
图1")
图2")
图3")
图4")
图5")
图6")
图7")
图8")
图9")
图10")
























| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
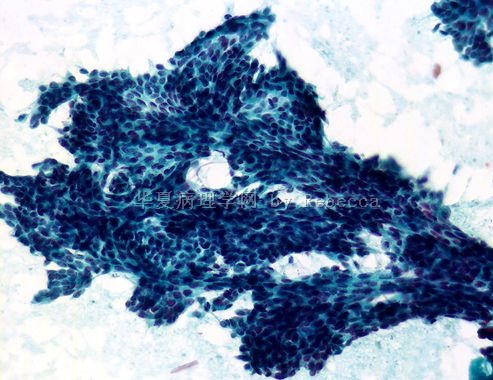
- 1例右侧乳晕下囊性包块FNAC(T1013)
图1") 图1
图1图2") 图2
图2图3") 图3
图3图4") 图4
图4图5") 图5
图5图6") 图6
图6图7") 图7
图7图8") 图8
图8图9") 图9
图9图10") 图10
图10
病史摘要:
女性患者王X 30岁
主诉:无意间发现右侧乳晕下一包块.
外科情况:右侧乳晕下可扪及一3.0X3.0大小的包块,边界清,活动度尚好。
B超:发现右侧乳晕下可见一29mmX28mm液性暗区,边界清晰。
临床诊断:右侧乳腺囊肿
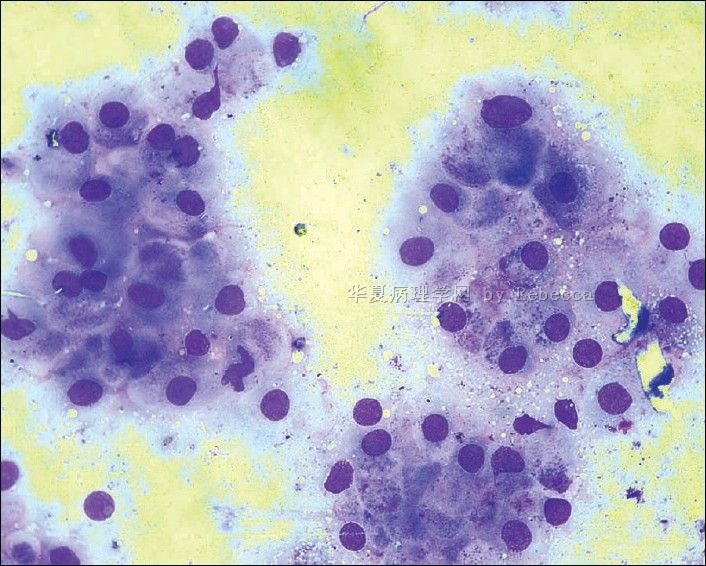
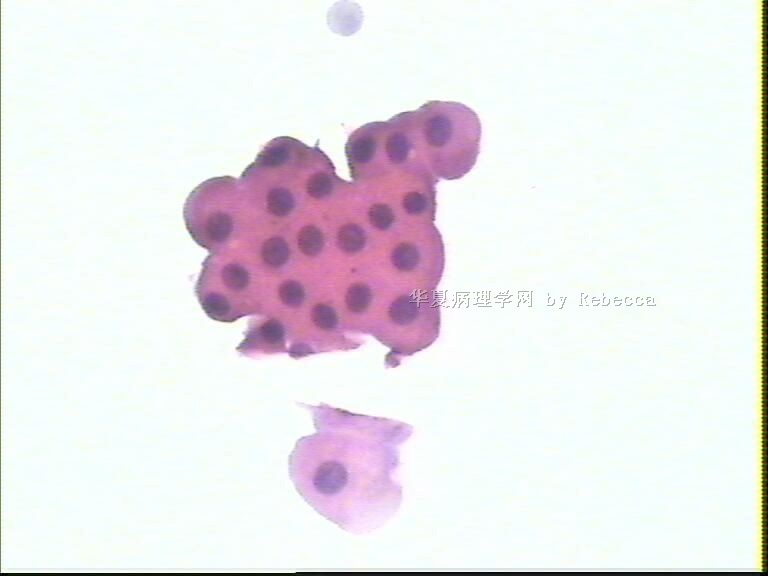
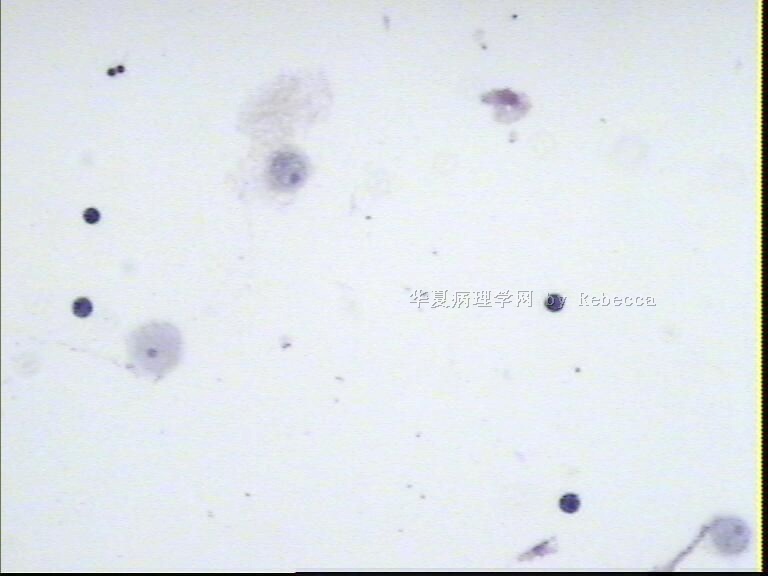
常规消毒下行细针吸取穿刺,抽吸出约7毫升淡咖啡色液体。全部离心,取试管底部沉淀物常规涂片、制片。HEX5
标签:
-
本帖最后由 于 2010-05-24 23:18:00 编辑

- 三十功名尘与土,八千里路云与月。
×参考诊断
-
本帖最后由 于 2010-05-31 19:52:00 编辑
| 以下是引用海上明月在2010-5-31 18:22:00的发言:
请教:乳晕下几近3cm的囊性肿块,针吸出7ml液体,诊断乳晕下纤维囊性乳腺病是否合适? 大汗腺化生是肯定存在的;细胞簇团的结构和细胞形态没有异型性,所以是良性的,也基本可以考虑;是伴大汗腺化生的囊性增生性病变,还是囊性伴大汗腺化生的肿瘤?有待组织学证实。 |
提得很好。
关于这一例我报告是:考虑为纤维囊性乳腺病合并大汗腺化生,还是稍留有一些余地的。
还有其他的病变,就是散在的顶浆分泌的泡沫细胞,慢性炎性细胞。不仅只是大汗腺化生及形成假乳头样突起的形态表现。
