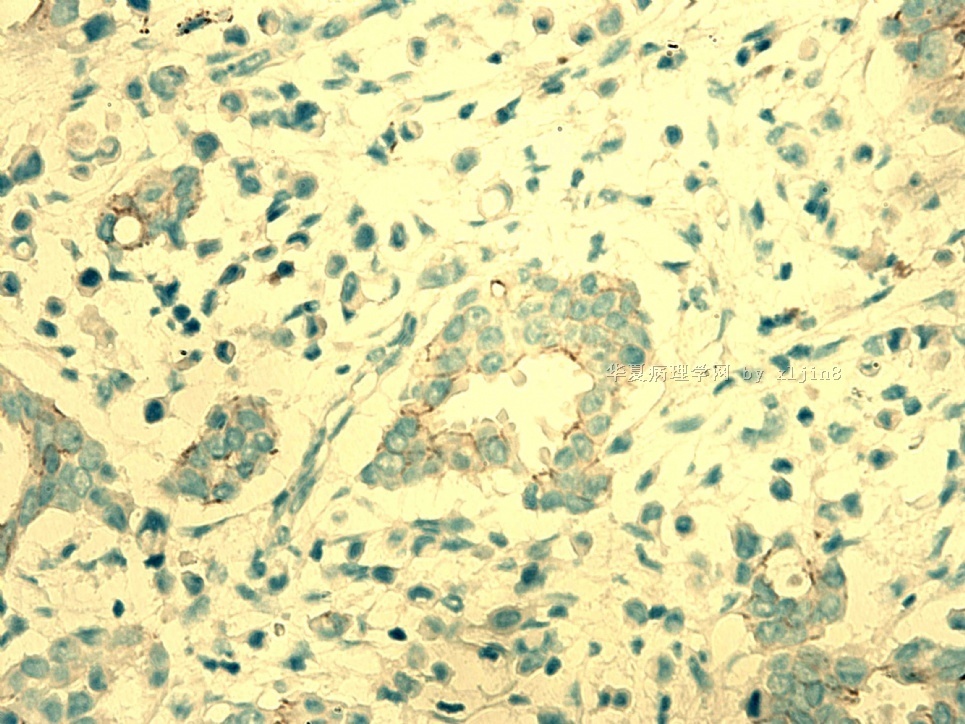
2、浸润的小管成分,免疫组化:
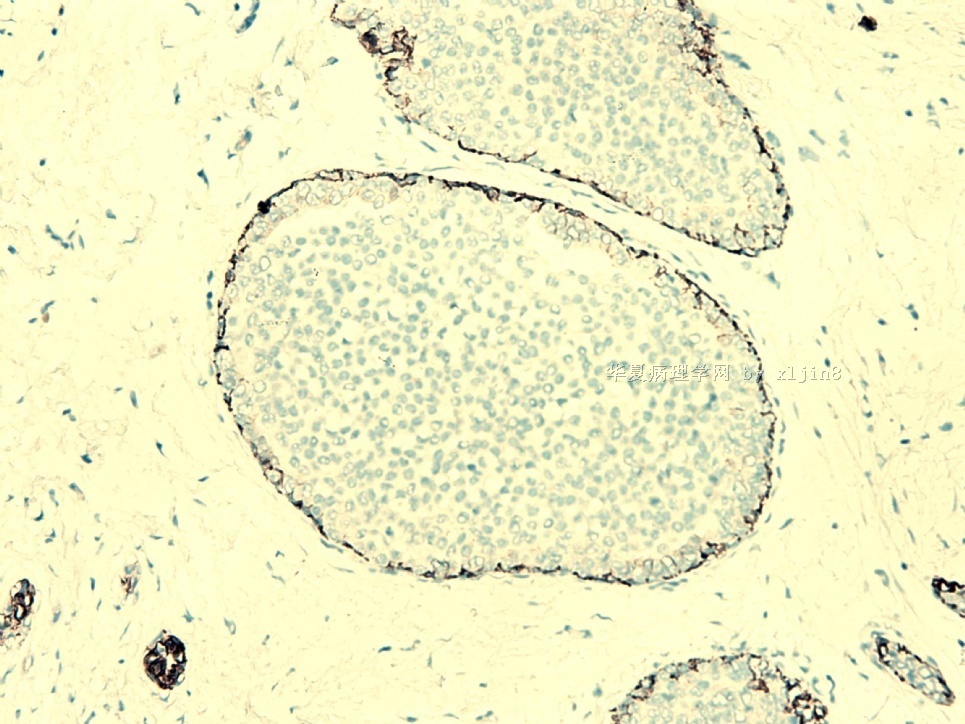
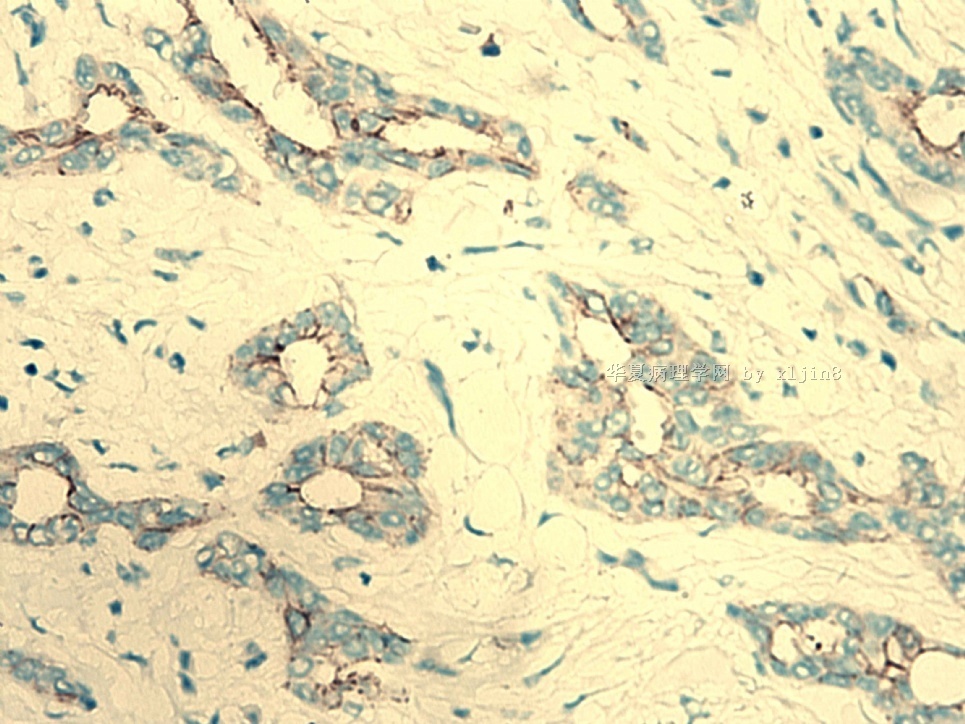
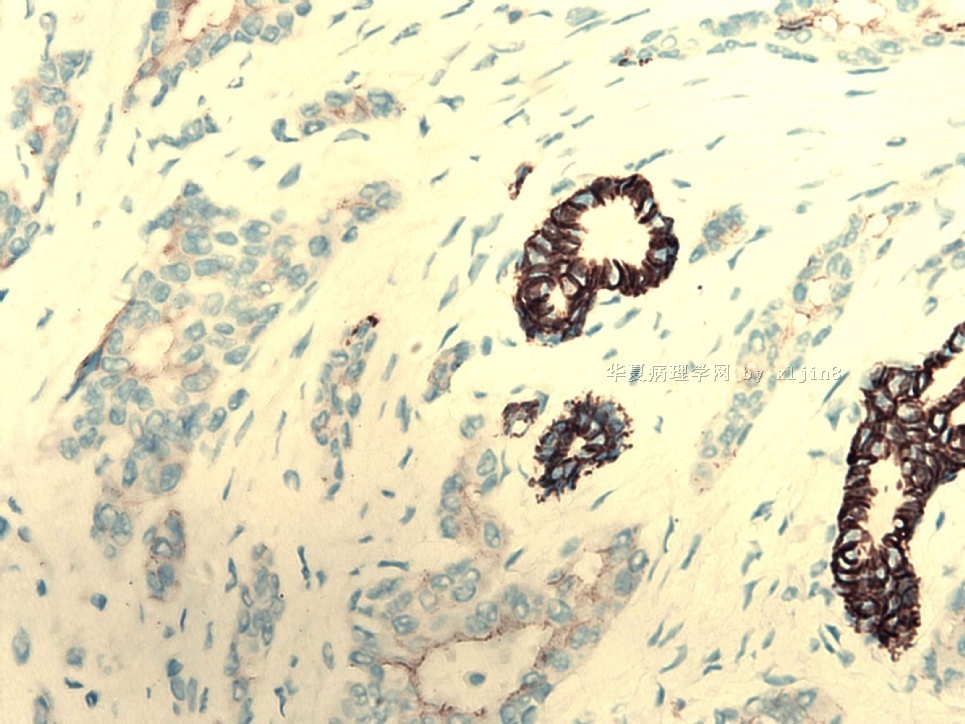
(1)大部分小管结构E-Ca弱阳性,p120和34BE12阳性,提示小叶癌性质。
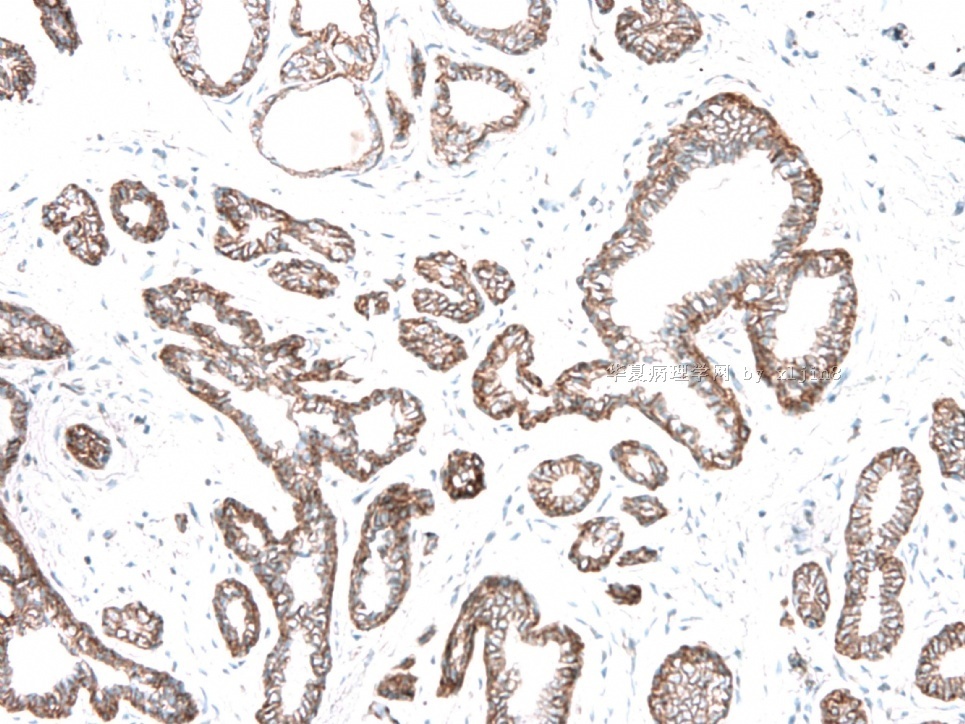
(2) 但23楼图6右侧有三个小导管明确的E-Ca强阳性,它们是癌吗?如果是,还存在导管癌性质的小管结构。要结合HE形态判断(免疫组化图中可见核形态与浸润成分不同,估计还是非癌性质的可能性大)。我起初想当然地认为它们是残留的正常导管,作为内对照出现的。
3、浸润的小管成分,HE:
1楼图4、9、10,可见小管成分与散在单个细胞是移行过渡的,推测小管成分是小叶癌性质。小叶癌的亚型可以形成小梁、条索、腺泡状,或中空小管,此时有人称为小管小叶癌tubulolobular carcinoma。另一种主流观点“肿瘤同时具有浸润性小叶癌和小管癌区域时,称为小管小叶癌。”
与小管癌相比,很多小管不是单层细胞,不是中空。它们更可能是高分化浸润性导管癌(但免疫组化不支持)。
我对本例的学习体会::
1、小管结构可能是小叶癌特殊亚型:小管小叶癌tubulolobular carcinoma
2、小管结构可能不是小管癌。
3、小管结构可能不是导管癌。
4、印像:浸润性小叶癌+小管小叶癌+小叶原位癌
Twenty-four examples of tubulolobular carcinoma were found among 1665 tumors in the National Surgical Adjuvant Breast Project (NSABP) series reviewed by Fisher et al. (68). These lesions, which constituted 1.4% of the series, were composed of small tubules as well as cords of tumor cells growing in the linear arrangement of classical invasive lobular carcinoma. Because it had many features intermediate between classical invasive lobular and tubular carcinoma, including a less favorable prognosis than tubular carcinoma, the authors concluded that tubulolobular carcinoma should be regarded as a separate variant of invasive lobular carcinoma. Illustrations and a discussion of tubulolobular carcinoma can be found in Chapter 13.
