
















| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
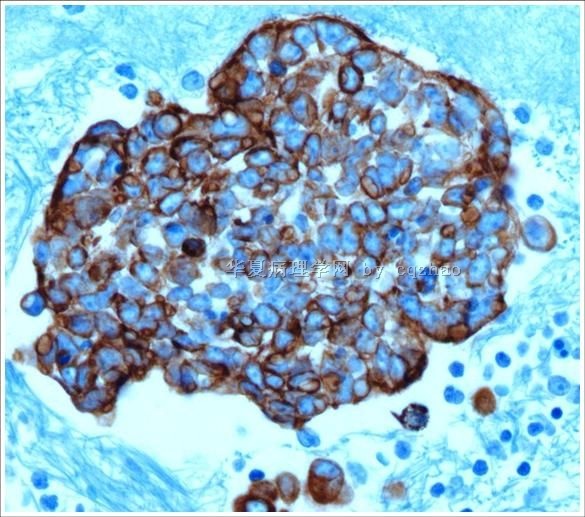
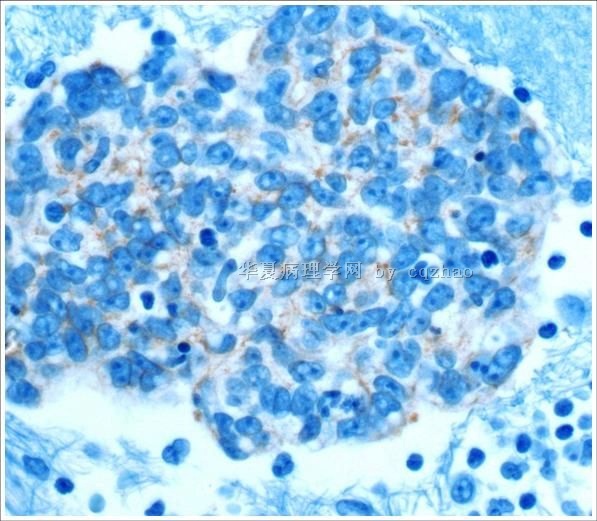
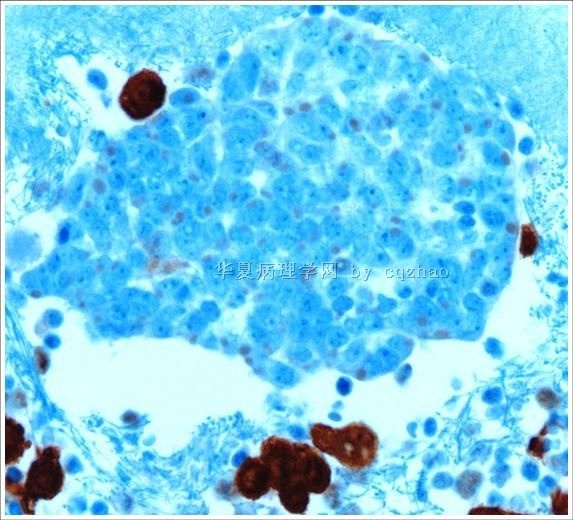
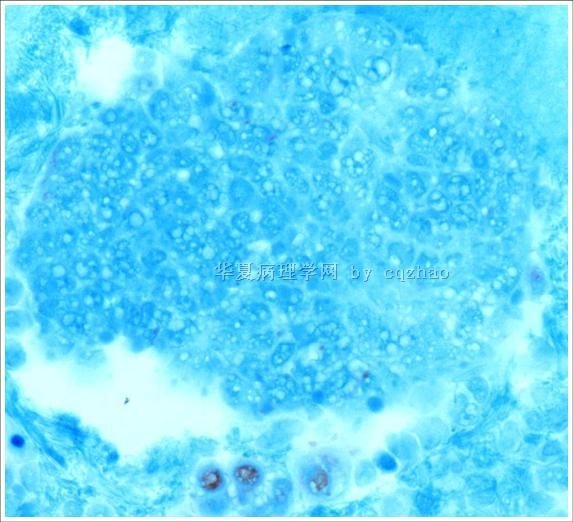
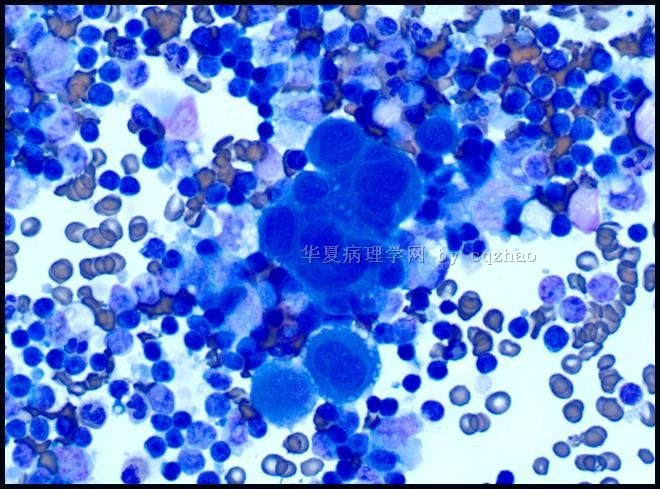
- 70 岁 妇女,胸水,metastatic adenoid cystic carcinoma from lung
-
本帖最后由 于 2009-08-07 11:58:00 编辑
Occasionally saw many body fluid cases with discussion here. I think some people may be nor aware of the principle for dx of body fluid.
