
















| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- 系统学病理及英语病理学之一
 图1
图1 图2
图2 图3
图3 图4
图4 图5
图5 图6
图6 图7
图7 图8
图8
1a Chronic Pancreatitis
Chronic pancreatitis is characterized by patchy fibrous replacement of whole lobules or parts of lobules, focal fat necrosis in different stages, and chronic inflammation. Grossly, depending on the etiology and degree of injury, the gland may be slightly firm but have a normal outline, lobular pattern, and color. Severe cases may be smaller than normal, bosselated, rock-hard, and display foci of fat necrosis, calcification, or fully developed calculi.
Gross: This chronically inflamed pancreas is small and scarred. The dilated pancreatic duct contains a stone (arrow). Chronic Pancreatitis with stone
onmouseover="showMenu(this.id, 0, 1)"> X-ray: This is an example of chronic pancreatitis with marked calcification of the pancreatic parenchyma. This calcification could be demonstrated by an x-ray of the abdomen.
onmouseover="showMenu(this.id, 0, 1)"> Gross: These are cross sections taken through the head of the pancreas in chronic pancreatitis. The sections of pancreas which you have in your class sets were taken in a similar fashion. Notice that the dense white fibrous scarring has almost totally obliterated the lobular architecture of the pancreas.
onmouseover="showMenu(this.id, 0, 1)"> This is a low magnification picture of the H&E slide of chronic pancreatitis in your class set. This particular patient had an obstructive type of pancreatitis due to carcinoma of the head of the pancreas. The lobular architecture of the pancreas is accentuated by broad bands of interstitial fibrosis.
onmouseover="showMenu(this.id, 0, 1)"> The fibrous scarring of the pancreas is highlighted with the Trichrome stain. The fibrous septa appear as blue bands surrounding the residual pancreatic lobules, which stain red. Shows the dense interstitial fibrosis surrounding two pancreatic lobules. Note there is also an increase in intralobular fibrous tissue and there is chronic inflammation.
The fibrous scarring of the pancreas is highlighted with the Trichrome stain. The fibrous septa appear as blue bands surrounding the residual pancreatic lobules, which stain red. Shows the dense interstitial fibrosis surrounding two pancreatic lobules. Note there is also an increase in intralobular fibrous tissue and there is chronic inflammation.
onmouseover="showMenu(this.id, 0, 1)"> The exocrine portion of the gland is most severely affected. There is almost total atrophy and fibrous replacement of pancreatic acini with relative preservation of the pancreatic ducts and islets of Langerhans (arrows). The intralobular pancreatic ductules are irregularly shaped and are embedded in chronically inflamed fibrous tissue. Several preserved islets are marked with arrows
Higher magnification shows preservation of the islets of Langerhans to better advantage (arrows).
标签:

- 赚点散碎银子养家,乐呵呵的穿衣吃饭
×参考诊断
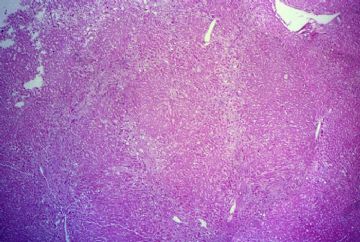 图1
图1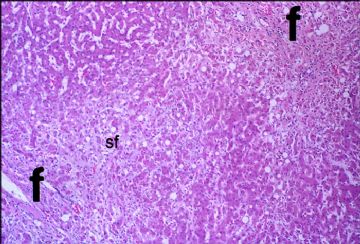 图2
图2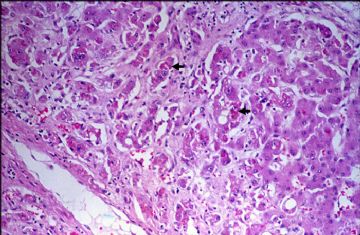 图3
图3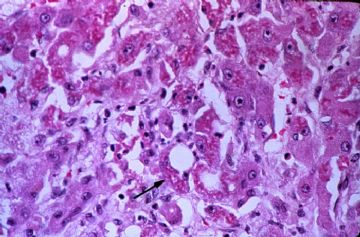 图4
图4
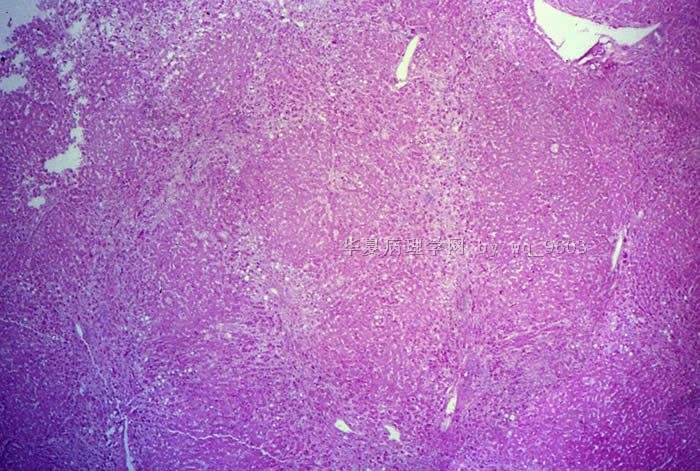
Slide 1
The hepatic architecture is disturbed by portal and sinusoidal (pericellular) fibrosis. Some of the fibrous bands are just beginning to link-up to circumscribe nodules of hepatic parenchyma. This patient not only has very early cirrhosis but also acute alcoholic hepat
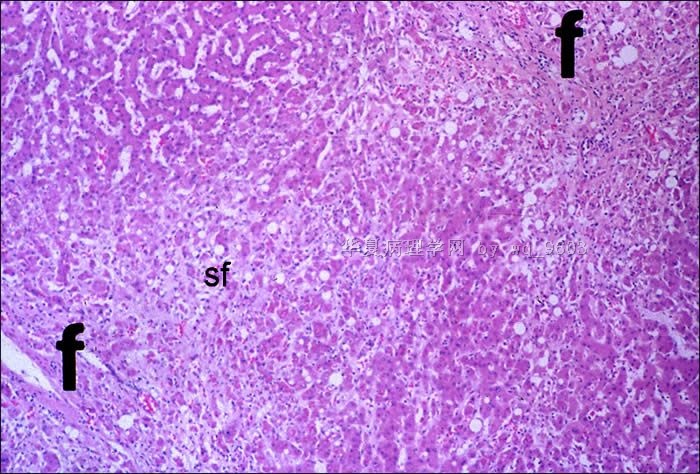
Slide 2
Shows portal fibrosis (f) and sinusoidal fibrosis (sf). The latter may be especially common in the livers of patients with severe alcoholic and non-alcoholic types of steatohepatitis.