小管小叶癌两种成分:小管;经典型小叶癌那样的线性排列的肿瘤细胞条索。作者结论:小管小叶癌的性质介于经典型浸润性小叶癌与小管癌之间。
68. Fisher ER, Gregorio RM, Redmond C, et al. Tubulolobular invasive breast carcinoma: A variant of lobular invasive cancer. Hum Pathol 1977;8:679–683.
Chapter 13
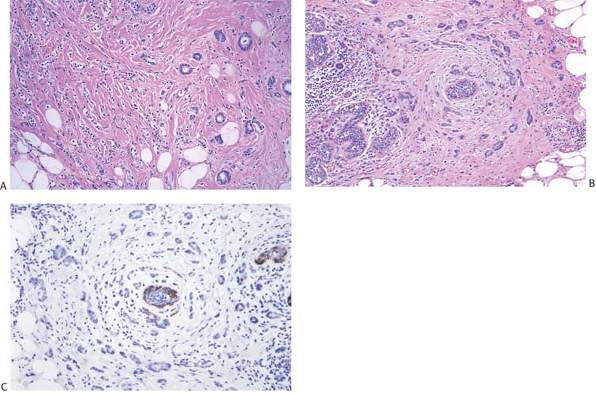
When the tumor has areas of invasive lobular and tubular carcinoma, it is referred to as tubulolobular carcinoma (Fig. 13.12). Tubulolobular carcinomas range in from 0.3 cm to 2.5 cm in greatest dimension (mean, about 1.3 cm) (41,42,43). In situ carcinoma found in the majority of cases consists of lobular carcinoma in situ (LCIS), ductal carcinoma in situ (DCIS), or LCIS and DCIS (41,42,43). DCIS alone is found more often in pure tubular carcinoma than in tubulolobular carcinoma, whereas tubulolobular carcinomas is more likely to be accompanied by LCIS only (41,42).
肿瘤同时具有浸润性小叶癌和小管癌区域时,称为小管小叶癌。0.3-2.4cm(平均1.3cm)。原位癌成分可以是LCIS、DCIS或兼有。纯小管癌常仅有DCIS,而小管小叶癌可能仅有LCIS。
Varying proportions of tubular and invasive lobular carcinoma are found in tubulolobular carcinomas. In one study of 11 cases, tubular and lobular carcinoma were nearly equally present in 3 (27%), lobular carcinoma was predominant in 5 (46%), and the tubular pattern was more pronounced in 3 (27%) (43). Almost all tubulolobular carcinomas are
immunoreactive for ERs and PRs (41,43). They are only rarely HER2/neu positive (43).
