























| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
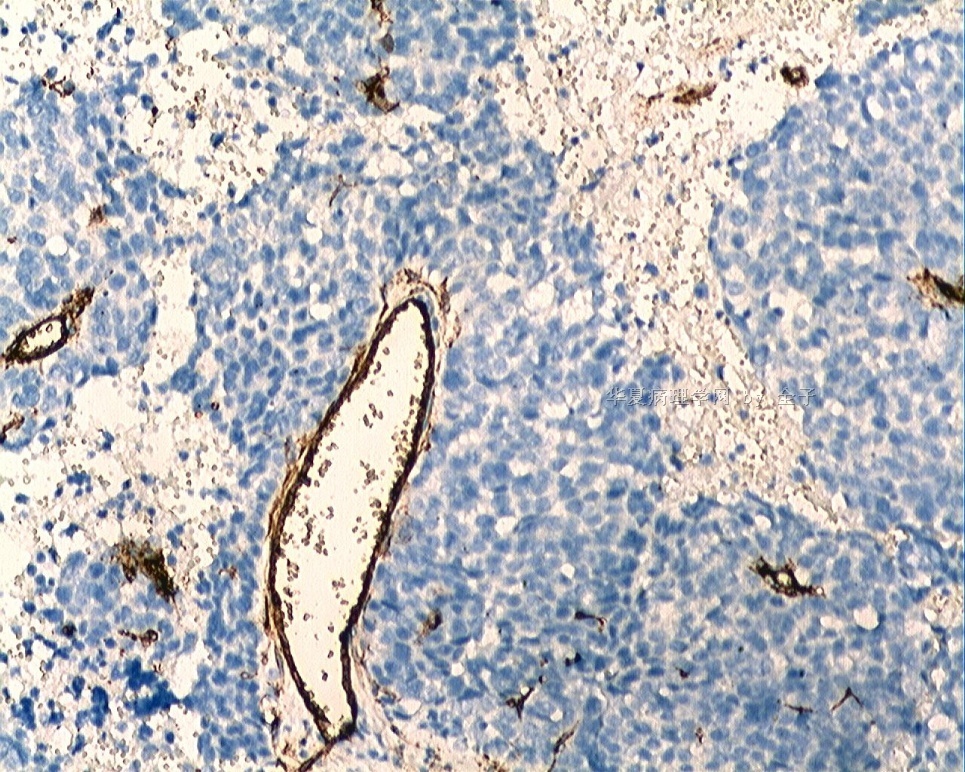
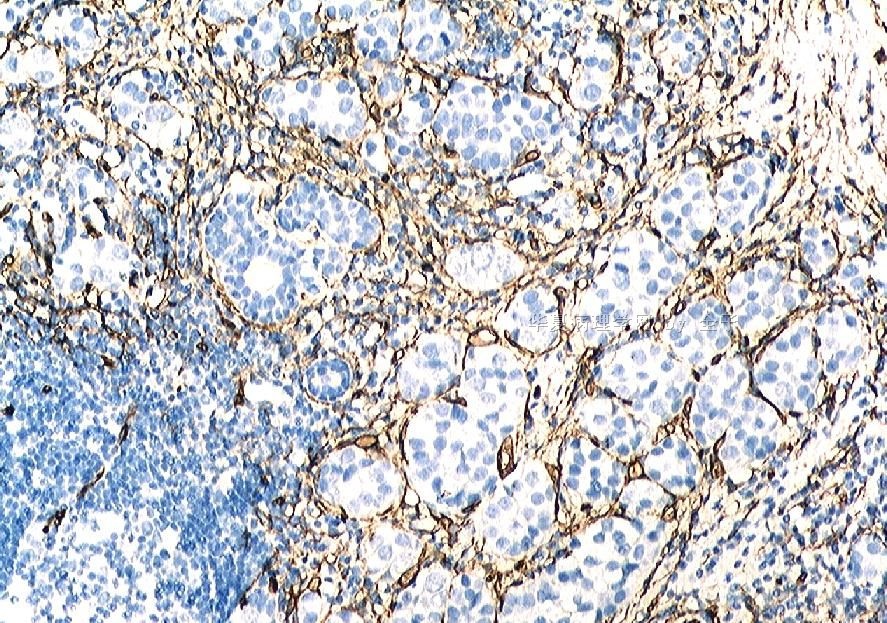
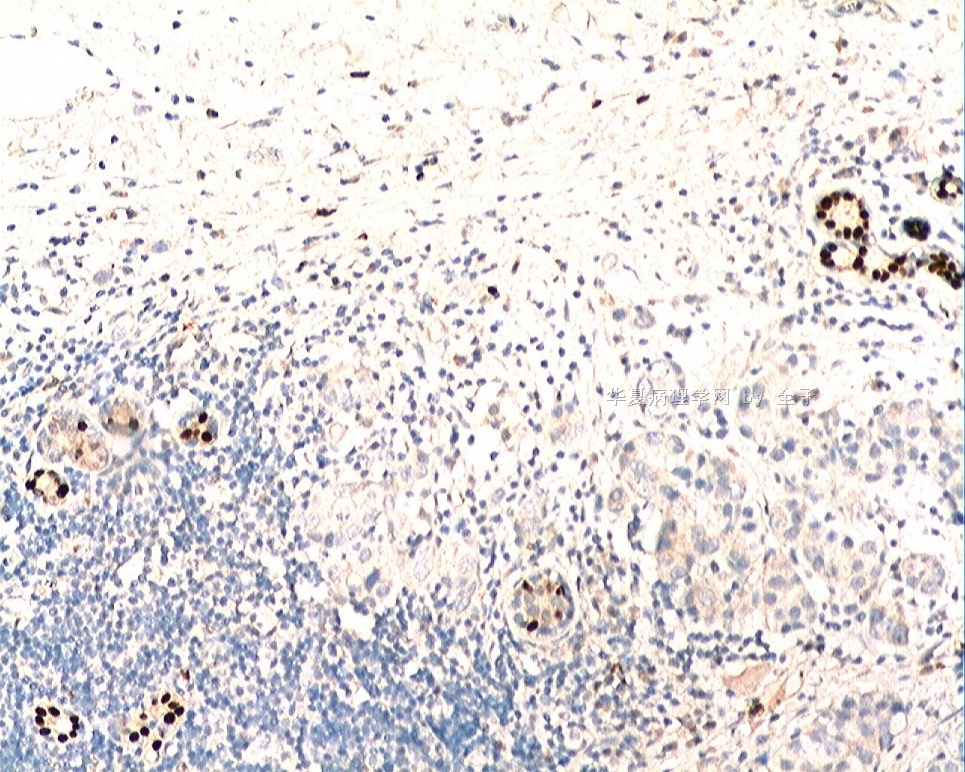
