






| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
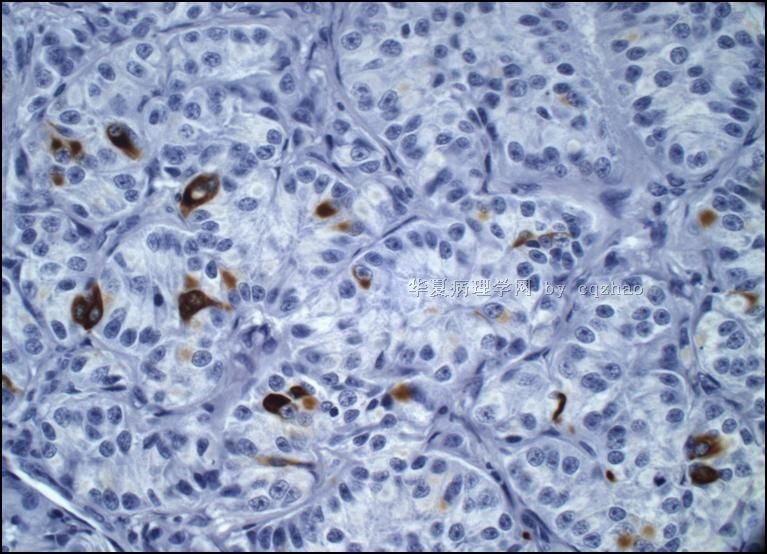
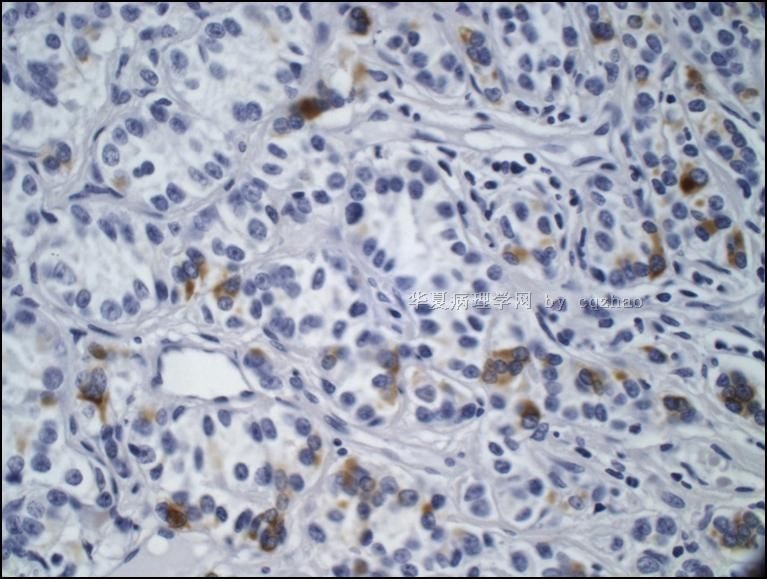
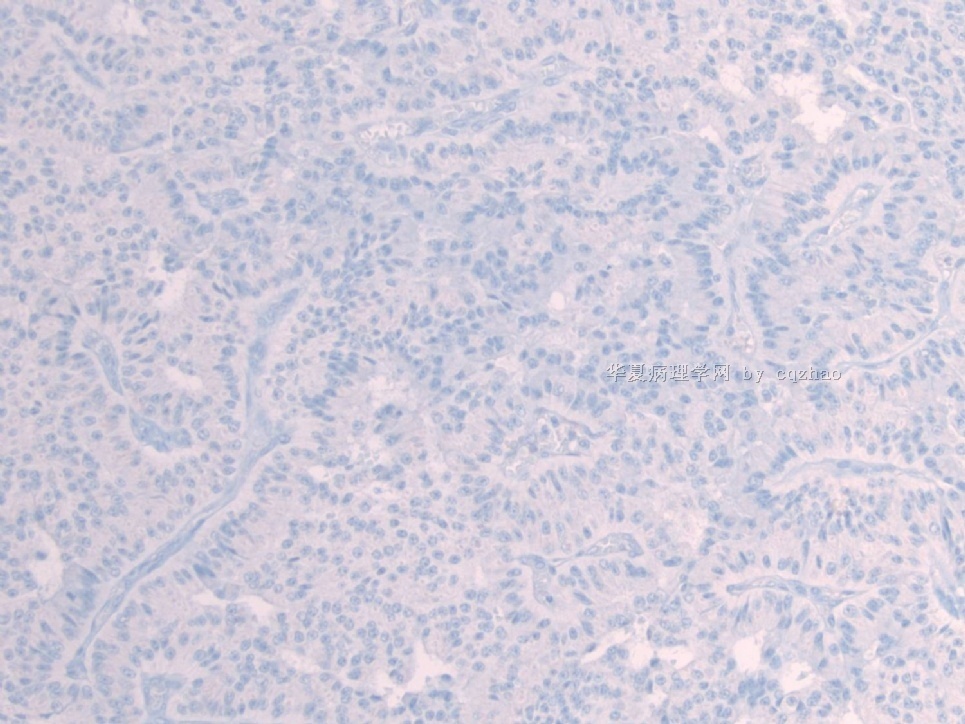
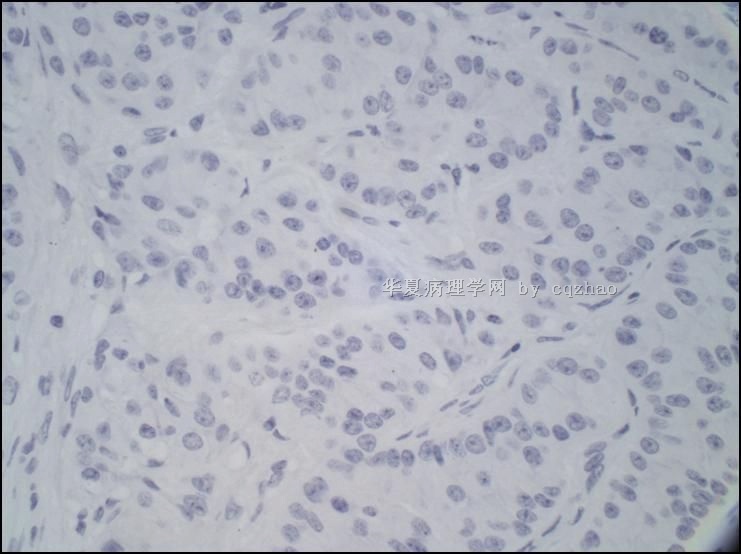
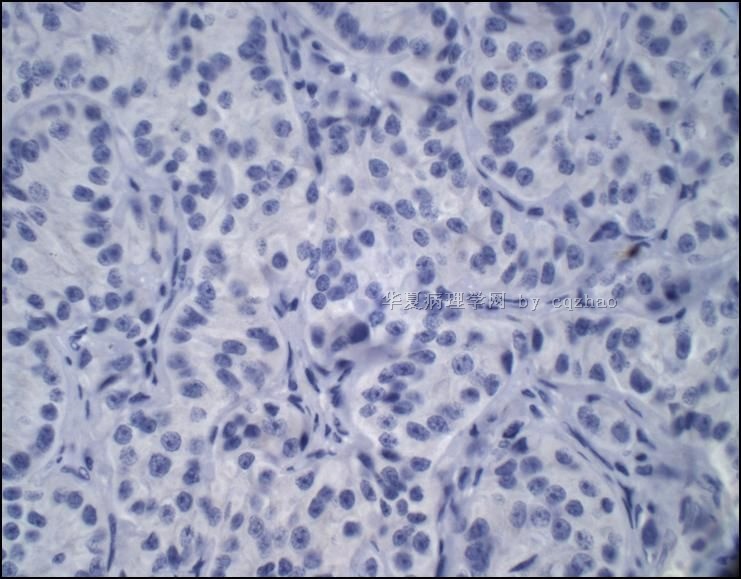
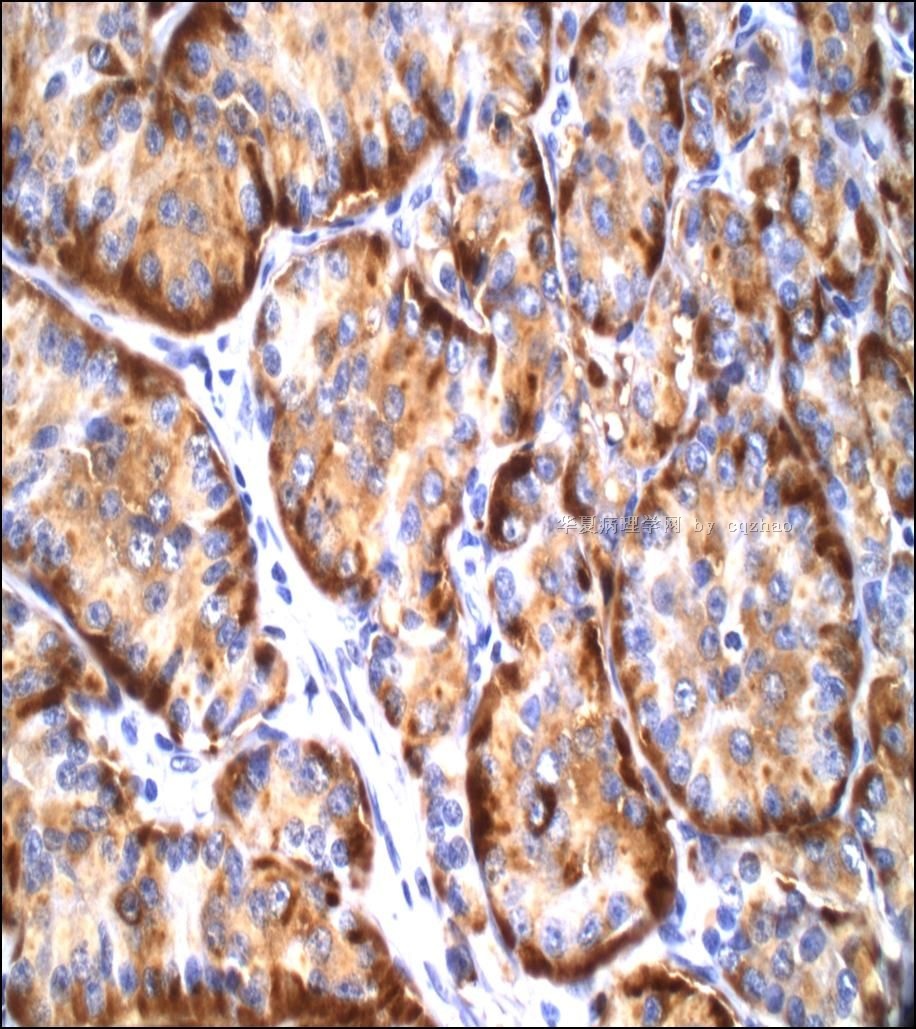