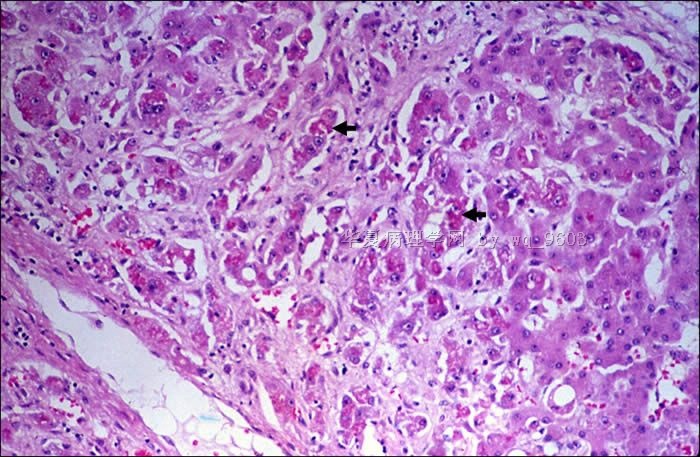
Slide 3
Shows prominent pericellular fibrosis (individual and small clusters of hepatocytes completely surrounded by fibrous tissue). This sinusoidal or pericellular fibrosis is usually most severe in centrilobular regions and is a common feature of alcoholic hepatitis. Note that many of the hepatocytes contain Mallory bodies.
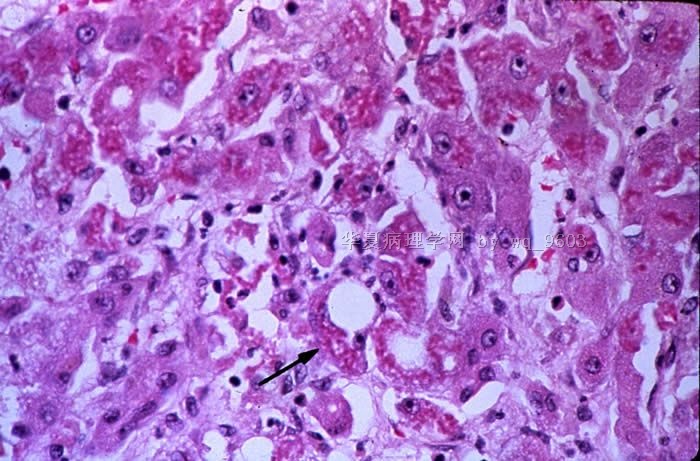
Slide 4
Mallory bodies (arrow) appear as violaceous, ropy, hyaline inclusions located in the perinuclear region of the cytoplasm of the hepatocytes. They are composed of degenerated intermediate (cytokeratin) filaments of the cytoskeleton of the liver cells. Mallory bodies are chemotactic for neutrophils, and polymorphonuclear inflammation is characteristic of alcoholic hepatitis. As a matter of fact, some investigators feel that enzymes released by polymorphonuclear leukocytes may be responsible for the pericellular fibrosis seen in alcoholic liver disease. You will remember that the inflammation in acute viral hepatitis, on the other hand, is predominantly mononuclear.
- 赚点散碎银子养家,乐呵呵的穿衣吃饭
 图1
图1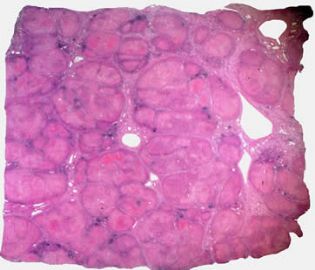 图2
图2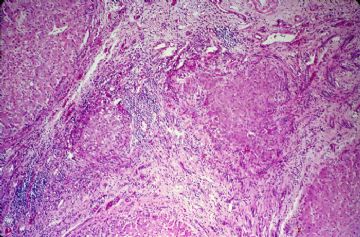 图3
图3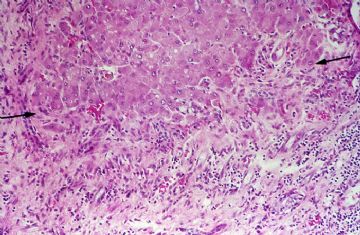 图4
图4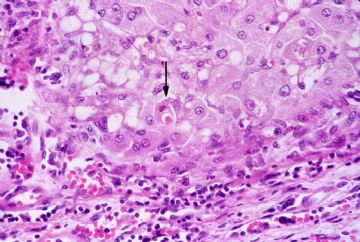 图5
图5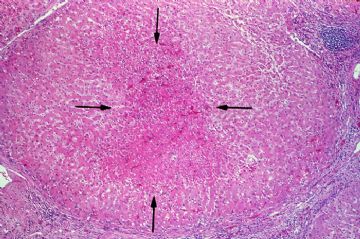 图6
图6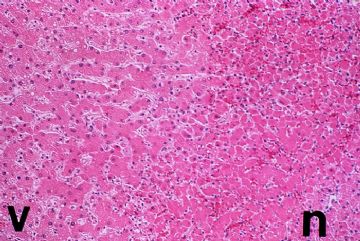 图7
图7
Slide 1
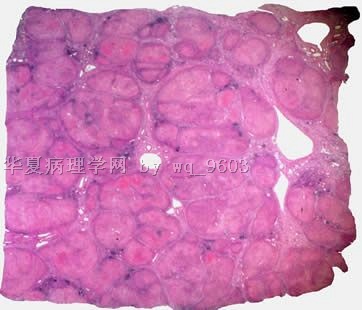
Gross: You will recall from your lecture that cirrhosis is a chronic disease of the liver characterized by diffuse destruction and regeneration of hepatocytes, as well as subsequent fibrous scarring that results in disorganization of the lobular architecture. Put more simply, cirrhosis is characterized by fibrosis of the liver and regenerative parenchymal nodules. Cirrhosis may be divided morphologically into two basic types: micronodular cirrhosis and macronodular cirrhosis. The micronodular pattern has uniform regenerative nodules of lobular size or smaller (3 mm in diameter and less) and in the U.S. is usually caused by alcohol. In macronodular cirrhosis, the regenerative nodules are large and irregular in size and shape. The fibrous septa are often broad. Macronodular cirrhosis corresponds loosely to the older terms "post-necrotic" or "multilobular" cirrhosis and in the U.S. is most often seen following chronic active viral hepatitis. This is an example of cirrhosis caused by hepatitis C.