这类纤维囊性乳腺病可能不止一个囊,可能还有微囊及卫星囊存在,也有纤维结构不良表现;它的特殊性在于临床上只表现为“孤立或单纯性囊肿”。
这例关键是能提示它是乳腺的良性增生性病变即可。如果报告导管乳头状瘤是需要接受进一步造影探查,甚至手术探查的。这个部位首要的鉴别诊断就是导管乳头状瘤、派杰氏病,但它们各自都有比较典型的临床特征和镜下形态学特点的。
谢谢。
- 三十功名尘与土,八千里路云与月。
-
本帖最后由 于 2010-05-31 23:05:00 编辑
MBW(马博文)老师的点评(ZT)
同意Rebecca的诊断意见。细胞学为什么会断定囊性?有些网友会这样提出问题,答案是肯定的。虽然没有看到囊壁、囊腔和囊内容物的切面,但要知道细胞学穿刺是由诊断者操作的,因此均为第一手证据性资料。首先得抽出液体,它的颜色、浓稠度、质地等也是参考的重要依据,没有腔隙空间就没有液体,反过来有液体就有腔隙。第二,其中的细胞成分分析,有积液、黏液或渗出就有有细胞反应,最应当见到的就是吞噬细胞,如浆膜腔积液中的泡沫样细胞大部分的“印戒细胞”等,被动或主动灌满了一肚子水,怎会没有空泡?如果是导管渗出,脱落的细胞必定有其表面的上皮细胞,此时的上皮细胞已非原有导管上皮的形态了,细胞的功能或能量系统出现问题了,就是说形态也随之改变,本例中的大汗腺样细胞就是其中之一,是变化而非原有皮肤汗腺细胞,胚胎时期的汗腺内陷形成乳腺的各级导管,早已变为导管上皮细胞。皮肤的汗腺细胞位置要浅表得多。可能会有增生的导管上皮细胞与大汗腺样“化生”细胞,问题来了,它是化生吗?请翻开教科书“化生”的定义,有思考就会有结论,相信诸多老师会有结论的。
在本例的诊断上我个人不主张直接与组织学对应,大致对应就足矣!这样的诊断语言已在本网发表过,就不再重复了。本例诊断为:乳腺导管上皮细胞增生,伴有大汗腺样变和导管扩张。
在鉴别诊断上应当与吞噬细胞鉴别,嗜酸性颗粒样胞质与泡沫样胞质应当能识别。小导管或末梢导管发生的大嗜酸性肿瘤要鉴别,深层部位是基础依据,异性型与单一性是重要依据。
在本例的诊断上我个人不主张直接与组织学对应,大致对应就足矣!这样的诊断语言已在本网发表过,就不再重复了。本例诊断为:乳腺导管上皮细胞增生,伴有大汗腺样变和导管扩张。