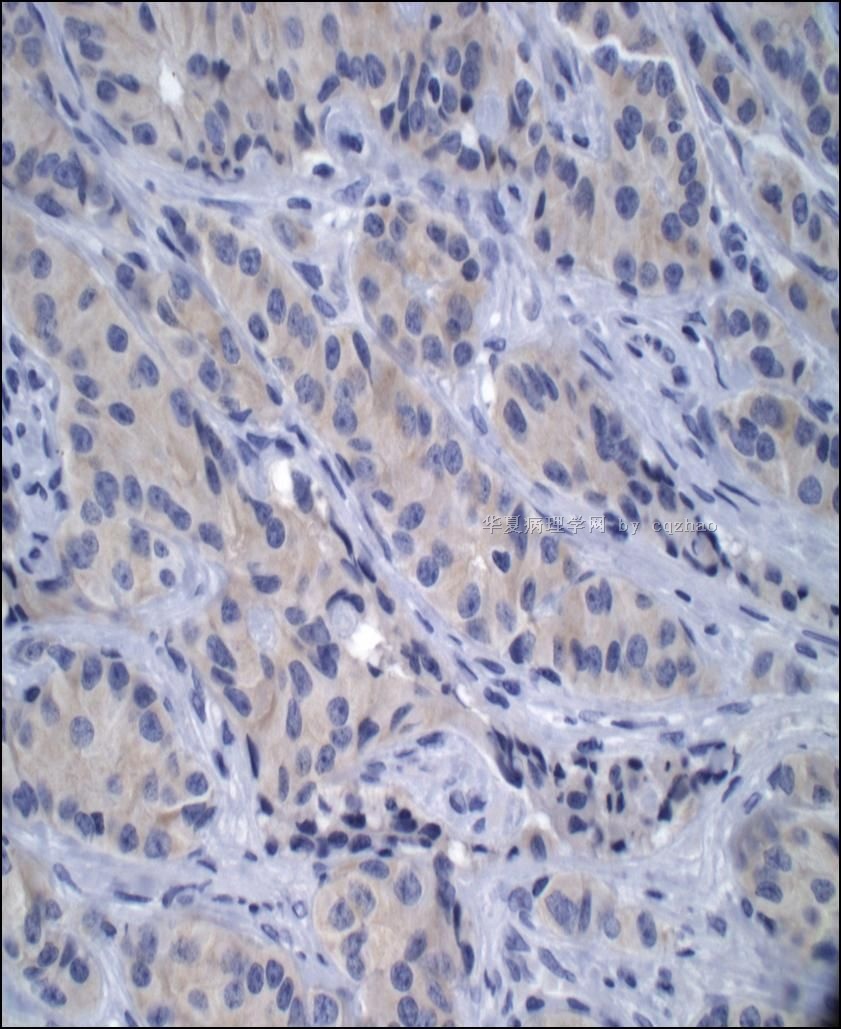
- 形态学难以诊断的卵巢类癌
57 y AA women/L ov mass 8x6x4 cm. This is the AFIP case in Jan 1974. Dr. Henry J Nosrr was Chair of Gynecology/breast Department at AFIP. He and his colleques reviewed the case, and also sent the case to MGH for second oppinion. The case was reviewed by Dr. Robert E. Scully and Dr. Stanley J. Robboy. I found the case in 2004 for immunostain research of ovarian sex cord stroma tumors and noticed their original interpretation for this case.Remember that there were no immuno atains in 1974. They had different oppinion and no final conclusion about this case.