Slide 2
Is a low power view of the actual slide in your class set. The hepatic architecture is disturbed by broad bands of fibrosis that completely circumscribe irregularly sized and shaped nodules of regenerating hepatic parenchyma. These nodules range in size from less than 1 mm in diameter to greater than 5 mm in diameter。
Slide 3
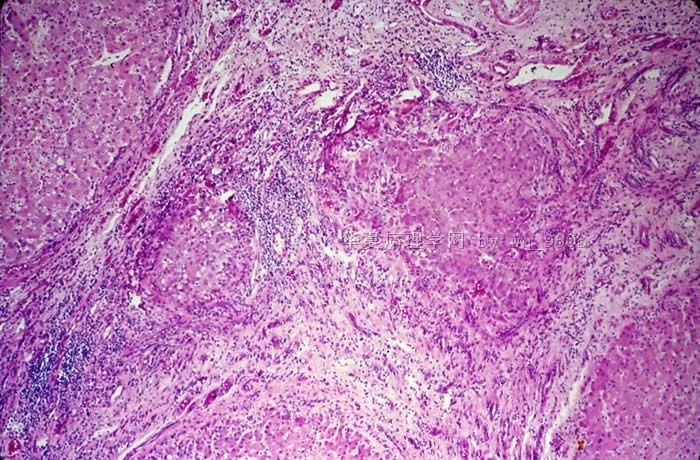
Shows at higher power the broad fibrous septa which completely surround regenerating nodules of hepatic parenchyma. This patient's cirrhosis resulted from chronic active hepatitis C and there is ongoing chronic inflammation and necrosis in this liver.
Slide 4
Is taken at the margin of a regenerative nodule and a fibrous scar (double arrows). Note the irregular contour of the regenerative nodules and the intense necroinflammatory activity (“piecemeal necrosis”) at the interface of the fibrous septa and the hepatic parenchyma
Slide 5
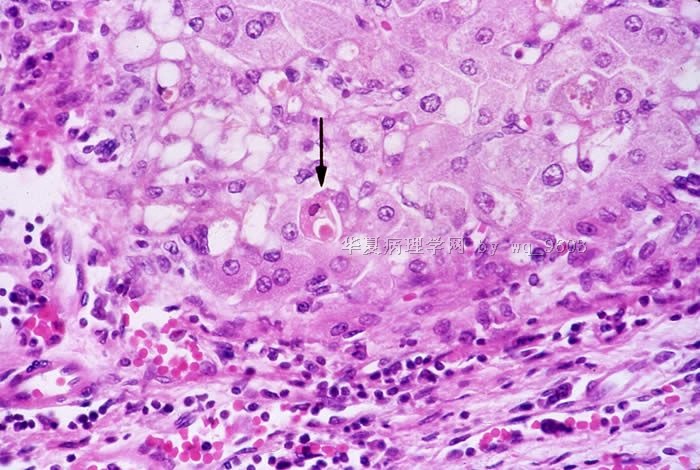
If you look carefully you may be able to find ongoing apoptosis of infected hepatocytes. The arrow indicates an acidophilic body
Slide 6
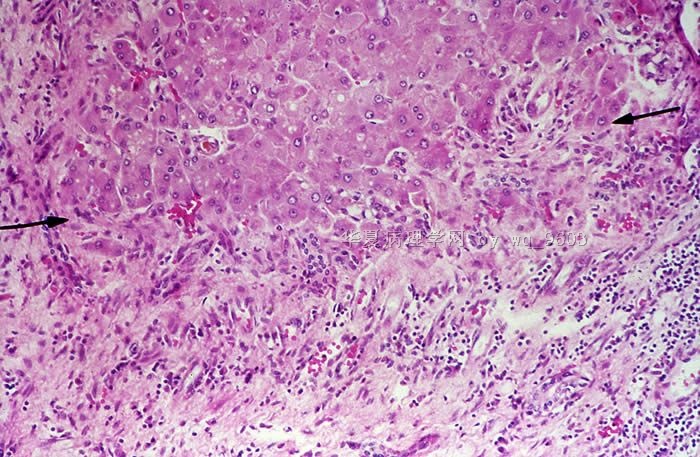
You may be puzzled to note that many of the hepatocytes within the center of the regenerative nodules are shrunken and more eosinophilic. These centrally located hepatocytes have undergone ischemic necrosis. You will recall from your syllabus that the fibrosis and regenerative nodules of cirrhosis destroy the hepatic architecture and disrupt blood flow through the liver. Often the hepatocytes at the center of the regenerative nodules are only marginally supplied with blood. Should the patient suffer a hypotensive episode, as typically occurs from bleeding esophageal varices, the centers of the regenerative nodules will infarct.
