









| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- B2654女/58岁 左乳腺癌 分类?(IHC结果2010-5-3)
| 姓 名: | ××× | 性别: | 年龄: | ||
| 标本名称: | |||||
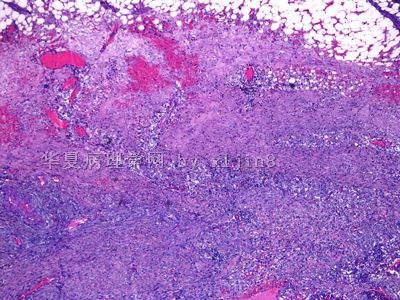
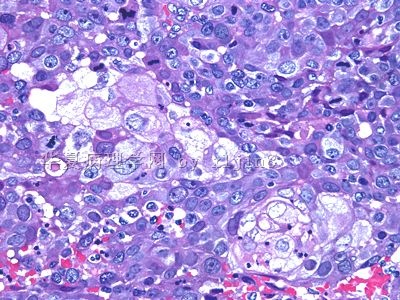
| 简要病史: | 左乳腺肿块8月余,无痛。最近明显增大。 | ||||
| 肉眼检查: | 乳腺组织5.5X5X4.5 CM, 切面见灰白色肿块,直径2.3cm,位于血性囊腔内。 | ||||
图1")
名称:图1
描述:图1
图2")
名称:图2
描述:图2
图3")
名称:图3
描述:图3
图4")
名称:图4
描述:图4
图5")
名称:图5
描述:图5
图6")
名称:图6
描述:图6
图7")
名称:图7
描述:图7
图8")
名称:图8
描述:图8
图9")
名称:图9
描述:图9
图10")
名称:图10
描述:图10
标签:基底细胞样乳腺癌
-
本帖最后由 于 2010-05-03 08:34:00 编辑

- xljin8
×参考诊断
| 以下是引用cqzhao在2010-4-7 11:28:00的发言: My 同事Dr. Bhargava had a study showing CK5 is the most sensitive marker, published in modern Path. However some cases cans till be CK5 negative. This is why we routinely order CK5, ck14, ck17, and EGFR for all triple negative case. |
