









| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
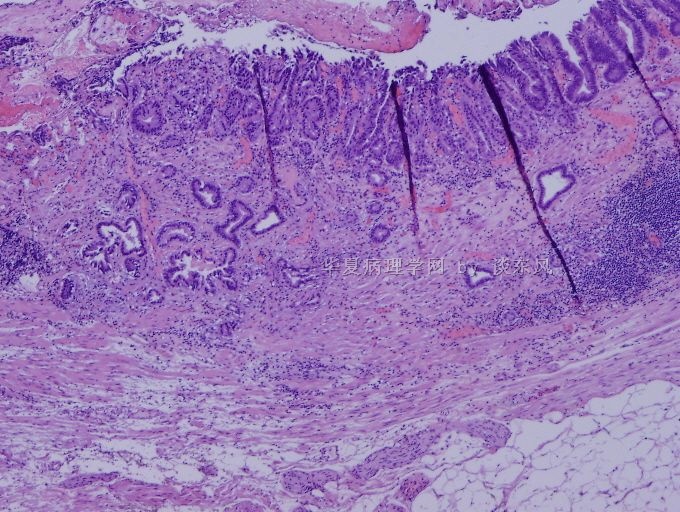
- 谈东风病例9 Case T0009:食道病变, 有浸润吗? If yes, How deep?
 图1
图1 图2
图2 图3
图3 图4
图4
| 姓 名: | ××× | 性别: | 58 | 年龄: | male |
| 标本名称: | |||||
| 简要病史: | Recent dysphasia. | ||||
| 肉眼检查: | 1.2cm lesion in the middle portion of esophagus. | ||||
How deep is the lesion??
Diagnosis: focal early adenocarcinoma within the muscularis mucosae (病变应是位于黏膜肌层).
This outside case was called as an invasive adencarcinoma involving the muscularis propria (肌层).
1. The muscularis mucosae in the esophagus, particularly in the lower middle and distal parts of esophagus, can be very thick. In the Barrett's esophagus, the muscularis mucosae would be "double layer". It is common error to call this muscularis mucosae as muscularis propria. But the tumor stage is significantly different.
2. Adenocarcinoma of the esophagus is very common in the western countries. For example, adenocarcinoma of the esophagus in U.S.A. is much more common than adenocarcinoma of the stomach. Most adenocarcinomas in the esophagus arise in a background of Barrett's esophagus (also see the second case in 第 14 楼). The criteria to call early adenocarcinoma is mainly based on a) archiectural disorder and b)early invasiveness, namely, the neoplastic glands penetrate through the basement membrane into the muscularis mucosae. Sometimes, the changes is very subtle, like this case, in which only one gland shows malignant transformation. The case in is more obvious, like the case in 第 14 楼.
标签:
-
本帖最后由 于 2010-06-06 02:19:00 编辑
×参考诊断
The discussion is added below. Thanks.
| 以下是引用艾佳在2010-5-27 8:52:00的发言: 是Barrett食管恶变吧。 |
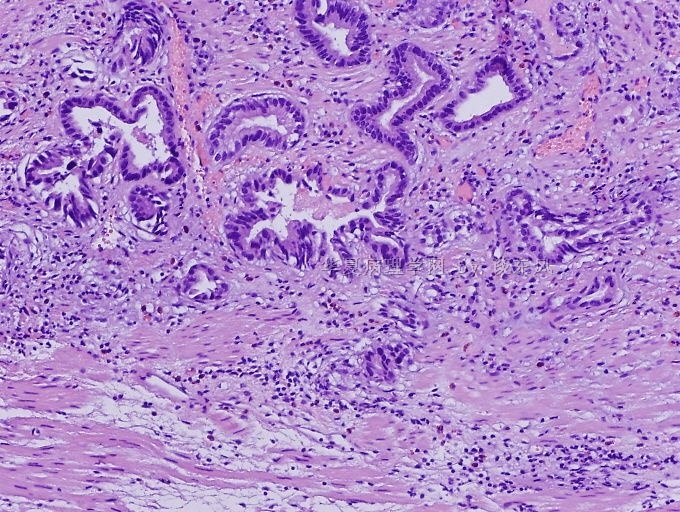
There is a background of Barrett's mucosa in the surface. A couple of glands with obvious architectural and cytological atypia, "invading" to "smooth muscle."
The questions are 1) any cancer? and if yes, 2) how deep?
| 以下是引用kint123在2010-6-3 6:24:00的发言:
1.2cm lesion in the middle portion of esophagus. 这应该是中段食管吧,这里也有“Barrett食管”一说? |
Excellent observation!
This is a consultation case from Sweden. Initially, we thought it may be an translational error. After email communications in English, I was informed that the patient has a long history of Barrett and this biopsy was taken about 6cm from the GE junction. In addition, there are two lesions, one 1.0cm in size and 4 cm from the GE junction, and another 1.1cm in size and 2cm from the GE junction. Overall impression is that the Barrett's lesion has focal pseduoregression, causing "islands" appearance endoscopically.
Nevertheless, the question of the case is how deep is the atypical glands.
The outside pathologist called "focal invasive carcinoma arising in a background of Barrett's mucosa. Tumor invades into the muscularis propria."
-
本帖最后由 于 2010-06-04 01:09:00 编辑
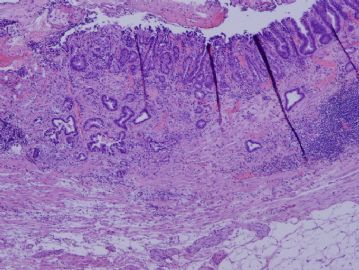 图1
图1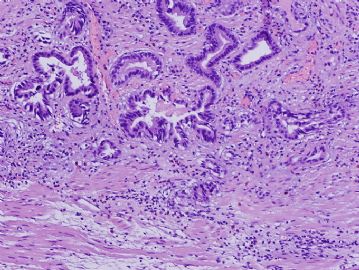 图2
图2
这个病例真是太难了!
如果是在胆囊看到类似的图像,可能考虑恶性吗?
表层的黏膜腺体分布存在极向——“具向表面伸长的方向感”,不象是恶性的。
肌层内“浸润”的腺体,上皮有一定异型,但不是高度异型,腺腔不完整,充满黏液,一侧黏液直接与肌组织“接壤”,可能是恶性腺体,也可能是良性病变腺体部分被破坏。尚能见到裸露于肌间的“黏液湖”,可能是恶性上皮产生的黏液在肌间浸润;也可能是良性上皮产生的黏液“溢出”到肌间隙,但是,范围不小,且黏液旁均未见到“异物反应”样的炎症反应。
不知道分子生物学检查是否有助于鉴别。但是,局部样本全包埋切片,以彻底了解局部组织的实况,似乎很有必要。
Good point.
The more photos are from a different case, showing similar pathology.

- “人生没有彩排,每一天都是现场直播”
| 以下是引用kint123在2010-6-4 6:57:00的发言:
岛状表现的Barrett食管?第一次听说,学习了。从谈老师的描述来看,这还是下段食管的,与胃食管交界很近 从第一张图看,病变应是位于黏膜肌层与黏膜下层交界的位置吧,尽管似有浸润,但细胞的异型性尚不足以诊断癌。类似病变发生于阑尾则类似于“恶性潜能未定型”,发生于乳腺类似于伴有异型增生的黏液囊肿样病变,由于各个系统的诊断标准差异很大,发生于这一部位的病变第一次见到,如我在工作中见到类似病变,倾向于保守一点的报告方式。 |
Very good.
The lesion is within 黏膜肌层 (muscularis mucosae).