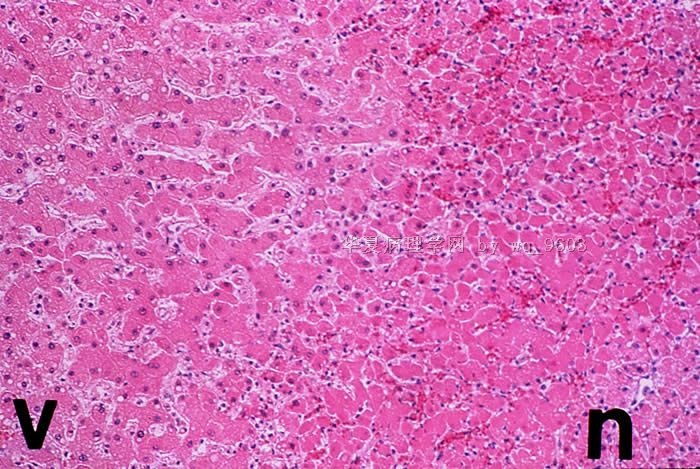
Slide 7
Shows at higher power, the demarcation between the peripherally located, viable (V) hepatocytes and the more centrally located, necrotic (N) hepatocytes.
- 赚点散碎银子养家,乐呵呵的穿衣吃饭
 图1
图1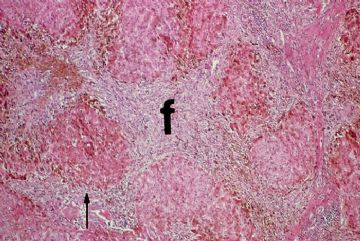 图2
图2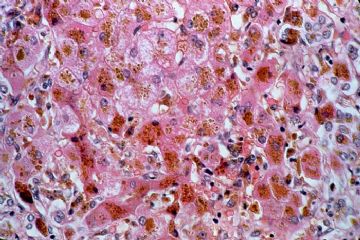 图3
图3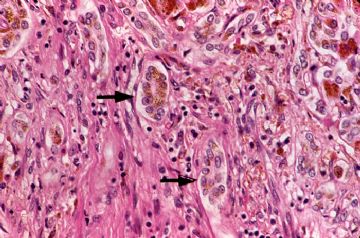 图4
图4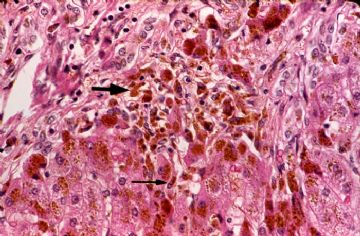 图5
图5
Primary Hemochromatosis of the Liver
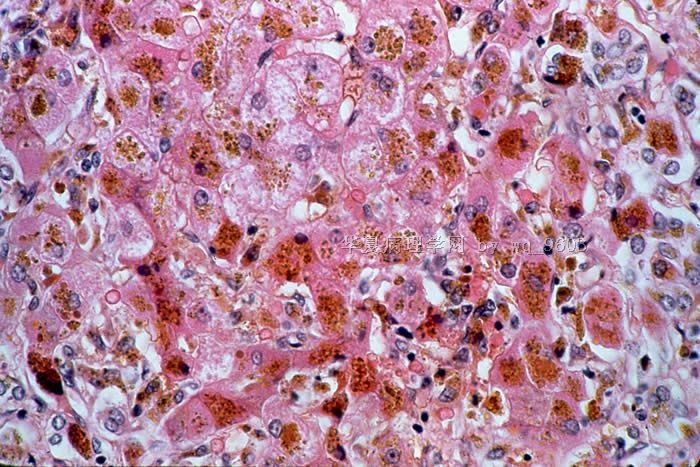
The basic pathologic feature in hemochromatosis is the deposition of massive amounts of iron in various organs of the body. Because the liver is the major storage site for iron and plays a key role in all conditions of iron overload, it is often severely affected. The deposition of iron in hepatic parenchymal cells leads to tissue damage, fibrosis, and eventually cirrhosis. The actual molecular mechanism by which iron causes hepatic damage is not known, but it is felt that iron alters oxidative phosphorylation. Hemochromatosis may be primary (hereditary) or secondary (increased dietary intake; multiple transfusions; hemolytic conditions). The changes in the liver in primary hemochromatosis depend on the stage of disease. In the early stages there is deposition of iron in the hepatic parenchymal cells but no alteration of the hepatic architecture. The liver is large and may have a rust or dark brown color。
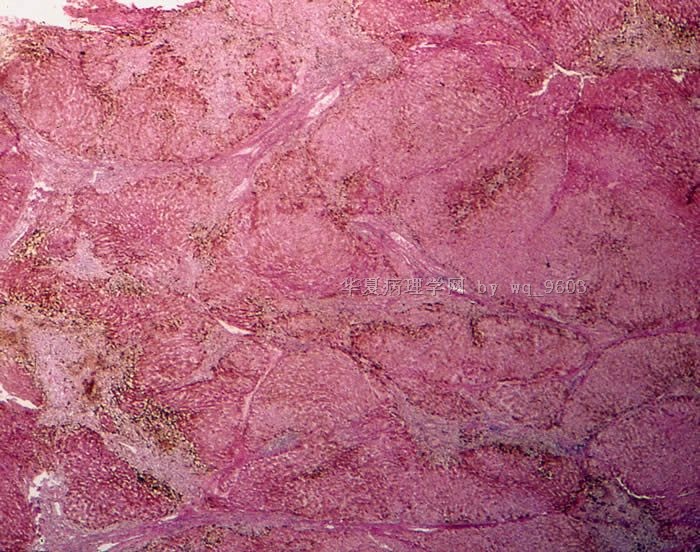
Slide 1
The example of hemochromatosis in your class set is an example of the late stages of the disease. Bands of fibrosis have completely circumscribed regenerating nodules of hepatic parenchyma. This is an example of cirrhosis caused by a metabolic disease.
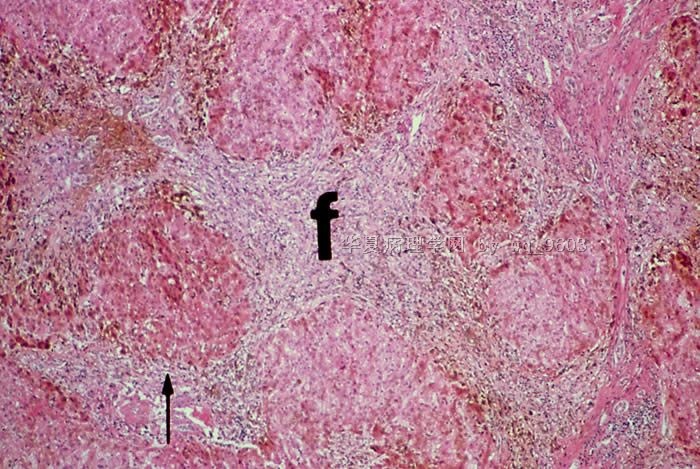
Slide 2
Higher magnification shows these chronically inflamed bands of fibrosis (F) surrounding islands of regenerating hepatic parenchyma (arrow). Note that the regenerative nodules lack central veins. Even at this magnification you may be able to appreciate the dark-brown hemosiderin pigment distributed throughout the liver.
