






| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- Inguinal lymphadenopathy
-
panzenggang 离线
- 帖子:189
- 粉蓝豆:480
- 经验:246
- 注册时间:2008-01-09
- 加关注 | 发消息
| 姓 名: | ××× | 性别: | Male | 年龄: | 70 years |
| 标本名称: | Inguinal lymph node | ||||
| 简要病史: | 70-year-old male, multiple inguinal lymphadenopathies with largest one up to 2.0 cm. No other clinial abnormalities. | ||||
| 肉眼检查: | Needle biopsy of inguinal lymph node. | ||||

名称:图1
描述:图1

名称:图2
描述:图2

名称:图3
描述:图3

名称:图4
描述:图4
标签:
×参考诊断
-
本帖最后由 于 2009-12-11 16:25:00 编辑
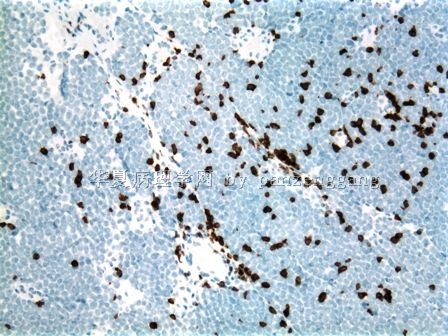
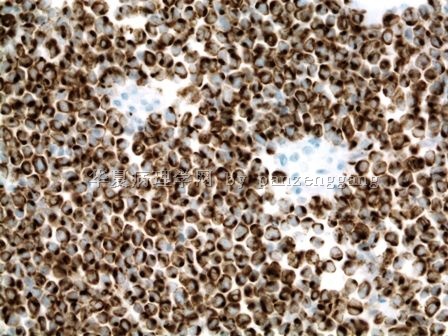
HE形态特点:淋巴结结构破坏,单一性小-中淋巴细胞增生,隐约结节状,较多厚壁小血管,无淡然的增殖中心,无星空现象,无中心母细胞(未给高倍镜示细胞核的细节和核分裂活性)。第4张图右下角有些细胞质略多,透明。临床特点老年人,多处淋巴结肿大。非常同意 Dr. Arhus 的诊断意见。我把套细胞淋巴瘤放在首位。 其他要除外毛细胞白血病,单核样B细胞淋巴瘤,前淋巴细胞白血病。标记抗体可选择:CD20, CD5, CD10, CD3, CD56, Cyclin D1, CD23 CD25,DBA 44,IgD, MIB-1。

