
图1")
图2")






| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- 外阴Paget病和EMPD简要总结介绍(cqz-2)
赵老师发起帖子来够吓人
谢谢分享这样的好病例。看了下很有启发,不一一翻译。
学生不才,最近刚刚写了篇文章中涉及到外阴,这里秀一下,希望对网友们能有点启发
Paget病 外阴是除乳腺外Paget病最常见的发生部位,大多数外阴Paget病是原发性的,但有5%是其它部位恶性病变(如膀胱尿路上皮癌、宫颈腺癌或结直肠腺癌等)的局部表现,此时外阴Paget病代表着这些恶性肿瘤的上皮内转移或扩散性病灶,因此辨别外阴Paget病是原发还是继发对临床治疗非常重要。多数研究证实原发性外阴Paget病的Paget细胞表达CK7、CEA和CAM5.2,大多数表达 GCDFP-15、HER-2和AR,ER和PR表达阴性。而来自于结直肠和和膀胱恶性肿瘤的外阴继发性Paget病通常表达该部位腺癌的免疫标记,如CK20、CDX2和MUC2阳性提示结直肠来源,而CK20和uroplakin Ⅲ阳性则为膀胱腺癌来源。最近有研究发现p63在外阴原发性Paget病与继发于膀胱尿路上皮癌的Paget病的鉴别诊断中具有价值,前者表达阴性,而后者表达阳性[8]。恶性黑色素瘤和外阴上皮内肿瘤(VIN)有时可有Paget样组织学构型,此时易误诊为外阴Paget病,但恶性黑色素瘤表达HMB45和S-100蛋白,而不表达CK7、CEA和GCDFP-15,Paget样VIN(Paget样鲍温病)CK7表达阴性。值得注意的是,正常皮肤内可含有CK7和CK20阳性的Merkel细胞,因此在诊断外阴Paget病时一定要结合形态学。
这样看来,赵老师这例我诊断---外阴原发性Paget病(CK7+、CEA+、CK5/6+、GCDFP-15弱+、HER-2+、p63大细胞--、CK20--、S-100--)
-
学习了,去年写了有关这方面的综述,把其中的结语摘录如下:
7.结语
在PD的各种变异型中,至少MPD的组织发生是有争议的。基于PC和其下的导管癌具有相同的黏液免疫表型,目前的研究支持亲表皮播散理论是其下有导管癌的MPD最重要的来源这种观点,而Toker细胞可能是部分其下没有乳腺癌的罕见MPD的来源。肛周的PD是特殊的,是仅表达MUC2的一组PD,提示MUC2做为识别可能来源于隐匿直肠癌的肛周PD的有用标记物。外阴PD的组织发生比MPD更复杂,乳腺样腺是外阴PD组织发生的另一侯选已被多位学者所推崇,应用粘蛋白基因做为一个新的标记重复验证了这种可能。外阴表皮内Bartholin腺与正常结构具有相同的粘蛋白表型,表皮内来自Bartholin腺或者MUC
PD是由几种奇特的病变实体构成的一组异质性病变,决定PD是表皮内还是表皮外来源对于治疗是最重要的,病理医生和临床医生都应该尽所有的努力检测所有的PD患者其下方是否有恶性肿瘤,黏蛋白基因表达在研究各种类型癌症的发生上是有帮助的,目前的研究显示MUC1几乎在所有的PD普遍表达,也可以用于筛选和确定表皮内PC的存在, MUC1比作为PC通用的上皮标记CK7要好,MUC1和CK7两者都出现在单一导管结构中(如小汗腺管、大汗腺管和Bartholin腺),提示单一导管或者他们的衍生物可能代表了EMPD各种亚型的起源。与直肠癌有关的肛周PD存在MUC2,在预知PD结肠来源方面MUC2似乎比CK20更特异。MUC
-
本帖最后由 于 2009-08-22 18:54:00 编辑
Glad to see above from Dr. Zhang and 青青子矜. I am a gynecologic/breast pathologist, but never do any research or write review about Paget's. Both of you did some research or wrote review articles in this area, so you know more detailed information. Thank for your expert's in-put.
I will continue to complete our resident's summary.
Primary EMPD
n Originate in the skin or apocrine sweat glands
n Not associated with distant adenocarcinoma
n Limited to the epidermis but may progress to invasive tumor, spreading to dermis, blood and lymphatics and potentially lethal metastases.