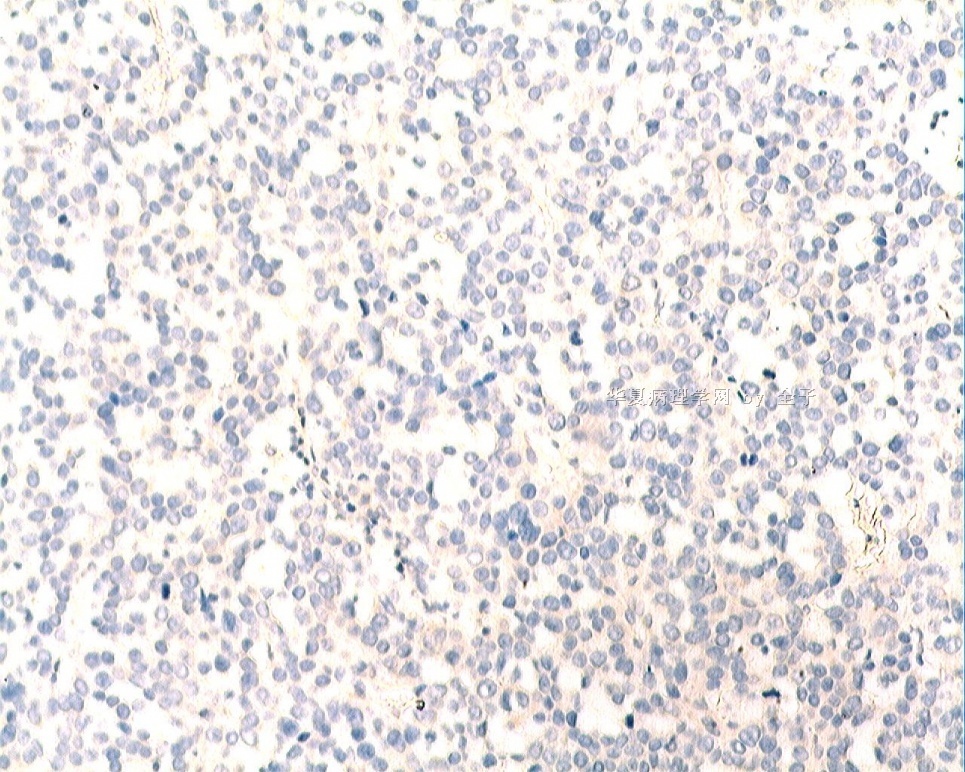
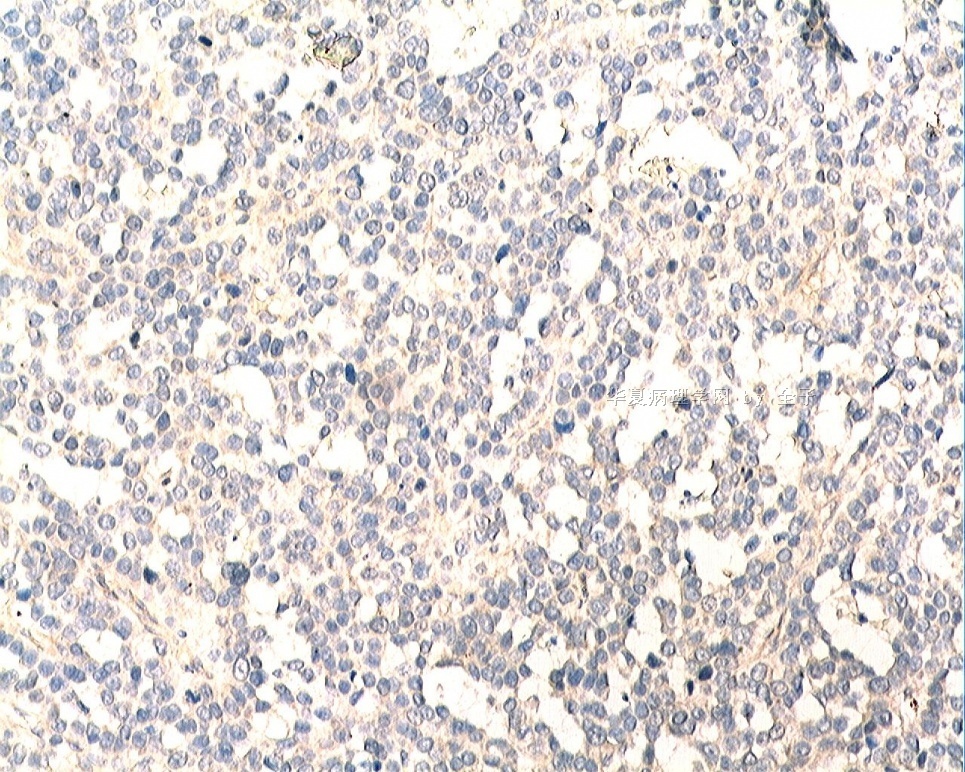
- B1833乳腺肿瘤,请教什么类型
 图1
图1 图2
图2 图3
图3 图4
图4 图5
图5 图6
图6 图7
图7 图8
图8 图9
图9 图10