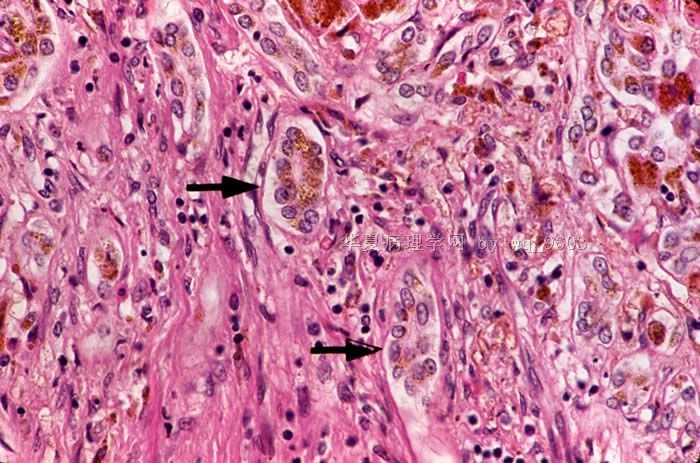
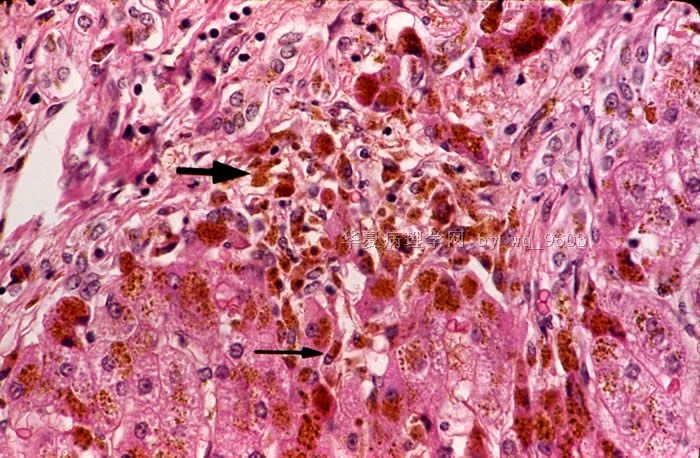
The golden-brown refractile hemosiderin granules are present within hepatocytes (Slide 3), within bile duct epithelium (Slide 4: Arrows), within Kupffer cells (Slide 5: Skinny Arrow) and within portal macrophages (Slide 5: Fat Arrow).
Slide 3
The golden-brown refractile hemosiderin granules are present within hepatocytes.
Slide 4
The golden-brown refractile hemosiderin granules are present within bile duct epithelium (Arrows).
Slide 5
The golden-brown refractile hemosiderin granules are present within Kupffer cells (Skinny Arrow) and within portal macrophages (Fat Arrow).
- 赚点散碎银子养家,乐呵呵的穿衣吃饭
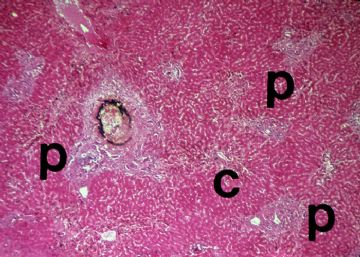 图1
图1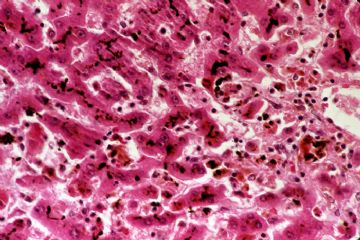 图2
图2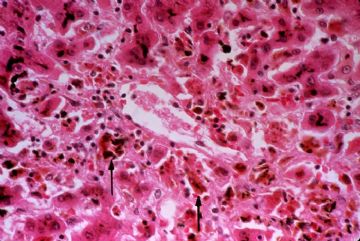 图3
图3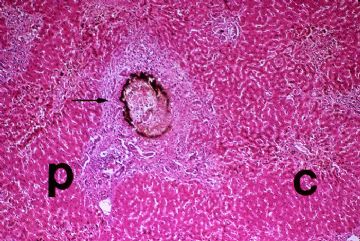 图4
图4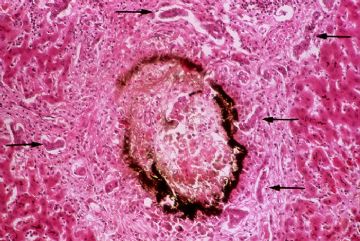 图5
图5
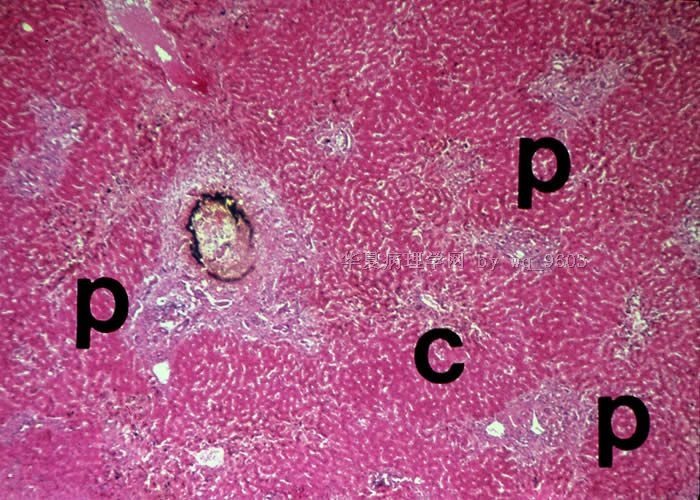
Liver Following Prolonged Extrahepatic Obstruction
Extrahepatic obstruction in adults may be due to a number of causes, including inflammatory fibrous strictures of the extrahepatic ducts, impacted calculi, or neoplasms of the extrahepatic ducts or head of the pancreas. The pathologic changes that are seen in the liver are dependent on the duration of the obstruction, but long-standing obstruction will eventually progress to micronodular cirrhosis. The histologic section of liver that you have in your class set was obtained from a patient who had obstruction of the intrapancreatic portion of the common bile duct of several months duration due to a carcinoma in the head of the pancreas。