1.Most common body cavity fluid in clinic includes pleural effusion and ascites (peritoneal fluid). The mesaothelium is a single layer of flat cells. However, Many reactive conditions can lead to mesothelial cell proliferation, thus binuleaton and multinucleation, increased mitotic figures, nuclear enlargement, increased N/C ratio, coarse chromatin, prominant nucleoli, markedcytological atypia. All these features can mimic neoplastic conditions, and may be misinterpreted as malignancy, especially, adenocarcinoma.
2. When we see a case with atypical glandular-like cells we must rule out if these cells are reactive mesothelial cells. This is very important. If they are mesothelial cells, they are benign reactive cells (of cause rare mesothelioma can be present. If they are epithelial cells they may be metastatic carcinoma cells (except endosalpingiosis in pelvic wash).
3. Remember that some reactive mesothelial cells can look very ugly and some adenocarcinoma cells can look benign.
4. Even though cytomorphology, history, clinical presentation are very important, the IHC stains are very important for some cases, especially for the cases without history. If you make dx only based on cytomorphologic features, you can be right (if you are a good cytopathologist) in most of times. However you will be wrong some times during your pathologist career.
5. Often it is a primary malignant dx in body fluid cytolgy. So we as pathologists have to be very cautious about our dx.
6. There are many markers to distinguish mesothelial cells from epithelial cells.
Epithelial cells: BerEp4, MOC 31, B72.3, CEA et al
Mesothelial cells (reactive or malignant): Calretinin, ck5/6, WT1 et al.
AE1/AE3, CK7, and EMA are postive in mesothelial cells. They are useless for this differentiation.
Many cytopathologists like to use two epithelial markers and two mesothelial markers for the difficult cases because occasionally some markers can have different expression. Some cases of mesothelial cells may ne positive for MOC31, some epithelial cells may be negative for berEp4 or B72.4. Of cause you always make your judgment based on the individual case.
7. If we rule out the mestothelial origin we can consider the possible primary of the malignancy based on cytology, clinical and imaging information, and more IHC stains.
8. The most common cause of a malignant pleural effusion in men is lung carcinoma, and in women it is breast ca. A malignant peritoneal effusion is most commonly caused by a gastrointestinal malignancy in men and by ovrian carcinoma in women.
-
本帖最后由 于 2009-08-06 10:39:00 编辑
| 以下是引用xiangyao在2009-8-6 0:59:00的发言: 请教赵老师,这个病例如果不做免疫组化标记,真的不敢定是恶性的吗?间皮细胞增生到这种程度也恐怕是瘤性的了!还有您们的细胞蜡块做的很好啊,不知道是用什么方法做的?希望能得到您的指导! |
As I mentioned before most of the time you may be right, but you will be wrong some times.
For body cavity fluid cytotech will centrifuge the fluid and make the direct smears, ThinPrep slide, cytospin slide, and cell block always. I do not know exactly how they make in the lab.However they just use the routine or usual methods. You should easily find these methods in some lab tech books or internet
-
本帖最后由 于 2009-08-01 22:47:00 编辑
这个病例比较有挑战性。
图1、2:可见以下细胞,多核的巨细胞(结构不清,可能是间皮)、红细胞、小淋巴细胞,少数中性粒细胞,及数量比较优势的大细胞(核质比高,染色质细腻,少量淡蓝色胞质)——有异型性,看起来是瑞氏染色,似乎是异型淋巴细胞或单核细胞。
图3、4:明确异型的细胞团,核仁明显且多个,核膜厚,细胞边缘似乎毛糙,疑恶性间皮瘤或腺癌;
图5、6:异型细胞团,细胞核似图1、2的散在异型细胞,核仁小而清晰,染色质细腻,尚见红色小球状结构(分泌物?——免疫球蛋白?),可见分裂相;
图7:与图1、2类似,不过中间的大团细胞结构比图1、2的较为清晰,见到开窗结构、围裙现象,考虑是间皮,见到更多的小淋巴细胞。
一般情况下,高龄患者的胸水首先想到肺癌。可是,本例图像很复杂,似乎是并病。
连猜带蒙:腺癌,伴大B细胞淋巴瘤。

- “人生没有彩排,每一天都是现场直播”