图10 图11
图11 图12
图12 图13
图13 图14
图14
| 姓 名: | ××× | 性别: | 女 | 年龄: | 46 |
| 标本名称: | 乳腺肿块 | ||||
| 简要病史: | 发现肿物3天 | ||||
| 肉眼检查: | |||||
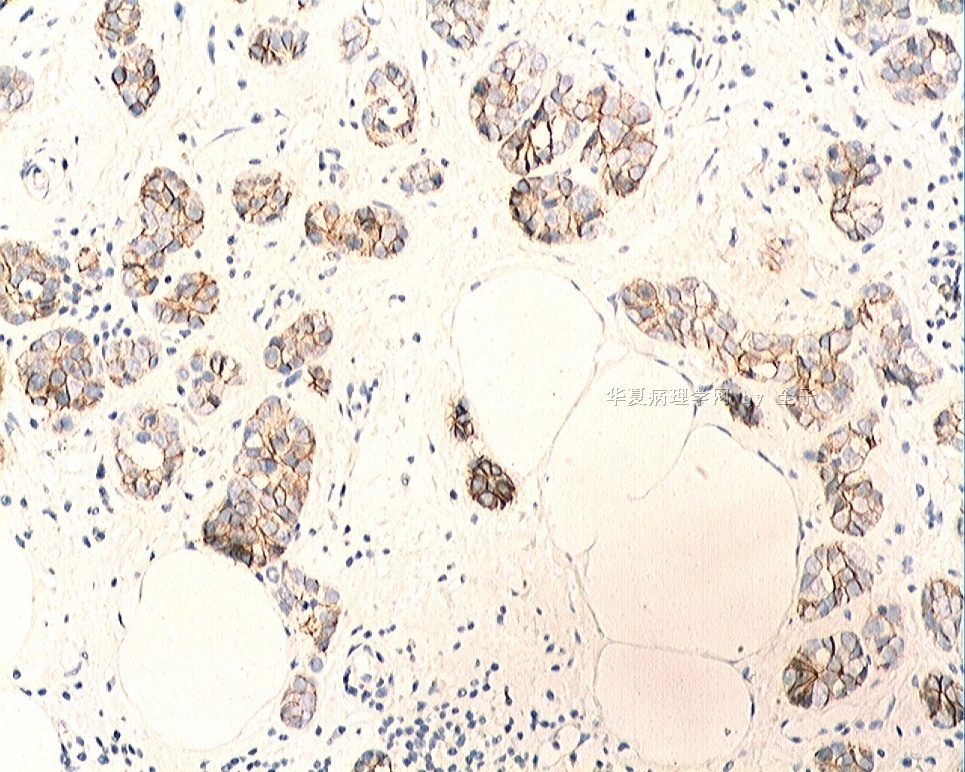