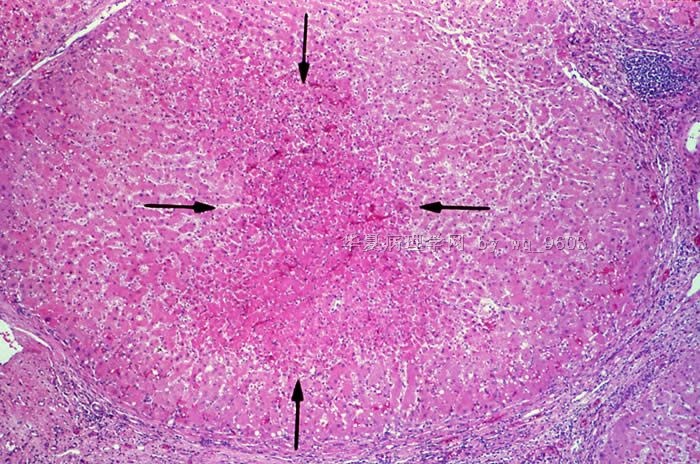
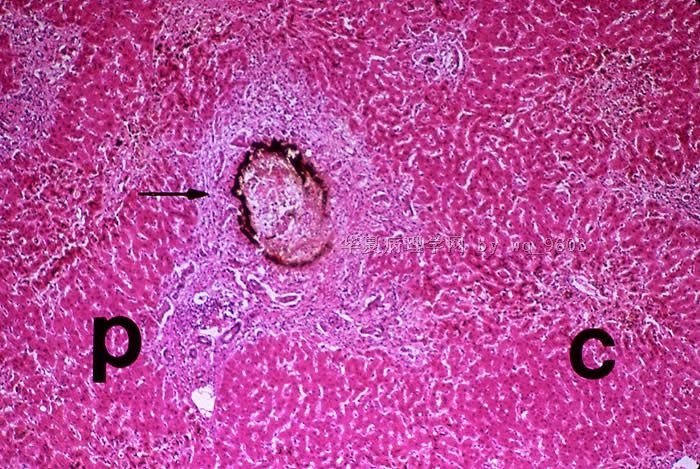
Slide 1
It can be seen at low power that this patient already has some portal scarring of the liver, but does not yet have cirrhosis. There are histopathologic changes in both the portal (P) and central (C) areas of this liver that you should be careful to examine.
Slide 2
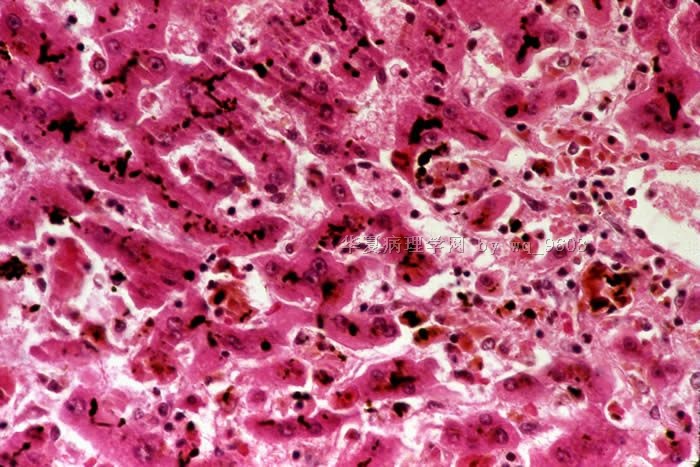
One of the earliest visible changes seen in the liver following extrahepatic obstruction is bile stasis. This is typically most severe in the centrilobular areas. The bile pigment is present as fine granules in the cytoplasm of hepatocytes and as very prominent bile plugs in the biliary canaliculi. Note that the biliary canaliculi between the hepatocytes are stuffed with dark green bile pigment.
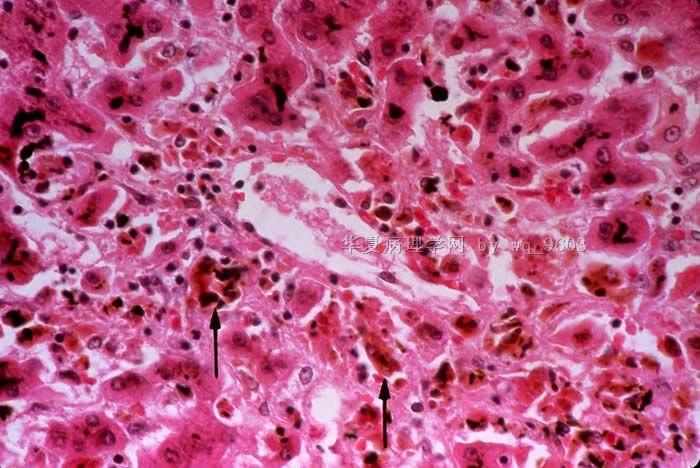
Slide 3
The bile pigment is toxic to hepatocytes which become swollen, showing rarefaction of the cytoplasm referred to as feathery degeneration. Some of these hepatocytes will die and be phagocytized by Kupffer cells which then become latent with bile pigment. This picture is taken from the centrilobular region of the liver and you will see a large central vein in the center of the photograph. Note that many of the pericentral hepatocytes have died and have been phagocytized by Kupffer cells (arrows) which contain bile pigment.
Slide 4
With time, the cholestasis progresses and may be seen in the periportal parenchyma. Occasionally, focal collections of dead, bile stained hepatocytes may be seen. These are called bile infarcts (arrow). They are usually seen in the periportal parenchyma.