我看的文献就是他写的
Bhargava R, Beriwal S, McManus K, et al. CK5 is more sensitive than CK5/
为什么BLBC的诊断中一直有EGFR的存在呢?一方面,EGFR并不是基底细胞的标记之一,另一方面,EGFR对于乳腺癌的治疗效果并不明显(Arteaga CL, Truica CI. Challenges in the development of antiepidermal growth factor receptor therapies in breast cancer. Semin Oncol.),我一直很困惑,难道就是因为有一定的阳性率吗?
- The More We See, The Less We Know!
-
本帖最后由 于 2010-05-03 08:32:00 编辑
 图1
图1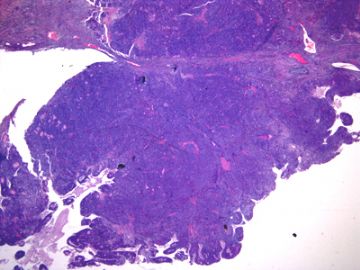 图2
图2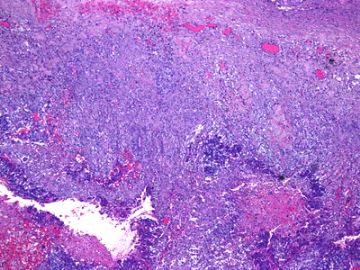 图3
图3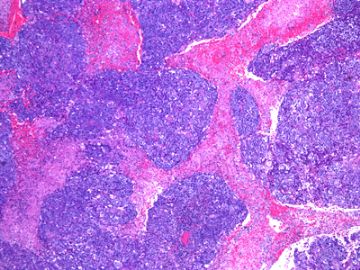 图4
图4 图5
图5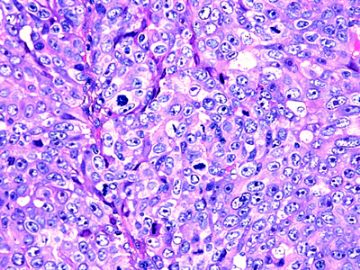 图6
图6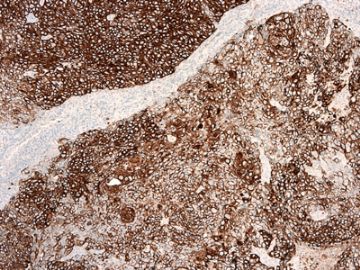 图7
图7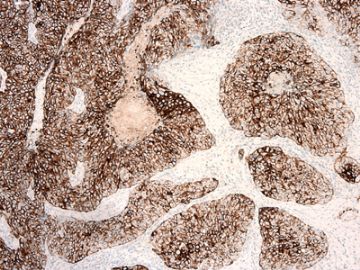 图8
图8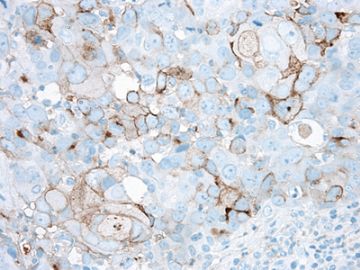 图9
图9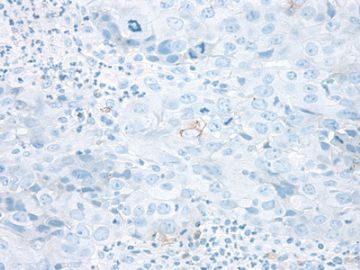 图10
图10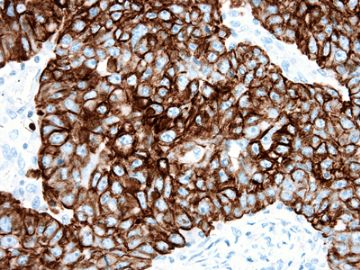 图11