在鉴别诊断上应当与吞噬细胞鉴别,嗜酸性颗粒样胞质与泡沫样胞质应当能识别。小导管或末梢导管发生的大嗜酸性肿瘤要鉴别,深层部位是基础依据,异性型与单一性是重要依据。
- 三十功名尘与土,八千里路云与月。
讨论与归纳:
1、乳腺囊肿在临床上多见于两种情况:
1)乳腺乳汁潴留囊肿
2)纤维囊性乳腺病
3、该例解剖位置稍特殊,即在乳晕下的地方。
4、该囊肿与乳腺大导管是不相通的。所以乳头没有溢液临床症状。
5、乳腺导管大汗腺化生常见于良性的慢性纤维囊性乳腺病;当看到大汗腺样化生导管上皮时,首先要考虑到是一种增生性改变的情况。
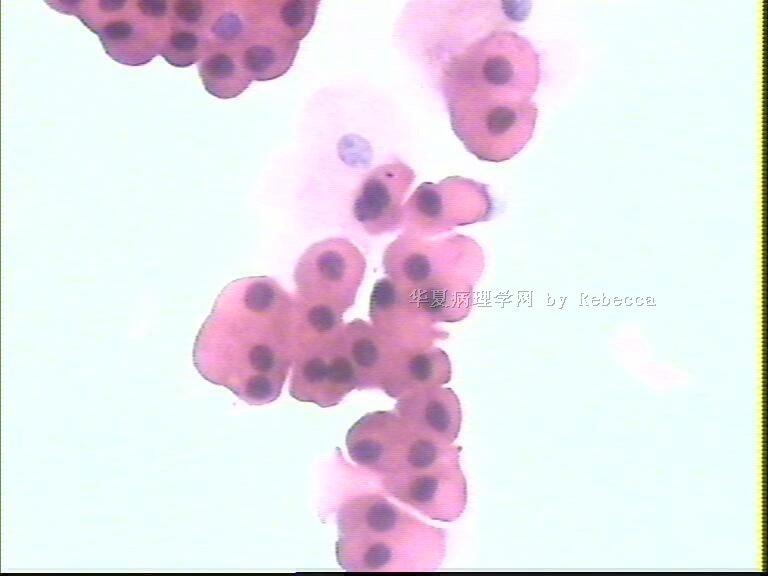
6、大汗腺样变的细胞具有它明显的细胞形态特征,胞浆丰富,嗜酸性染色,透亮,仔细辨认可见胞浆内含丰富细小的分泌空泡;可见活跃的顶浆分泌现象;核通常圆形、类圆形,大小比较一致。相对的低核浆比。
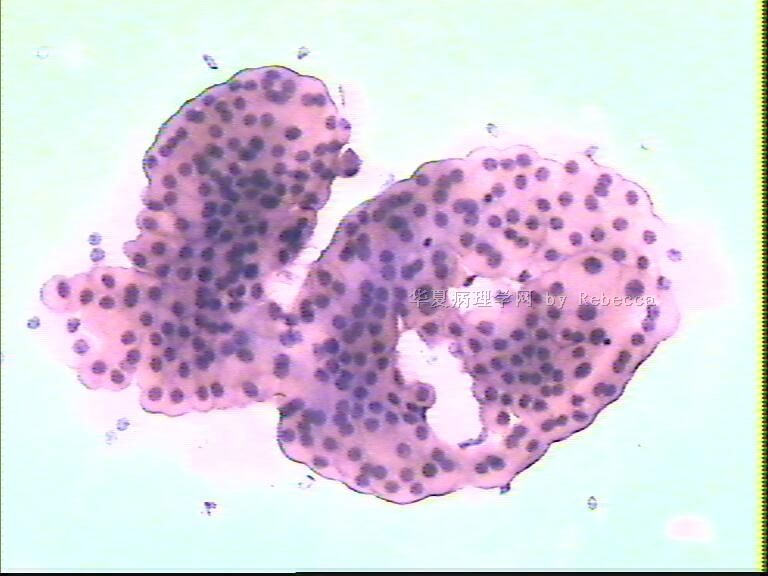
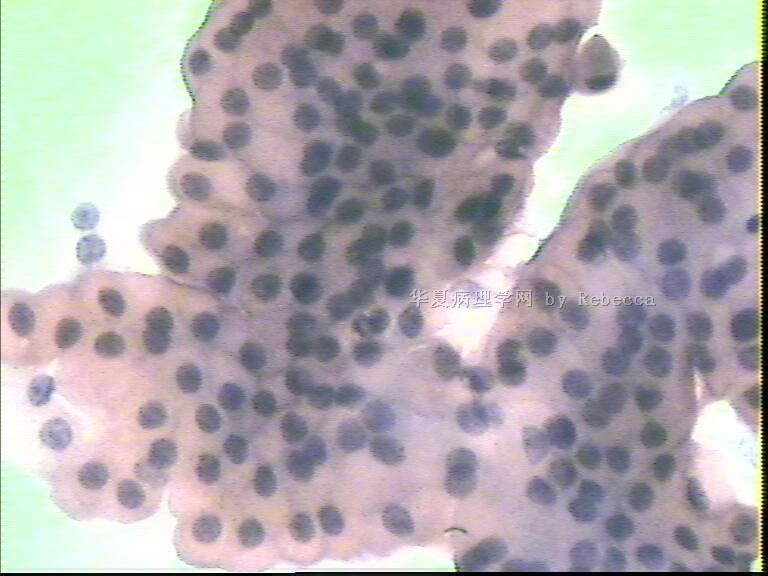
7、在致病因素(可能是荷尔蒙)作用下,大汗腺化生的乳腺导管上皮合成代谢会很旺盛,囊内不断生成的分泌空泡被推向四周胞浆的边缘,以顶浆分泌形式分泌排泄,引起已经堵塞扩张的乳腺终末导管进一步扩张,形成一个囊池。同时大汗腺样化生导管上皮也可以增生,增生突起形成假乳头样结构;它不是一个真性的乳头,没有间质长入,也没有血管作为支架,也看不到肌上皮存在。实际就是大汗腺导管上皮增生突起成一簇状堆积。
此刻,增生的大汗腺化生细胞胞浆浓缩深染,密度增加,细胞变小,胞浆边缘呈圆弧状,平铺时形成花边样外观,当它们簇拥在一起时,便形成了我们看到的“乳头”。
它们之间的边界依然是清晰可辨认的,胞浆依然可看见隐隐约约的分泌小颗粒。我们不难看到本例中从典型的大汗腺样化生细胞移行——>浓缩的花边样细胞过渡,它们是同源性的。
1)乳腺乳汁潴留囊肿
2)纤维囊性乳腺病
3、该例解剖位置稍特殊,即在乳晕下的地方。
4、该囊肿与乳腺大导管是不相通的。所以乳头没有溢液临床症状。
5、乳腺导管大汗腺化生常见于良性的慢性纤维囊性乳腺病;当看到大汗腺样化生导管上皮时,首先要考虑到是一种增生性改变的情况。