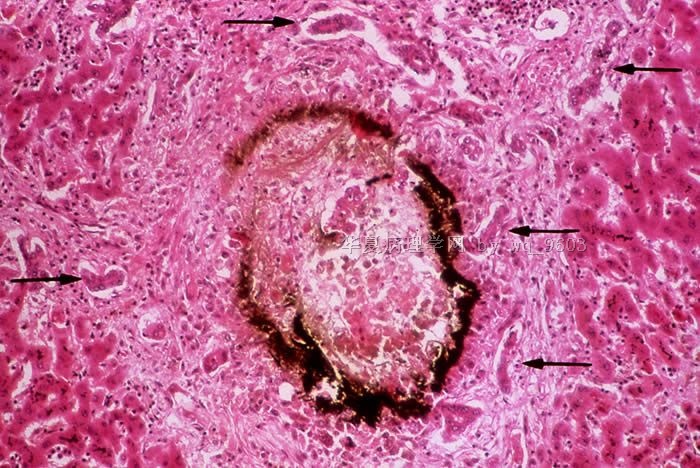
Slide 5
Shows a higher magnification a periportal bile infarct. After several weeks of unrelieved obstruction, bile ductular proliferation (arrows) may be seen. With time there is progressive portal fibrosis. Eventually, these fibrous septa link to completely circumscribe islands of hepatic parenchyma and the patient will develop cirrhosis
- 赚点散碎银子养家,乐呵呵的穿衣吃饭
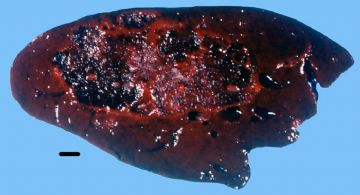 图1
图1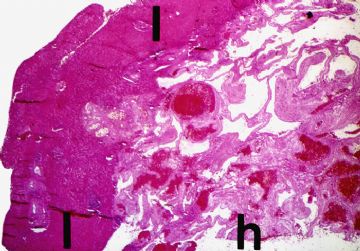 图2
图2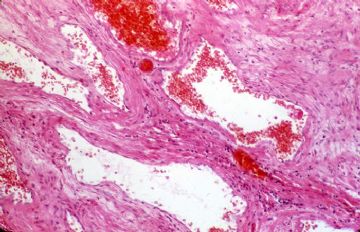 图3
图3
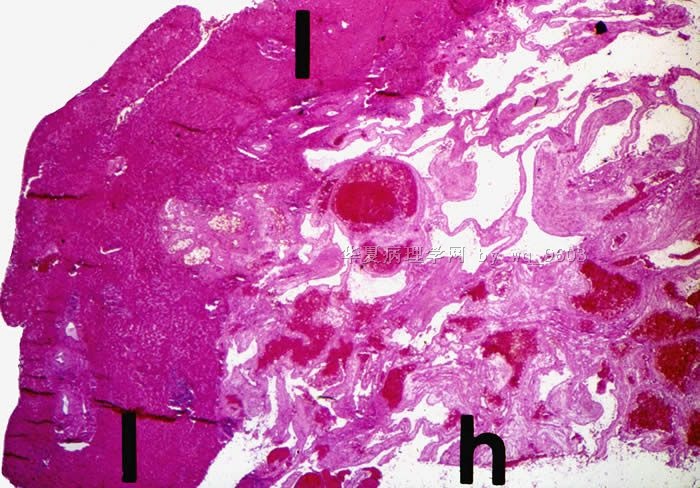
Cavernous Hemangioma of the Liver
The cavernous hemangioma is the most common benign tumor of the liver, occurring at all ages and in both sexes. The majority are asymptomatic, but occasionally they may cause vague abdominal symptoms following episodes of thrombosis. Even more rarely, they may rupture and cause intraperitoneal hemorrhage.
Slide 1
Grossly, most hemangiomas are solitary and under 5 cm in size. This is a particularly large one, measuring about 9 cm. in greatest dimension. It is a soft pulpy, hemorrhagic mass with a spongy consistency.
Slide 2
This is a low power view showing the junction of the normal liver (L) at the left with the hemangioma (h) at the right.
Slide 3
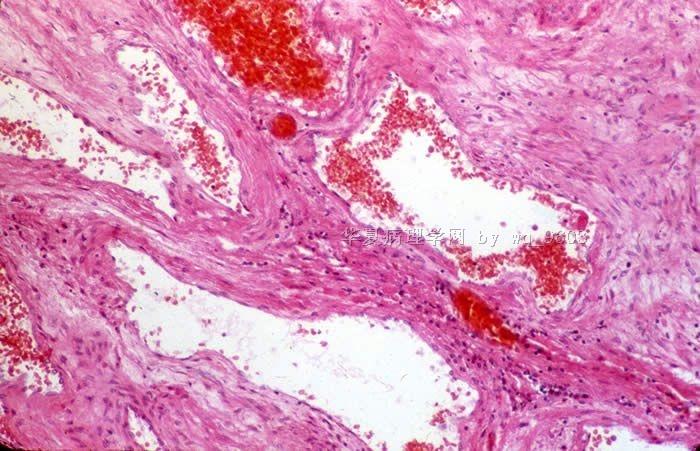
The tumor is composed of endothelial-lined, blood-filled cavernous spaces separated by a fibromyxoid stroma.