图11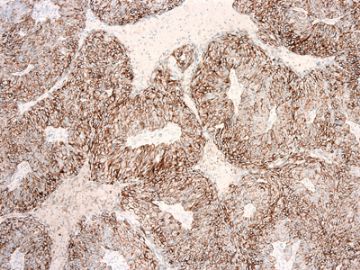 图12
图12 图13
图13 图14
图14 图15
图15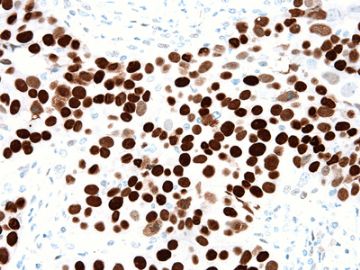 图16
图16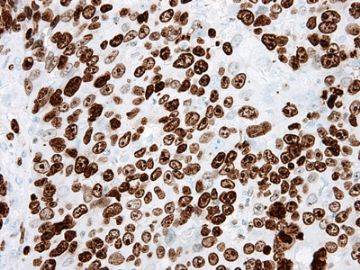 图17
图17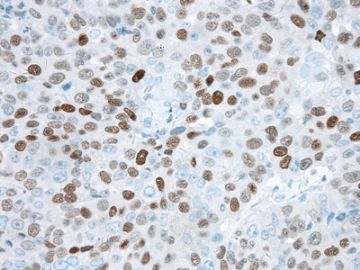 图18
图18
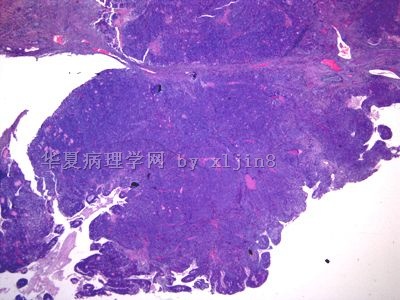
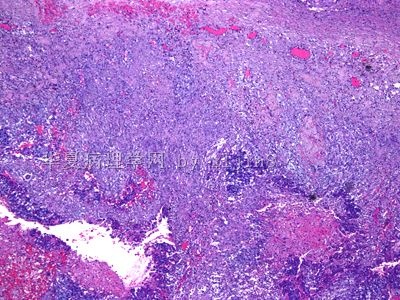
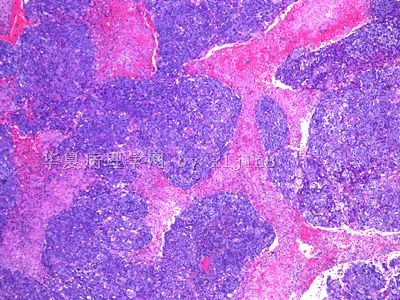
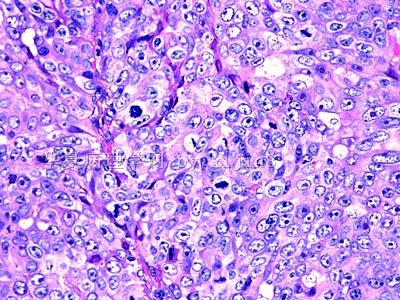
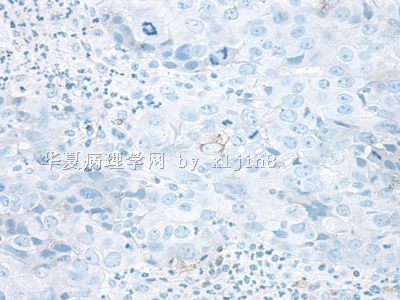
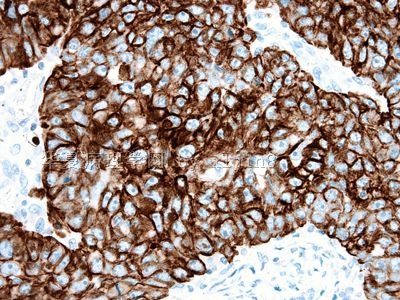
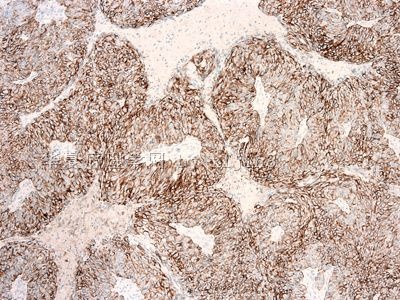
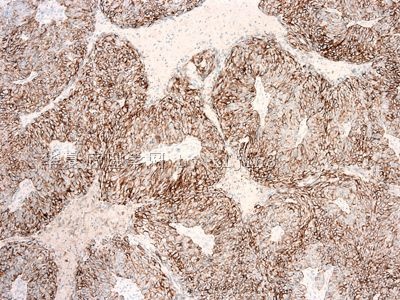
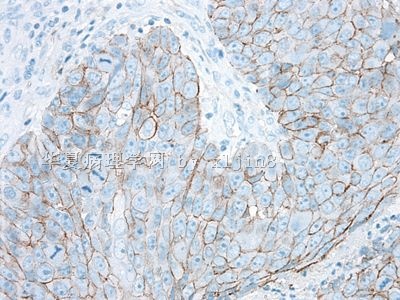
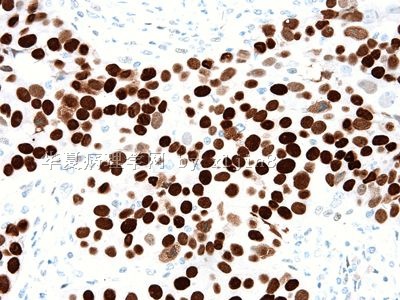
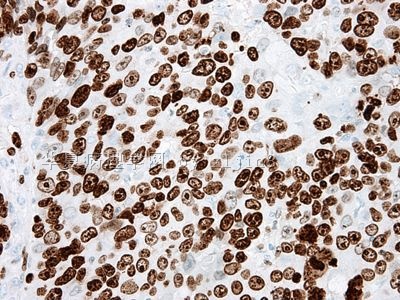
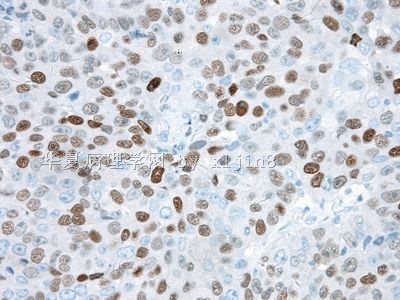
此例是会诊病人。 要求明确是髓样癌还是其他类型癌。IHC标记结果ER-PR-、p63+、SSMHC-、CK5/6-/+34BE12+;目前还在进行标记。照片会尽快上传。谢谢!