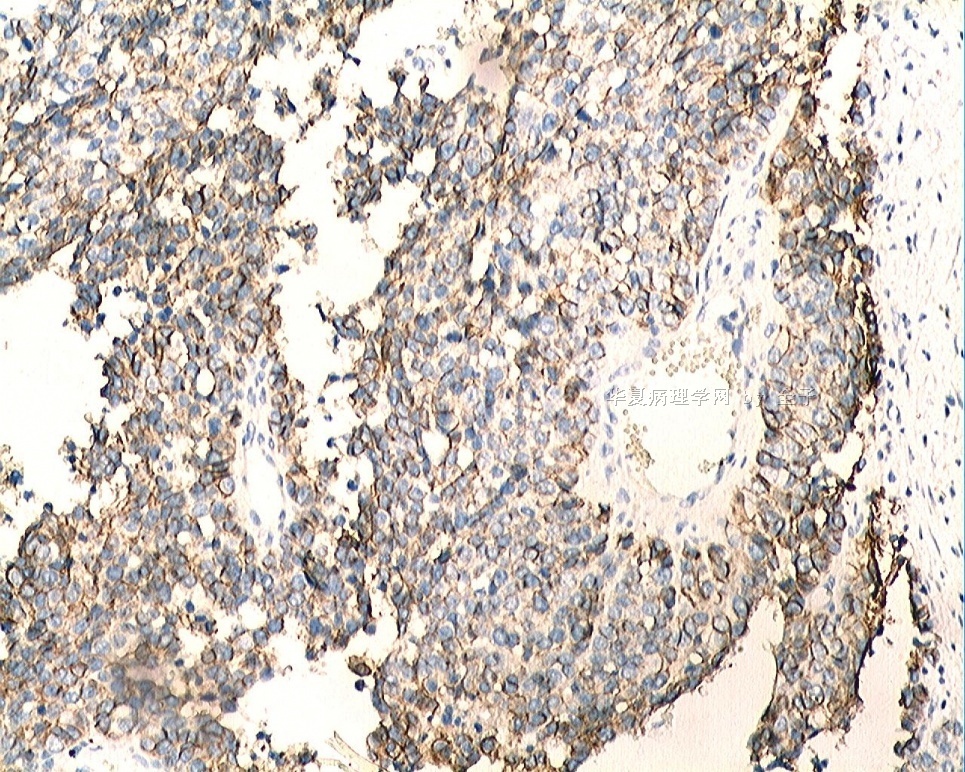
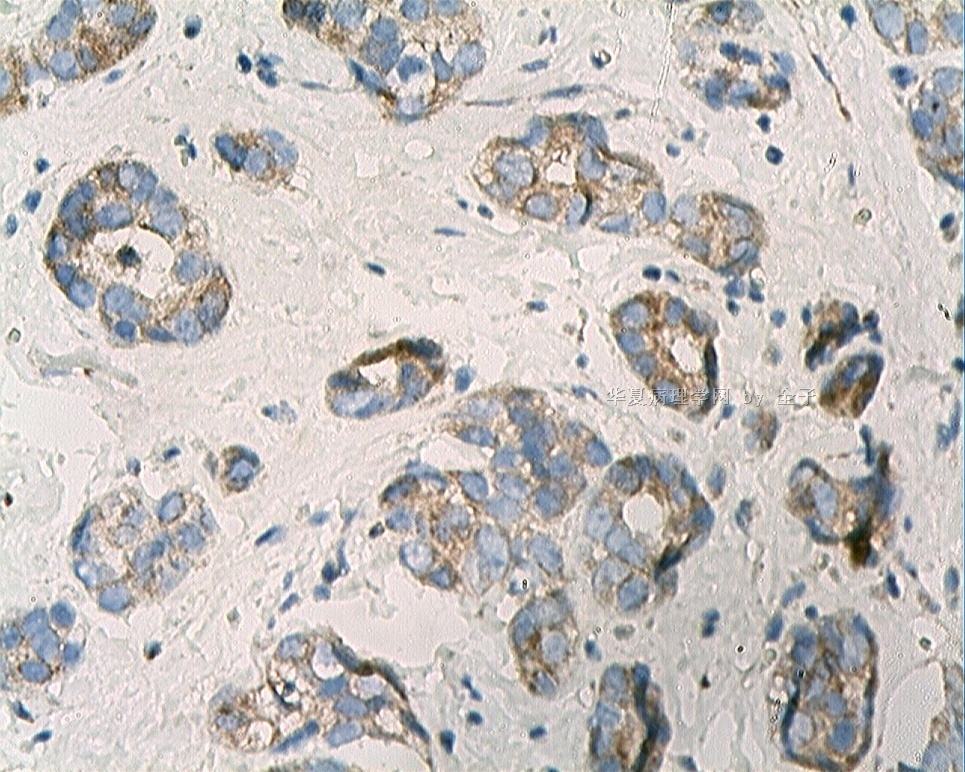
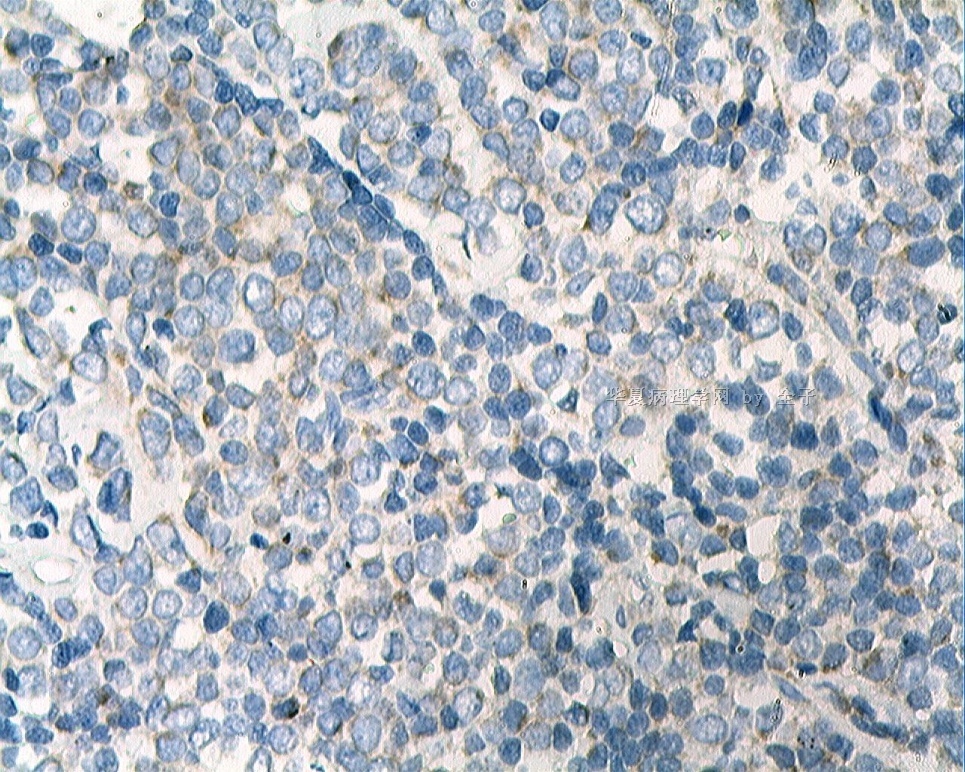
标签:乳腺浸润性导管癌 神经内分泌分化
-
本帖最后由 于 2009-06-13 13:40:00 编辑
相关帖子
×参考诊断
-
本帖最后由 于 2009-06-14 22:37:00 编辑
| 以下是引用笃行者在2009-6-14 21:40:00的发言:
是个少见的图像,前几幅图令人头痛,后几幅图似浸润性导管癌。 “血管源性肉瘤”是个大胆的想法。是的思路应该开阔,“一切皆有可能”。当然应首先考虑常见的肿瘤,常见的肿瘤不像,就要考虑少见的,原发的不像,就要考虑转移的。 |
Agree.