- 赚点散碎银子养家,乐呵呵的穿衣吃饭
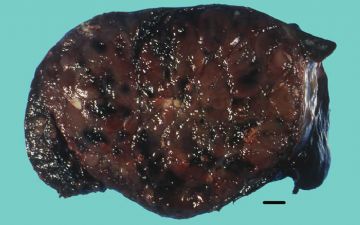 图1
图1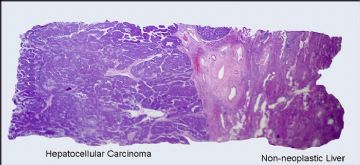 图2
图2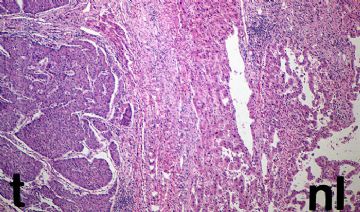 图3
图3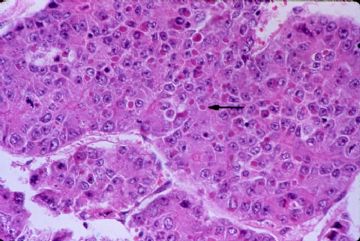 图4
图4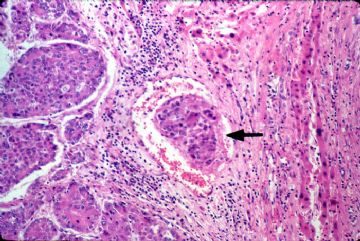 图5
图5
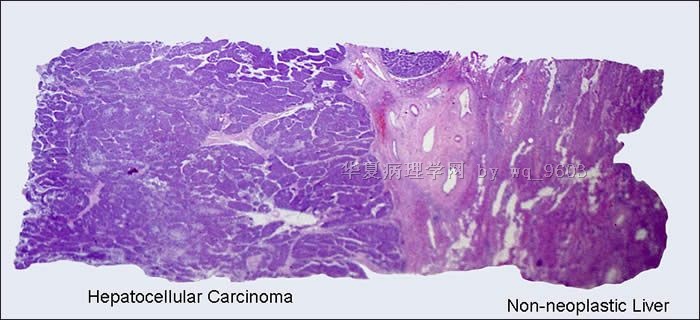
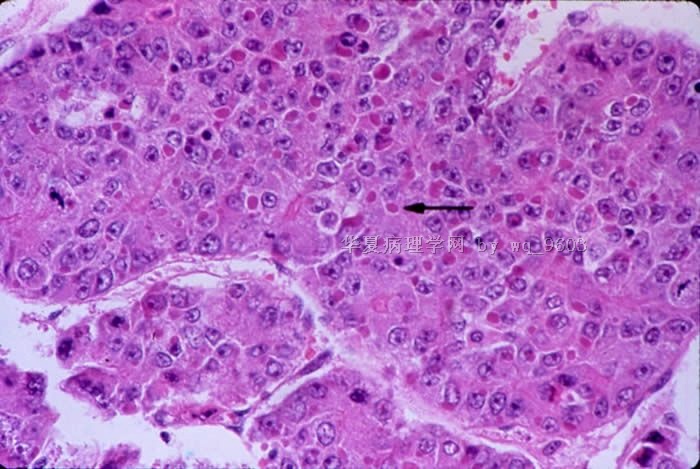
Hepatocellular Carcinoma
Slide 1
Gross: Hepatocellular carcinoma has a variable macroscopic appearance. This particular hepatocellular carcinoma grew as a predominantly solitary mass occupying most of the right lobe of the liver of a 69 year old white male. The tumor is predominantly tan-brown but you will notice focal areas of yellow necrosis as well as dark red areas of hemorrhage.
Slide 2
The histologic section in your class set was taken at the junction of the tumor and the non-neoplastic liver.
Slide 3
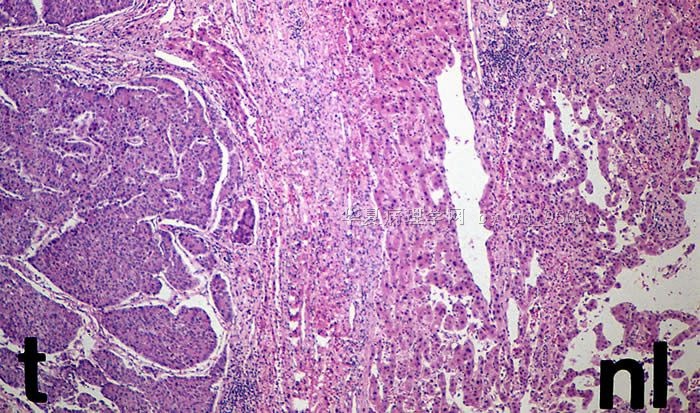
The junction of tumor and normal liver is seen to better advantage at higher power. The hepatic parenchyma at the edge of the tumor is compressed, giving the false impression that the carcinoma is encapsulated.
Slide 4
The histologic appearance of hepatocellular carcinoma is also extremely variegated. Many different histologic patterns may be seen, but most are only important to surgical pathologists. This particular carcinoma is growing in nests and thick cords that are separated form one another by thin-walled sinusoids. Cytologically, the tumor cells bear some resemblance to normal hepatocytes, but they are slightly larger, have more irregular nuclei, and prominent nuclei. There are also numerous mitotic figures. You may also notice that many of the tumor cells contain intracytoplasmic violaceous, hyaline globules (arrow) that represent proteins produced by the tumor cells. Occasionally, these hyaline globules represent collection of alpha-fetoprotein or alpha-1-antitrypsin.
Slide 5
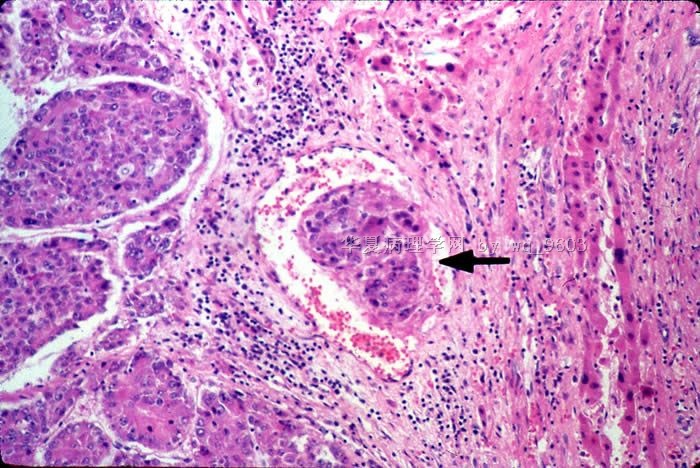
Hepatocellular carcinoma shows a marked tendency to spread by intrahepatic veins, both hepatic and portal. Most of the slides in your class sets will show tumor thrombi within portal vessels (arrow).
- 赚点散碎银子养家,乐呵呵的穿衣吃饭