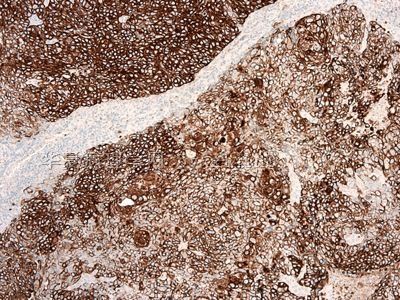
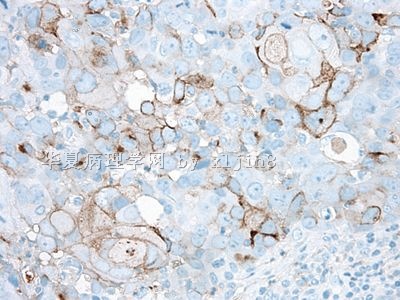
2010-5-3 IHC标记:
图1AE1/AE3;图2 Cam5.2;图3 CD10; 图4 CK5/6;图5 CK7; 图6 CK8;图7 CK18;图8 E-cadherin; 图9 HER2;图10 p53;图11Ki-67, 图12 p63;
- xljin8
| 以下是引用wang4160在2010-5-5 9:04:00的发言:
请教各位老师,基底细胞样癌大家是否已经用在了实际工作中 毕竟这个基因分子分型似乎还不是完全成熟! |
Depend on the comminucation with sugerons and oncologists.They are differenent classsification.
In fact 基底细胞样癌 is a special type of invasive ductal ca. Currently the treatment is similar to other classic type of IDC.
We call them invasive ductal ca with basal-like phenotype.
There are some discussion about 基底细胞样癌 in this link.
http://www.ipathology.com.cn/forum/forum_display.asp?keyno=110426
-
本帖最后由 于 2010-05-07 10:17:00 编辑
| 以下是引用kint123在2010-4-7 19:49:00的发言:
我看的文献就是他写的 Bhargava R, Beriwal S, McManus K, et al. CK5 is more sensitive than CK5/ 为什么BLBC的诊断中一直有EGFR的存在呢?一方面,EGFR并不是基底细胞的标记之一,另一方面,EGFR对于乳腺癌的治疗效果并不明显(Arteaga CL, Truica CI. Challenges in the development of antiepidermal growth factor receptor therapies in breast cancer. Semin Oncol.),我一直很困惑,难道就是因为有一定的阳性率吗? |
Sorry, Just notice your talk.
Several reasons: EGFR was used in the first several basal-like ca papers and also relative % of basal-like ca are positive for EGFR.In addition, Anti-EGFR drugs are potential use for breast ca.
In fact I am not sure the exact reason. You are a thoughtful pathologist.
-
本帖最后由 于 2010-05-07 10:40:00 编辑
P63+, 34BE12+, CK5-, ER-, PR-, Ki67 90%
Her2 equivocal score 2+, need to do FISH Her2..
If Her2 negative, I will call basal-like ca.
Now Her2 score 2. I still think it is a basal-like ca. But it is not a good call based on the difinition. Remember there are a lot of gray zones in medicine.
Do not matter what we call it is a high grade ca. The treatment and prognosis will be the same whatever we call.
If it is my case I will call invasive ductal carcinoma, histologic grading 3 (tubual formation-3, nuclear atypia-3, mitotic activity-3; total score 9/9).
I will not call medullary ca for this case because the infiltrating margins and cytomorphology of the tumor.
Just for reference
Do not matter what we call it is a high grade ca. The treatment and prognosis will be the same whatever we call.
If it is my case I will call invasive ductal carcinoma, histologic grading 3 (tubual formation-3, nuclear atypia-3, mitotic activity-3; total score 9/9).
I will not call medullary ca for this case because the infiltrating margins and cytomorphology of the tumor.
太精彩了,Zhao老师您太棒了,我好崇拜您哦!
- 老林