- xljin8
-
panzenggang 离线
- 帖子:189
- 粉蓝豆:480
- 经验:246
- 注册时间:2008-01-09
- 加关注 | 发消息
| 以下是引用panzenggang在2009-12-12 11:24:00的发言: Somebody please tell me how to add the pictures in the reply. The tumor is negative for CD3, CD5, CD20 and CD79a, except scattered reactive lymphocytes. The last picture is 40x. 您可以通过选择编辑,然后用插入新图片的方式试一下。 这可能不是规范的方法,但是我是这样插入图片的。 |
- xljin8
-
除了Dr. Arhus 的 建议外,我还想到1)浆细胞瘤(要标记:CD138, VS38C,Bob-1,Oct-2;2) T/NK NHL(标记LCA, CD56),3)髓系肿瘤(标记MPO,PGM1,CD34)此外,老年人要考虑其它 4)小细胞恶性肿瘤,如转移性小细胞癌,AE1/AE3, EMA, Cam 5.2,MIB-1,TTF-1,包括(Merkel cell carcinoma - CK20+)。
此外,能否重染HE,上述高倍图片苏木精染色太深,肿瘤细胞核的细节无法辨认清楚。
- xljin8
-
panzenggang 离线
- 帖子:189
- 粉蓝豆:480
- 经验:246
- 注册时间:2008-01-09
- 加关注 | 发消息
-
本帖最后由 于 2009-12-13 15:37:00 编辑
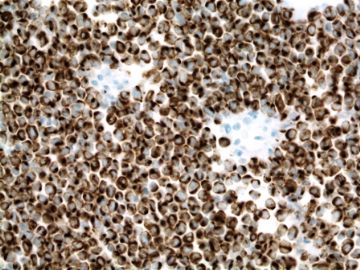 图1
图1
(Sorry I cannot type Chinese, and I can’t install Chinese since my Department gave me the computer during residency training)
The HE stain was OK.
Actually when I first saw this case, I had the same question: why the staining is so dark and weird? The nuclei are so dark and uniform, almost like ground glass pattern. could that be due to fixation or other artifact? Probably not, since it was a small needle biopsy and should be very easy to fix, and I did not see any signs of artifact. Anyway, the nuclei are really dark with very homogeneously fine chromatin.
Dr. XLJin8 gave very good differential diagnoses. However, we can probably rule out several of them just based on HE:
1). Plasma cell myeloma: larger cells with more cytoplasm and more clumped chromatin;
2). T/NK: moderate clear cytoplasm, and more irregular nuclei, classic vascular proliferation with inflammatory cells in the background.
3). Myeloid tumor: medium to large cells with some cytoplasm depending upon the stage of differentiation, but the chromatin should be very open with prominent nucleoli if in the blast stage, or should show some evidence of differentiation if in other stage.
4). Small round blue cell tumor: most likely, but again there are several entities, including small cell carcinoma of the lung, PNET, ALL, and small cell melanoma. But what most puzzled me was the nuclei: dark and homogeneous, more fine than "salt and pepper".
This case was showed in our Department QA meeting. My attending showed us the CD3 and CD79a first. When I saw both stainings were negative, I suddenly thought of a tumor with this kind of dark and fine chromatin, except the fact that it may have organoid growth pattern which didn't show in this lymph node. I asked her: do you have CK20? She was very surprised. Actually, at the time, I just started collecting the cases of "metastatic tumors in the lymph node mimicing lymphomas", and it was not surprising that I had this idea.
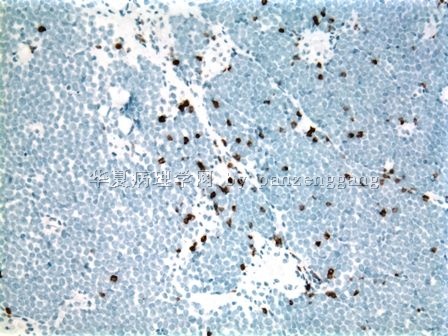
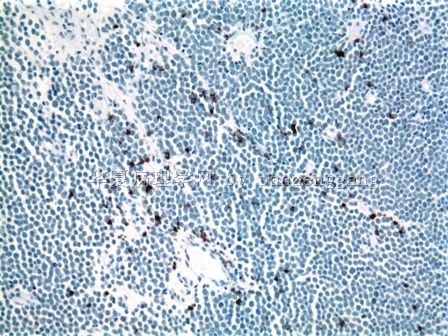
IPX: CK 20+ , as shown below. He had no skin lesion.
-
本帖最后由 于 2009-12-13 22:08:00 编辑
| 以下是引用panzenggang在2009-12-13 15:35:00的发言: (Sorry I cannot type Chinese, and I can’t install Chinese since my Department gave me the computer during residency training)
The HE stain was OK.
Actually when I first saw this case, I had the same question: why the staining is so dark and weird? The nuclei are so dark and uniform, almost like ground glass pattern. could that be due to fixation or other artifact? Probably not, since it was a small needle biopsy and should be very easy to fix, and I did not see any signs of artifact. Anyway, the nuclei are really dark with very homogeneously fine chromatin.
