
图1")
图2")
图3")
图4")
图5")
图6")

| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- 右上纵膈肿块(中-日-澳2009墨尔本病理读片会病例1)
-
本帖最后由 于 2010-01-21 01:13:00 编辑
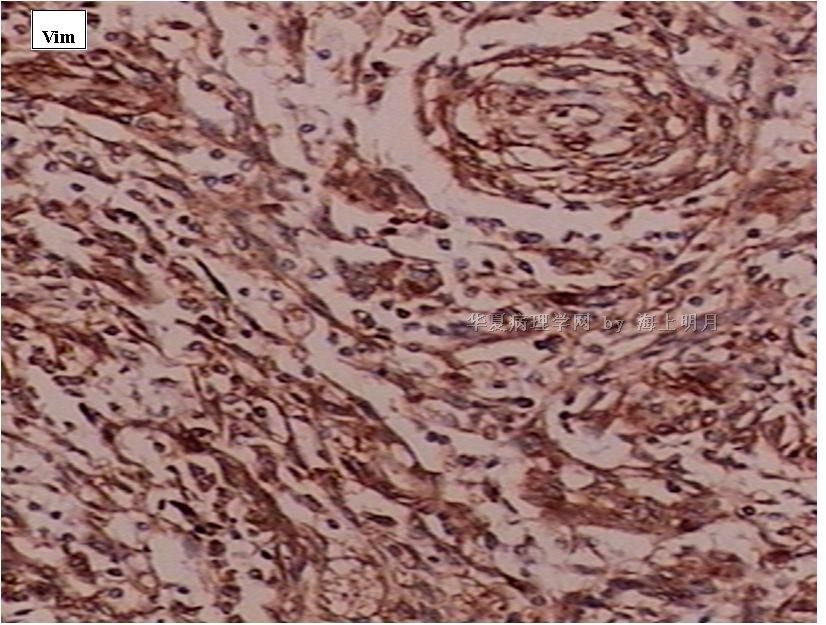
异位脑膜瘤可见于鼻腔、鼻窦、中耳、颈部、皮肤、骨内(尤其是颅骨与颜面部),甚至罕见于纵膈、肺和血管内。有报道在神经鞘膜的同时发生异位脑膜瘤(ectopic meningioma)。
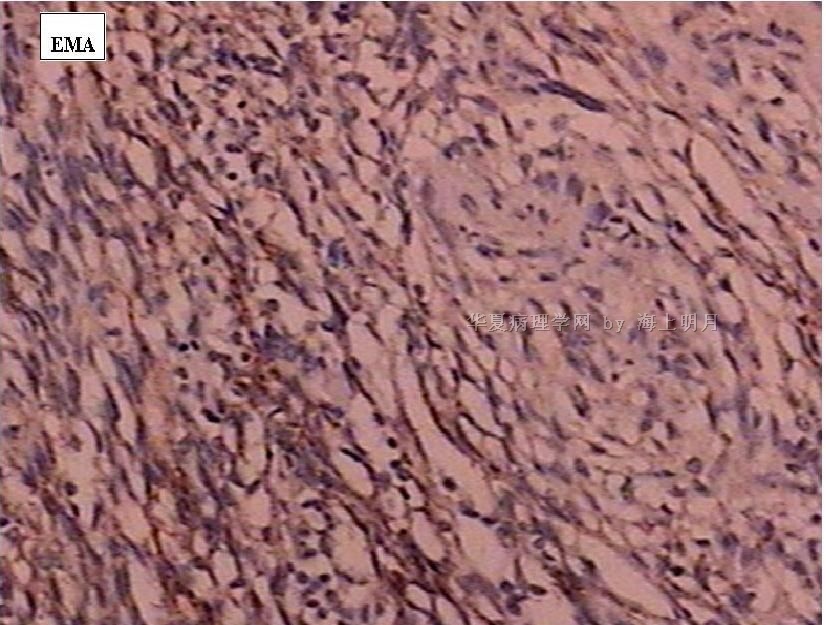
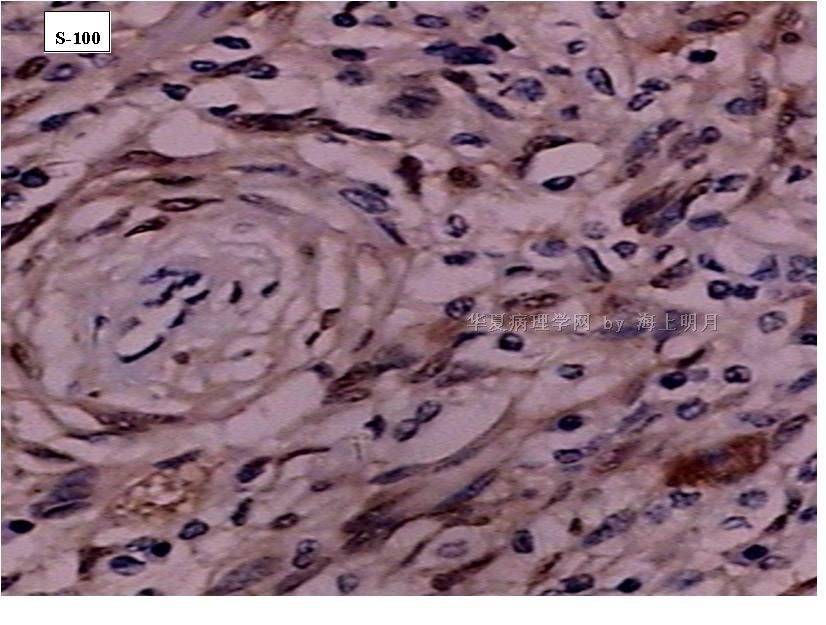