I would like to share this case with our Chinese pathologists.
1. Know how difficult for some cases if there is no immunostain
2. To learn the concept of these world leading pathologists.
3. Hope our patholgoists know these greast pathologists. Welcome some ones to write some brief introduction for these pathologists,Robert E. Scully, Henry J Nosrr, Stanley J. Robboy. All of them are alive
4. Try yourself and you may have a better diagnosis than these experts. Ha, ha.
cz
标签:
-
本帖最后由 于 2010-06-09 23:19:00 编辑
×参考诊断
-
本帖最后由 于 2009-11-03 03:36:00 编辑
Dr. Norris: Final Long Letter to Contributor pathologist (March. 21, 1974).( I copied parts to you)
-In talking to these fellows at a meeting last week, I took the position that the lesion might be a carcinoid, and they got rather upset. They hold their view strongly the lesion is a SCT.
-I think we should keep the diagnosis open and see if we definitely resolve with time whether or not the lesion is a SCT or carcinoid
cz:
At that time, Dr. Norris though mostly it was an carcinoid case. However most pathologists in the gynecologic department at AFIP were agaist him.
I once showed the case in a talk at UPMC 1n 2006. Austin, who worked three years at AFIP with Dr. Norris in the late of 1980s, told the story to Norris. Norris sent an email back with a good humor " finally I made one case correctly after 32 years"
The purpose I showed this case is to demonstrate the ovarian sex cord tumor is a large family of tumors exhibiting varying degrees of differeentiationa and pathologic features. Some cases are difficult to make the dx for pathologists, even for the expert pathologists. The importance is that you should have the differnetial diagnoses and some basic knowledge of immunostains.
This cases is here for a long time. Thank above interpretaion.
Dr. Norris at AFIP signed the case originally in January 14, 1974. His differential diagnosis included sertoli cell tumor (SCT) and carcinoid, but he favorred carcinoid. He had a long discussion in his report. Also the case was discussed in department conference.
Dr. Norris is an excellent gyn/breast pathologist and worked for about 30 years in gyn/breast department at AFIP and was the Chair of the department for many years(longest chair in the department). He did a lot of important research in the areas of gyn/breast pathology. Dr. Kurman once worked at AFIP and was Dr. Norris's staff pathologist for a few years in the late 1970th. In the early 1990 he retired from AFIP and Worked in a group in Florida. Tavassoli became the Chair after Dr. Norris retired from AFIP. Now Dr. Norris completely retired and enjoys his life in Florida.
Do you agree with Dr. Norris's interpretation for this case?
Dr. Henry J Nosrr , Dr. Robert E. Scully and Dr. Stanley J. Robboy.
我知道一些,他们都是顶级妇科病理专家,尤其崇敬Scully
我基本同意fangg:环状小管性索肿瘤。
但是Dr.zhao说了,主要结构是前三张图,那么修正一下诊断:Sertoli细胞瘤,部分伴有环状小管结构。
鉴别诊断如Dr.Young以前的一篇经典文献中所述,在此从略。

华夏病理/粉蓝医疗
为基层医院病理科提供全面解决方案,
努力让人人享有便捷准确可靠的病理诊断服务。
-
本帖最后由 于 2009-11-03 03:37:00 编辑
Dr. Stanley J. Robboy (carcinoid expert) currently is at Duke and is the president of CAP from this month for one year.
He was at MGH at that time. He reviewed the case and wrote the report:
I have looked at the seven EM photos and believe that the granules differ from those in carcinoid.
cz:
Basically he did not think it was carcinoid.