Dr. XLJin8 gave very good differential diagnoses. However, we can probably rule out several of them just based on HE: 1). Plasma cell myeloma: larger cells with more cytoplasm and more clumped chromatin; 2). T/NK: moderate clear cytoplasm, and more irregular nuclei, classic vascular proliferation with inflammatory cells in the background. 3). Myeloid tumor: medium to large cells with some cytoplasm depending upon the stage of differentiation, but the chromatin should be very open with prominent nucleoli if in the blast stage, or should show some evidence of differentiation if in other stage. 4). Small round blue cell tumor: most likely, but again there are several entities, including small cell carcinoma of the lung, PNET, ALL, and small cell melanoma. But what most puzzled me was the nuclei: dark and homogeneous, more fine than "salt and pepper". This case was showed in our Department QA meeting. My attending showed us the CD3 and CD79a first. When I saw both stainings were negative, I suddenly thought of a tumor with this kind of dark and fine chromatin, except the fact that it may have organoid growth pattern which didn't show in this lymph node. I asked her: do you have CK20? She was very surprised. Actually, at the time, I just started collecting the cases of "metastatic tumors in the lymph node mimicing lymphomas", and it was not surprising that I had this idea.
IPX: CK 20+ , as shown below. He had no skin lesion. (为了使更多的年轻医师能参与讨论,将此译为中文。不对之处请Dr. Pan 纠正,谢谢!) 抱歉,不能用中文,因为我使用的是部门给住院医师训练期用的电脑,不允许安装中文软件。 HE染色并没有问题。 实际上我第一次看到此病例的切片也有同样的疑问,染色为什么这样深和奇特?细胞核染色如此之深和均匀,几乎就像毛玻璃。难道是由于固定或其他人为因素造成的?不可能,因为它是穿刺标本,应该很容易固定,再说也未看到任何其他人为因素造成的改变。不去管它,反正细胞核染色很深,染色质非常细小和均匀。 XLJIN8 列出很好的鉴别诊断,但是,通过HE形态就能排除其中的几种疾病。 1)浆细胞性骨髓瘤 细胞应该更大,细胞质更多,染色质应该粗大成簇。 2)T/NK细胞淋巴瘤 应该有中等量的细胞质,核更不规则,背景中应该存在典型的血管改变和炎症细胞。 3)髓细胞肿瘤 如果是母细胞阶段,肿瘤细胞总有一些与分化相应的细胞质改变,染色质很空,有明显的核仁。如果是处于分化的其他阶段,细胞必然会表现出某些分化的证据。 4)小圆形蓝细胞肿瘤 此例最为可能。但是仍有几种疾病需要鉴别,包括肺小细胞癌、PNET、急性淋巴细胞性白血病、小细胞性恶性黑色素瘤。然而,使我最为迷惑的是肿瘤细胞核的深染和如此的一致性,染色质要比“盐和胡椒粉”更加的细小。 此病例是我们部门在质量保障(QA)会上展示的。我的主治医师先让我看了CD3 和CD79a的免疫组化标记片,当我看到二者均不表达时突然想的一种具有这样核深染和染色质细小的肿瘤,除了这个淋巴结内的病变没有显示出器官样结构外。我问她,你是否标记了CK20 ?她非常吃惊。 实际上,在那时候,我正在开始收集“类似淋巴瘤的淋巴结转移性癌”。 这样她就不会奇怪为什么我会想到Merkel细胞癌。 免疫组化标记CK20+(图示)。患者没有皮肤病变。
|
- xljin8
-
panzenggang 离线
- 帖子:189
- 粉蓝豆:480
- 经验:246
- 注册时间:2008-01-09
- 加关注 | 发消息
-
本帖最后由 于 2009-12-23 10:44:00 编辑
-
Diagnosis: metastatic Merkel cell carcinoma.
-
Microscopic description: The tumor consists of monotonous, small, round and blue cells with very high N/C ratio and evenly dispersed chromatin. The nucleolus is inconspicuous. The tumor cells are dyscohesive with focal vaguely nodular pattern. Abundant mitotic figures are present.
-
Differential diagnosis:
-
T-ALL: young age, mediastinal mass, TdT+, CD3+.
-
B-ALL: young age, more common as leukemia form, TdT+, CD10+, CD20+.
-
Metastatic small cell carcinoma for the lung: CK20-, CK5/6+, TTF+ (50%), CEA+/-.
-
Small cell melanoma: S100+, MITF+. MART1+, HMB45+, CK20-.
-
PNET: CD99+, Vimentin+, CK20-.
-
Merkel cell carcinoma: CK20+, CK5/6-, p63-, TTF1-, CEA-, S100-, vimentin-, CD45-, CD117+, Synaptophysin+, chromogranin A+.
-
-
Tumor
PanCK CK20 CK5/6 P63 TTF1 CD99 CEA S100 Melan-A
Vimentin CD45
Merkel cell carcinoma + + - - - +/- - - - - - Metastatic small cell carcinoma (lung) + - - - + +/- +/- - - - - Small cell squamous carcinoma + - + + - - - - - +/- - Small cell eccrine carcinoma + - - - - - +/- +/- - +/- - Small cell melanoma - - - - - +/- - + + + - Primitive neuroectodermal tumor +/- - - - - + - - - + - Non-Hodgkin's Lymphoma - - - - - +/- - - - +/- +
|
Summarized by Zenggang Pan, MD, PhD For more detail, please visit: http://www.enjoypath.com/hp/hp-073/hp-073.htm |