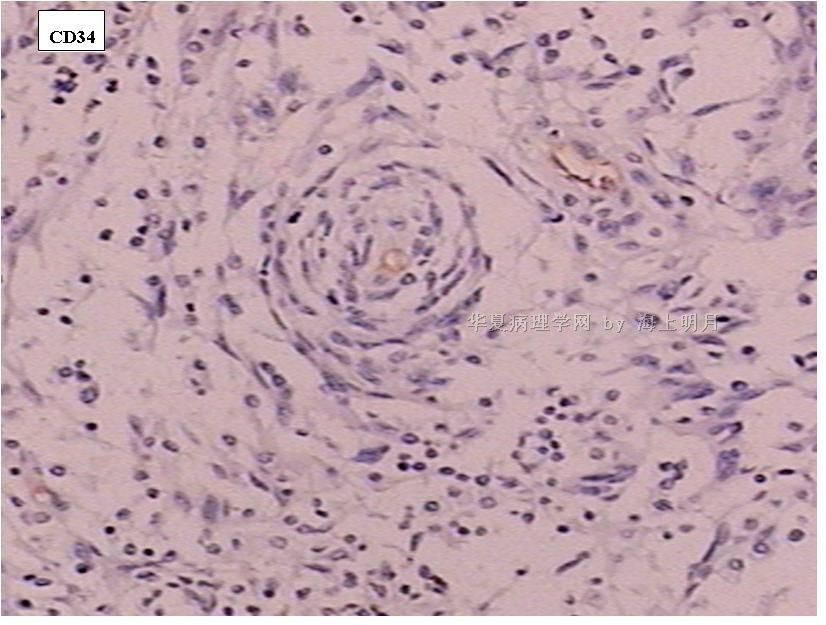
注意要与神经鞘膜瘤(及其神经束膜瘤,S-100一般为阴性)、纤维组织细胞瘤、树突细胞肿瘤、A型胸腺瘤、促纤维增生恶性黑色素瘤和SFT等良恶性肿瘤鉴别。
需注意核分裂计数和肿瘤性坏死以及肿瘤周围浸润情况,以除外恶性。IHC标记可资辅助鉴别诊断。
本例的大体标本和影像显示有局部囊性变和出血。有文献报道,异位脑膜瘤可以因囊变而出血为首发症状。

- 王军臣
J Neurooncol. 1996 Sep;29(3):217-21.
Pathology of meningiomas.
University of Texas M.D. Anderson Cancer Center, Division of Pathology (Neuropathology), Houston, USA.