6、大汗腺样变的细胞具有它明显的细胞形态特征,胞浆丰富,嗜酸性染色,透亮,仔细辨认可见胞浆内含丰富细小的分泌空泡;可见活跃的顶浆分泌现象;核通常圆形、类圆形,大小比较一致。相对的低核浆比。
7、在致病因素(可能是荷尔蒙)作用下,大汗腺化生的乳腺导管上皮合成代谢会很旺盛,囊内不断生成的分泌空泡被推向四周胞浆的边缘,以顶浆分泌形式分泌排泄,引起已经堵塞扩张的乳腺终末导管进一步扩张,形成一个囊池。同时大汗腺样化生导管上皮也可以增生,增生突起形成假乳头样结构;它不是一个真性的乳头,没有间质长入,也没有血管作为支架,也看不到肌上皮存在。实际就是大汗腺导管上皮增生突起成一簇状堆积。
此刻,增生的大汗腺化生细胞胞浆浓缩深染,密度增加,细胞变小,胞浆边缘呈圆弧状,平铺时形成花边样外观,当它们簇拥在一起时,便形成了我们看到的“乳头”。
它们之间的边界依然是清晰可辨认的,胞浆依然可看见隐隐约约的分泌小颗粒。我们不难看到本例中从典型的大汗腺样化生细胞移行——>浓缩的花边样细胞过渡,它们是同源性的。
- 三十功名尘与土,八千里路云与月。
-
本帖最后由 于 2010-05-29 16:09:00 编辑
cqzhao 老师会诊意见:(ZT)
Interesting case and thank for sharing.
I once did a lot of breast FNA when I was cytofellow at USC where all breast mass lesions would be referred to cytopathologists to do FNA. Now days FNA is rare to be used for the primary evaluation of breast lesions at Magee and most large medical centers in the US. If we do not consider the money, cost-effect, it will be easy for pathologists to read breast core bx than FNA.
For this case I woud like to sign out:
-Negative for maligancy.
-clusters of apocrine cells.
-Suggestive of fibrocystic changes.
Comment:
Mostly it is a lesion with cystic papillary apocrine metaplasia even though the papillary lesion cannot be completely excluded.
FNA combined with clinical impression and imaging finding (Triple test) is highly accurate. If one of the parameters is discordant, surgical biopsy is warranted. Benign Triple test should return for follow up in 3 to 6 months. (write this part in your comment for all FNA breast cases to protect yourself).
In fact 3 cm cystic lesion should be excisioned. Of cause I will not write this sentence in my report. Pathologists do not need to take all the responsblity for patient care. We take care of the part we should have.
http://ipathology.cn/forum/forum_display.asp?keyno=259376
- 三十功名尘与土,八千里路云与月。
-
本帖最后由 于 2010-05-28 22:38:00 编辑
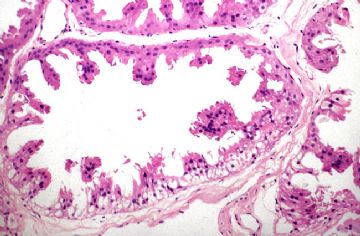 图1
图1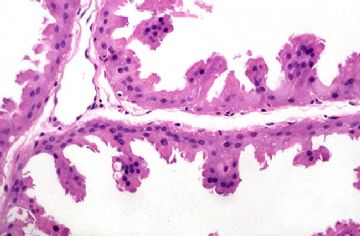 图2
图2
GO ON.