Multifocality is more frequent in tubulolobular carcinoma than in pure tubular carcinoma, having been found in 19% (42) and 29% (41) of tubulolobular cases in two studies. By comparison the frequency of multifocality in pure tubular carcinomas was 10% (41) and 20% (41). These patients are slightly more likely to have axillary lymph node metastases than are women with pure tubular carcinoma (41,42,43), but a prognosis closer to that of pure tubular carcinoma than that of invasive lobular carcinoma (41,42).比纯小管癌的腋淋巴结转移率轻度增加。
The precise position of tubulolobular carcinoma in the classification of breast carcinomas is uncertain. Tubulolobular carcinoma has been regarded as a variant of tubular carcinoma by some authors, and as a form of invasive lobular carcinoma by others. The observation that almost all tubulolobular
carcinomas in 3 studies were E-cadherin positive supports ductal histogenesis, since loss of E-cadherin reactivity is associated with invasive lobular carcinoma (42,43,44). E-cadherin immunoreactivity was found in invasive tubular and invasive lobular components, even in tumors wherein the lobular pattern was more prominent. In one study α-catenin and β-catenin were expressed in 50% and 62.5%, respectively, of tubulolobular carcinomas (44). Esposito et al. (43) detected membranous reactivity for α-, β-, and χ-catenin in all tubulolobular and tubular carcinomas they studied. Infiltrating lobular carcinomas displayed cytoplasmic staining for β–and χ-catenin but no reactivity for α-catenin. In this study all tubular and tubulolobular carcinomas had membranous reactivity for E-cadherin. Membranous E-cadherin reactivity is absent from lobular carcinomas. Immunoreactivity for the high-molecular-weight cytokeratin 34βE12 (K903) was observed in about 50% of tubular, tubulolobular, and invasive lobular carcinomas. Wheeler et al. (42) found that 25 of 27 tubulolobular carcinomas were immunoreactive for the high-molecular-weight cytokeratin K903, a marker that has been associated with lobular differentiation (45,46). Overall the mixed immunophenotype of tubulolobular carcinomas reflects the ductal and lobular histologic components of these tumors, with the preponderance of evidence supporting ductal histogenesis.
部分作者认为小管小叶癌是小管癌的亚型,而其他人认为是浸润性小叶癌的亚型。E-ca和catenin系列以及34βE12 (K903)的表达报道不一,多为混合性表达,反映兼有导管和小叶分化,而以导管起源的证据为主。目前认为小管小叶癌预后好。
Three-dimensional modeling of tubular and tubulolobular carcinomas revealed a growth pattern in which cavitary glandular structures were connected by a network of slender, solid cords of single cells (47). In tubulolobular carcinomas the connecting network of single cells appeared to consist of longer strands, which might account for the histologic pattern suggestive of invasive lobular carcinoma.
As greater experience with tubulolobular carcinoma is obtained, it is likely to emerge as a separate subtype of mammary carcinoma, distinct from tubular and invasive lobular carcinoma. Presently, patients with tubulolobular carcinoma should be viewed as having a good prognosis. It remains to be seen if the prognosis equals the exceptionally favorable outcome of pure tubular carcinoma.
41. Green I, McCormick B, Cranor M, et al. A comparative study of pure tubular and tubulolobular carcinoma of the breast. Am J Surg Pathol 1997;21:653–657.
42. Wheeler DT, Tai LH, Bratthauer GL, et al. Tubulolobular carcinoma of the breast. An analysis of 27 cases of a tumor with a hybrid morphology and immunoprofile. Am J Surg Pathol 2004;28:1587–1593.
43. Esposito NN, Chivukula M, Dabbs DJ. The ductal phenotypic expression of the E-cadherin/catenin complex in tubulolobular carcinoma of the breast: An immunohistochemical and clinicopathologic study. Mod Pathol 2007;20:130–138.
44. Kuroda H, Tamaru J, Takeuchi I, et al. Expression of E-cadherin, α-catenin, and β-catenin in tubulolobular carcinoma of the breast. Virchows Arch 2006;448:500–505.
45. Bratthauer GL, Miettinen M, Tavassoli FA. Cytokeratin immunoreactivity in lobular intraepithelial neoplasia. J Histochem Cytochem 2003;51:1527–1531.
46. Bratthauer GL, Monifar F, Stamatakos MD, et al. Combined E-cadherin and high molecular weight cytokeratin immunoprofile differentiates lobular, ductal, and hybrid mammary intraepithelial neoplasias. Hum Pathol 2002;33:620–627.
47. Marchio C, Sapino A, Arisio R, et al. A new vision of tubular and tubulo-lobular carcinomas of the breast, as revealed by 3-D modeling. Histopathology 2006;48:556–562.
(英文资料来自Rosen's Breast Pathology, 3rd Edition)
名称:图1
描述:图1
华夏病理/粉蓝医疗
为基层医院病理科提供全面解决方案,
努力让人人享有便捷准确可靠的病理诊断服务。











