







| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
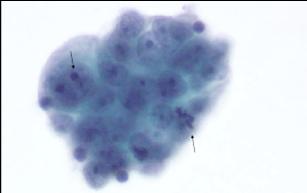
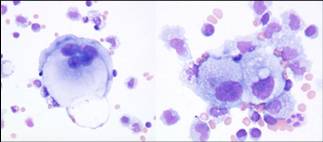
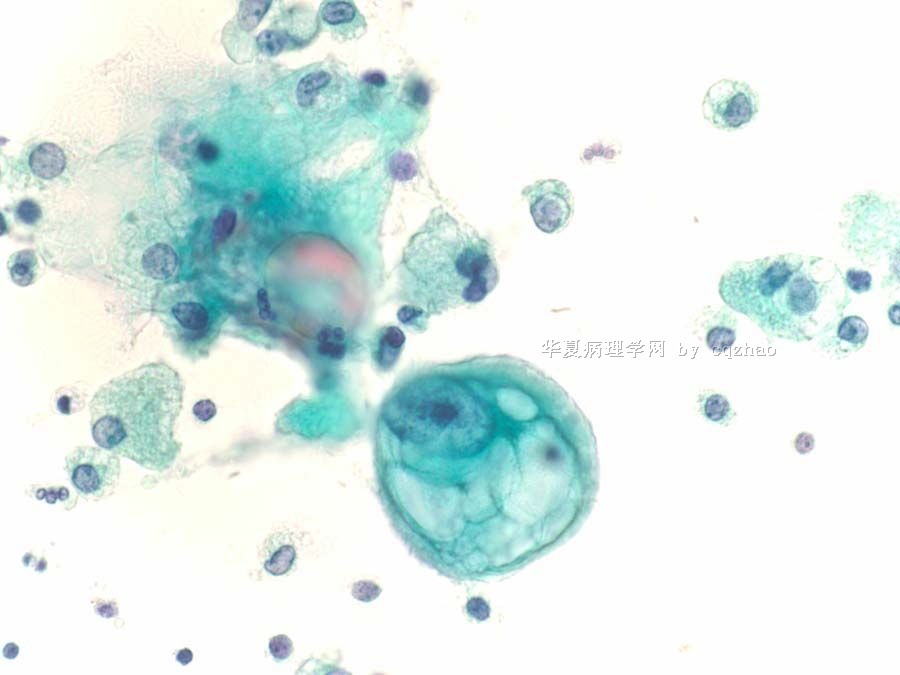
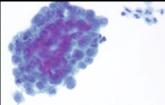
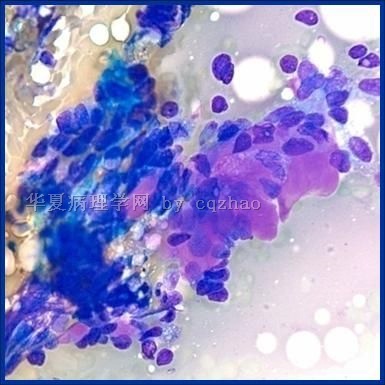
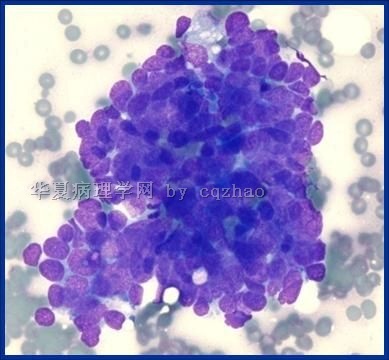
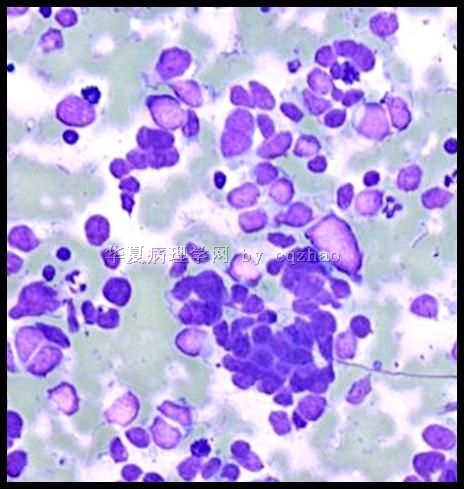
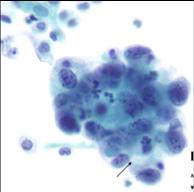
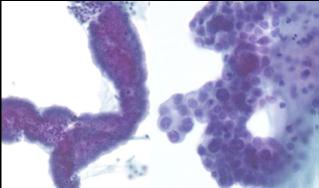
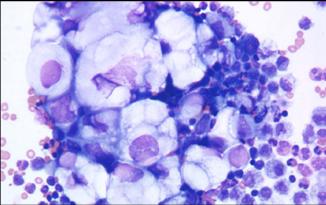
- 70 岁 妇女,胸水,metastatic adenoid cystic carcinoma from lung
-
本帖最后由 于 2009-10-11 07:59:00 编辑
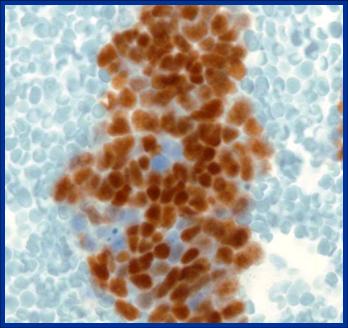
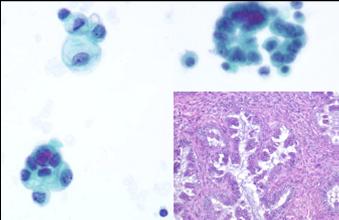
Fig 3 for p63 stain
Basaloid Squamous Cell Carcinoma
n Highly aggressive malignant tumor
n Head, neck, and anal region
n Cytomorphological features:
- nests or cords of small crowded cells
- minimal cytoplasm
- nuclei - hyperchromatic,
- prominent hyalinization
- peripheral palisading
- mitotic activity
n IHC: 34BE12, AE1/3, CAM5.2
名称:图1
描述:图1
名称:图2
描述:图2
名称:图3
描述:图3
Lymphomas and Leukemia in Effusions
n Known complication
n Decline in numbers
n Rarely primary manifestation
n Cytomorphological features:
- dyscohesive
- necrosis, entire cells or mercury drop karyorrhexis
- small cells, immunoblast like cells, immature plasma cells
-
本帖最后由 于 2009-10-11 07:56:00 编辑
Metastatic Small Cell Carcinoma
n Primary from lung, bladder, esophagus, prostate
n Highly aggressive tumor
n Cytomorphology highly accurate and reliable
n IHC – Neuroendocrine markers, pancytokeratin (100% dot like), TTF-1
名称:图1
描述:图1

名称:图2
描述:图2
Malignant Mesothelioma
n Diffuse growth
n No foreign population
n Knobby flower like clusters
n Occasional giant cells
n Dense cytoplasm
n Central/paracentral location of nucleus
n Collagen balls
n Psammoma bodies rare
n Acidic mucin – Alcian blue
n EM – long slender microvilli
Benign/reactive Mesothelial Cells
n Single/small clusters
n Flat/cuboidal
n Cytoplasm – bi-phasic
n Nuclei - single/bi/multinucleated
n Reactive cells mimic mesothelioma
n Inflammatory background
n Causes: Pneumonia, PE/ infarct, cirrhosis, hepatitic, uremia, pancreatitis, dialysis, chemo/radiotherapy
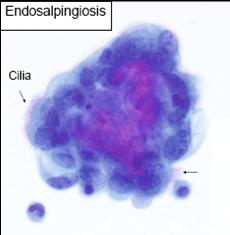
Adenoid Cystic Carcinoma
• Uncommon malignant salivary gland neoplasm
• Mainly head and neck region.
• Indolent growth and multiple local recurrences.