? Undifferentiated pluripotent cell of the epidermis or adnexa
? Toker cells of the vulvar epidermis
What are Toker cells?
n Intraepithelial cells with pale staining cytoplasm and bland cytologic features
n Located in the epidermis immediately adjacent to lactiferous ducts
n Considered a primitive germ cell of the lactiferous duct or inter-epithelial extension of lactiferous duct cells
n 10% normal nipples on H&E
83% normal nipples and 65% of accessory nipples with CK7 IHC
-
本帖最后由 于 2009-08-22 08:03:00 编辑
Mammary-like glands (MLG)
n Glands that normally occur in the interlabial sulcus between the labia minora and labia majora
n Histologic features of female breast and sweat glands
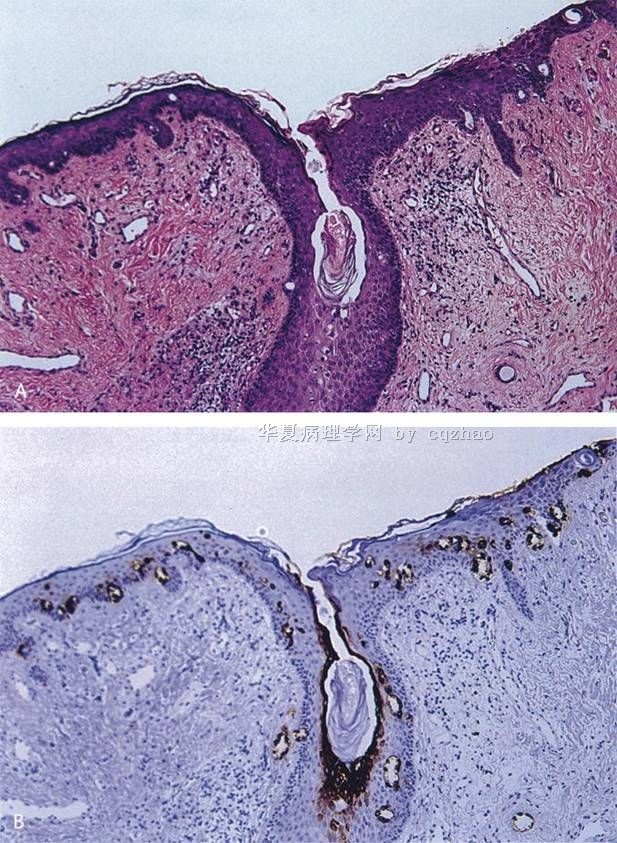
n A, Opening of MLG with formation of duct-like structures by hyperplastic Toker cells (H&E).
B, CK7 positivity in hyperplastic Toker cells (CK7).From: Willman: Am J Dermatopathol, Volume 27(3).June 2005.185-188
名称:图1
描述:图1
Is Toker cells Precursor Cells???
n Toker cells are a feature of the interface between the epidermis and the epithelium of lactiferous ducts of the breast, ectopic breast tissue and MLG.
n Morphologically appear to be benign counterpart of malignant cells in PD.
n Supported by IHC staining
Conclusion
n Extramammary Paget’s Disease is an uncommon neoplasm, occurring most frequently in postmenopausal women on the vulva
n It was once believed to be secondary to underlying neoplasms, like mammary PD.
n Currently it is thought to be divided into two separate types, primary and secondary.
n IHC can aid in determining the type of EMPD and the origin of secondary EMPD.
n Toker cells may be the precursor cells in primary EMPD.
-
本帖最后由 于 2009-08-23 04:51:00 编辑
Above summary is from one of our first year pathology resident. In fact she is resident only for the two month (starting from July, 2009).Residents and fellows need to prepare a lot of talks, case discussion, paper review in department conference, tumor board. They learn pathology knowledge when they prepare the talk. In fact I learned some new information from above our resident's presentaion. Also pathologists need to give reisdents and fellow many teaching course.
Some of the number or percentage may be not very accurate depending the papers you read. You can get a general information about EMPD.
I wish our young pathologists to learn from this case not nly the dx of Paget's. The more importance is to learn the way or thought, priniciple how to make your dx in clinical practice.
As pathologists we always should have differential dx for our cases even for some easy cases. For all paget's dieases we always order some stains to support our dx even though we almost are sure the dx based on the H@E slides. We do not want to misdiagosed melanoma or paget's. This is called low level but too significant mistakes. We may lost the job if we make this kind of mistakes.
Ok, I will finish this topic. Thank all of you who read or wrote the discussion for this topic. I especially appreciate 青青子矜 and Dr. Zhang for sharing their study or review summary.
It is the morning in China and in the US we are in the Friday night. I am playing 麻将game with my family tonight. I just learn it recently. I feel it is interesting and a good relaxing game.
Good weekend, cz
"I wish our young pathologists to learn from this case not nly the dx of Paget's. The more importance is to learn the way or thought, priniciple how to make your dx in clinical practice."
Thanks Pro cz fou your kindness and encouragement. We all have learned so much from your speech and discussion.Thank you,sir!