Because meningiomas arise from arachnoid cells present in the meninges, they can occur in any location where meninges or ectopic meninges exist, such as the nasal cavity, the paranasal sinuses, the middle ear, and even the mediastinum. Although the tumors may range in appearance from epithelial to mesenchymal, they are characterized by a uniform distribution of cells with shapes ranging from polygonal epithelial-like to spindled and fusiform. Historically, classification of meningiomas has been based upon cell shapes, cell patterns, cell products, or stroma, implying clinicopathologic differences among the types. Numerous observations have shown that certain conditions may indicate a predisposition for developing meningiomas, prompting extensive studies of meningiomas using cytogenetic techniques. Meningiomas are common neoplasms arising from the central nervous system meninges. They are important because of the morbidity they produce. Their critical intracranial and intraspinal locations make diagnosis and surgical removal difficult.
- 王军臣
-
本帖最后由 于 2010-01-20 17:42:00 编辑
以下是陈博士所说的那篇文章的摘要.
Am J Surg Pathol. 2005 Jul;29(7):845-58.
Soft tissue perineurioma: clinicopathologic analysis of 81 cases including those with atypical histologic features.
Department of Pathology, Brigham and Women's Hospital, and Harvard Medical School, Boston, MA 02115, USA.
Perineuriomas are uncommon benign peripheral nerve sheath tumors that include soft tissue, sclerosing, and intraneural variants. Fewer than 50 soft tissue perineuriomas have been reported to date, and the clinical significance of atypical histologic features is unknown. To characterize these tumors further, 81 soft tissue perineuriomas received between 1994 and 2003 were retrieved from the authors' consult files. Hematoxylin and eosin sections were reexamined, immunohistochemistry was performed, and clinical details were obtained from referring physicians. Forty-three patients were female and 38 male (mean age, 46 years; range, 10-79 years). Tumor size ranged from 0.3 to 20 cm (mean, 4.1 cm) in greatest dimension. Most patients presented with a painless mass. The tumors arose in a wide anatomic distribution: 36 lower limb, 19 upper limb, 15 trunk, 7 head and neck, 3 retroperitoneum, and 1 paratesticular. Forty-two tumors were situated primarily in subcutis, 25 in deep soft tissue, and 9 were limited to the dermis. Nearly all cases were grossly well circumscribed; 12 showed focal microscopically infiltrative margins. Most tumors had a storiform and focally whorled growth pattern; 17 exhibited fascicular areas. Thirty-eight tumors were hypocellular, 15 were markedly hypercellular, and 7 showed alternating zones of hypocellularity and hypercellularity. Stroma was usually collagenous but in 17 tumors was predominantly myxoid, and in 16 was mixed collagenous and myxoid. Mitoses ranged from 0 to 13 per 30 high power fields (mean, 1); 53 tumors had no mitoses. Based on worrisome cytologic or architectural features, 14 cases were classified as atypical perineuriomas: 12 contained scattered pleomorphic cells, 1 showed an abrupt transition from typical morphology to a markedly hypercellular, fascicular area with cytologic atypia, and 1 exhibited diffuse infiltration of skeletal muscle. All tumors were reactive for epithelial membrane antigen; 50 of 78 (64%) expressed CD34, 22 of 76 (29%) claudin-1, 16 of 77 (21%) smooth muscle actin, and 4 of 81 (5%) S-100 protein. All tumors were negative for glial fibrillary acidic protein, neurofilament protein, and desmin. Clinical follow-up was available for 43 patients (mean, 41 months; range, 6-146 months). Among tumors for which the status of surgical margins was known, 52% were widely excised, 31% were marginally excised, and 18% had positive margins. Only two tumors recurred locally (one of which was atypical): one recurred 10 years following primary excision; and one recurred twice, 5 and 9 years following excision. No tumor metastasized. Soft tissue perineuriomas behave in a benign fashion and rarely recur. Atypical histologic features (including scattered pleomorphic cells and infiltrative margins) seem to have no clinical significance and appear to be akin to those seen in ancient schwannoma and atypical (bizarre) neurofibroma.
- 王军臣