• Metastasis - lung, bone and rarely involves pleura and pericardium.
• Grading
- tubular and cribriform patterns are considered low grade/grade 1
- 30% to ~70% solid is intermediate grade/grade 2
- predominantly solid is high grade/grade 3
n Differential diagnosis –
- Basal cell adenoma/adenocarcinoma
- Small cell carcinoma
- Basaloid carcinoma.
n Immunohistochemistry:
-cells in ducts - Keratin, CEA, alpha-1 chymotrypsin,
S-100, CD117
- cells around pseudoglandular spaces - S100, actin
- dedifferentiated tumor - S100
-
本帖最后由 于 2009-10-11 07:53:00 编辑
I pasted this case here for a long time. No person asks what is the original tumor for this malignant plueral effusion. It seems that i have to 唱独角戏to finish this case. Ha, ha.
The patient had lung FNA biopsy to dianosis of adenoid cystic carcinoma (ACC). The FNA was done in another hospital. I read the surgical report and cannot take photos to show you. The lung tumor is positive for Pan CK, CK7, S100 (focal), p903, and negative for synaptophysin, cd56, p63, and TTF-1. Ki67 shows positivity in 35% of the cells. The differential dx included small cell carcinoma and IHC did not support. ACC can be a primary from bronchial primary or metastatic from salivery gland origin. Since this patient had parotidectomy for a malignant tumor (do not the dx), it is possible that the current tumor is a metastatic from parotid if the parotid tumor was ACC.
-
本帖最后由 于 2009-09-12 19:53:00 编辑
Endometrial endometrioid adenocarcinoma
ovarian serous borderline tumor
ovarian mucinous borderline tumor
ovarian mucinous borderline tumor (right top: mesothelial cells, left two clusters: mucinous borderline tumor, histology: mucinous borderline tumor)
名称:图1
描述:图1
名称:图2
描述:图2
名称:图3
描述:图3
名称:图4
描述:图4
-
本帖最后由 于 2009-09-10 06:58:00 编辑
Agree with above.
The work concept may be different in different work condition, sources. Currently in the USA, Pathologists (at least most) will try hard to identify the primary for body flood positive cases. For example patient has a lung mass with positive pleural flood, we will do ck7, ck20, TTF1 and try to confirm the lung primary. The pathologic diagnosis should include malignant or benign, also the possible origins. Even for the lung mass FNA, we also do some basic immuno panel to confirm the primay and types (squamou carcinoma, adenocarcinoma, small cell carcinoma).