Breast-nonmalignant
Fibrocystic disease
Apocrine metaplasia of breast
Digital Atlas of Breast Pathology by Meenakshi Singh, MD © - Department of Pathology, Stony Brook University Medical Center.
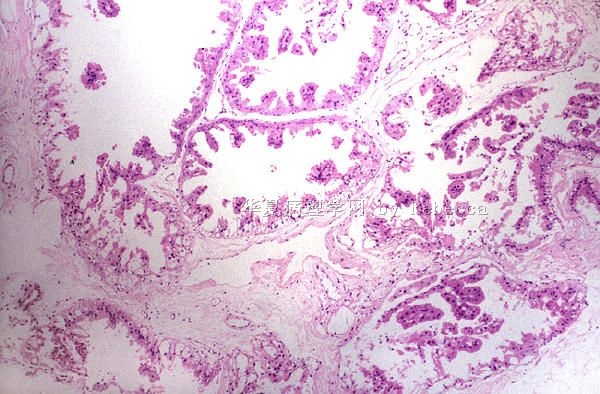
Highly complex papillary apocrine change, high power.
(From PathologyOutlines.com)
- 三十功名尘与土,八千里路云与月。
-
本帖最后由 于 2010-05-28 22:44:00 编辑
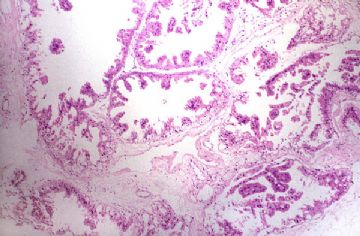 图1
图1
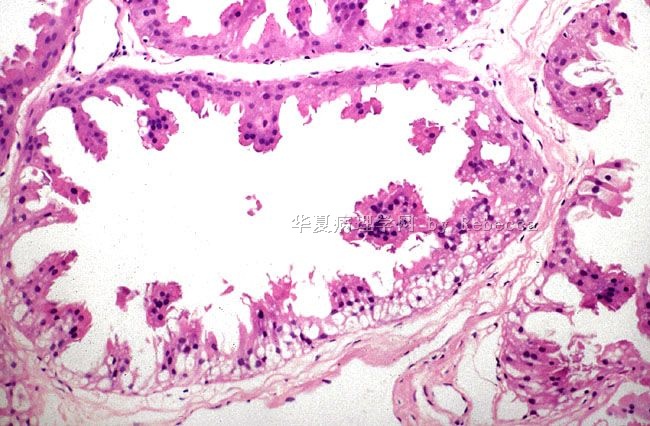
乳腺纤维囊性乳腺病,大汗腺样化生图像
Highly complex papillary apocrine change, low power.
Even at low power, the low nuclear to cytoplasmic ratio is readily apparent along with the uniform cell size and hints of decapitation secretions. The vacuolated cytoplasm and decapitation secretions along with the bland nuclear features are characteristic.
- 三十功名尘与土,八千里路云与月。
-
本帖最后由 于 2010-05-28 22:39:00 编辑
 图1
图1
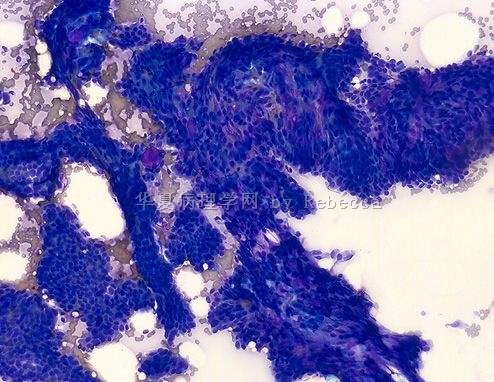
乳腺导管乳头状瘤细胞学图像
Figure 1 :FNA smears show uniform cells with abundant cytoplasm, eccentric nuclei and inconspicuous nucleoli lying in groups and sheets. Apocrine metaplasia is also seen in some areas. (Leishman-Giemsa, x 400)
(From PathologyOutlines.com)
- 三十功名尘与土,八千里路云与月。