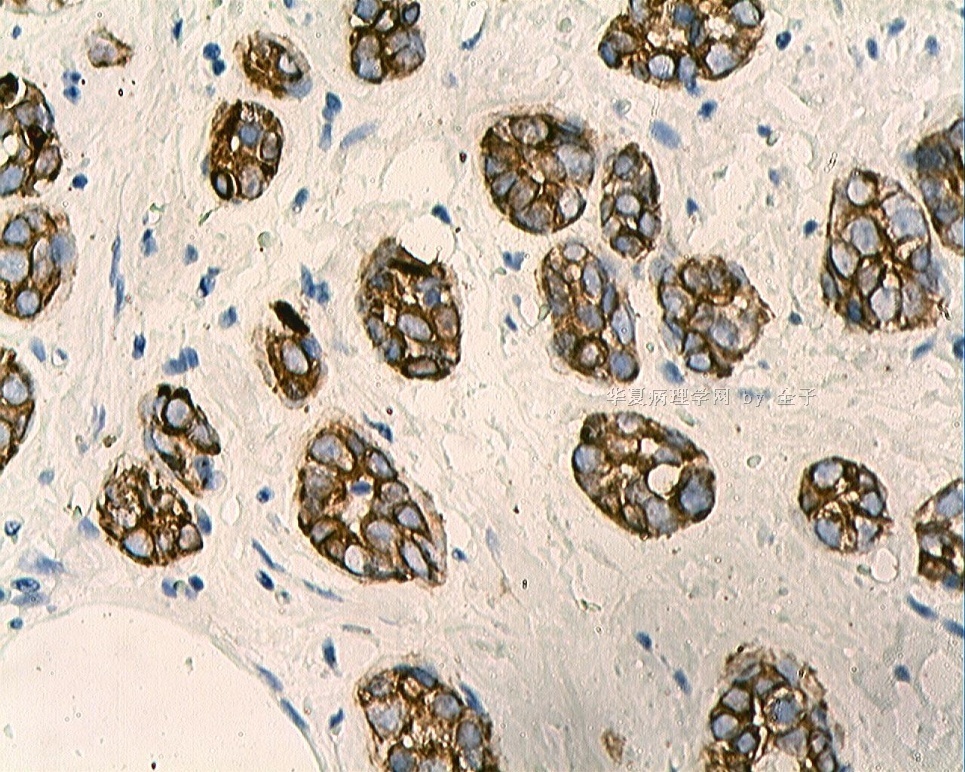
1. Last photos show small glandular formatons, cytologic atypia, mitoses, like invasive ductal ca. Difficult to interpretate the first group of photos. The chance of one tumor is much more common than that of two different tumor in same breast. Do some Pan CK stain to see if the two areas show same positivity. If the cells in first photos are negative for CK stains. Then think others.
2. Original or metastatic tumor if it is a adenocarcinoma case. It is true it is not very typical breast invasive ductal ca even in the last few photos.
Check if pt had malignant history, clinical impression and x-ray information.
If not sure, do IHC CK7, CK20, ER, PR, mamaloglobin, TTF-1. GYN, lung, GI....
3. Then think more.
Confused by the growth pattern of the case.
In fact it is not difficult to have dx if you have your DDX and IHC.
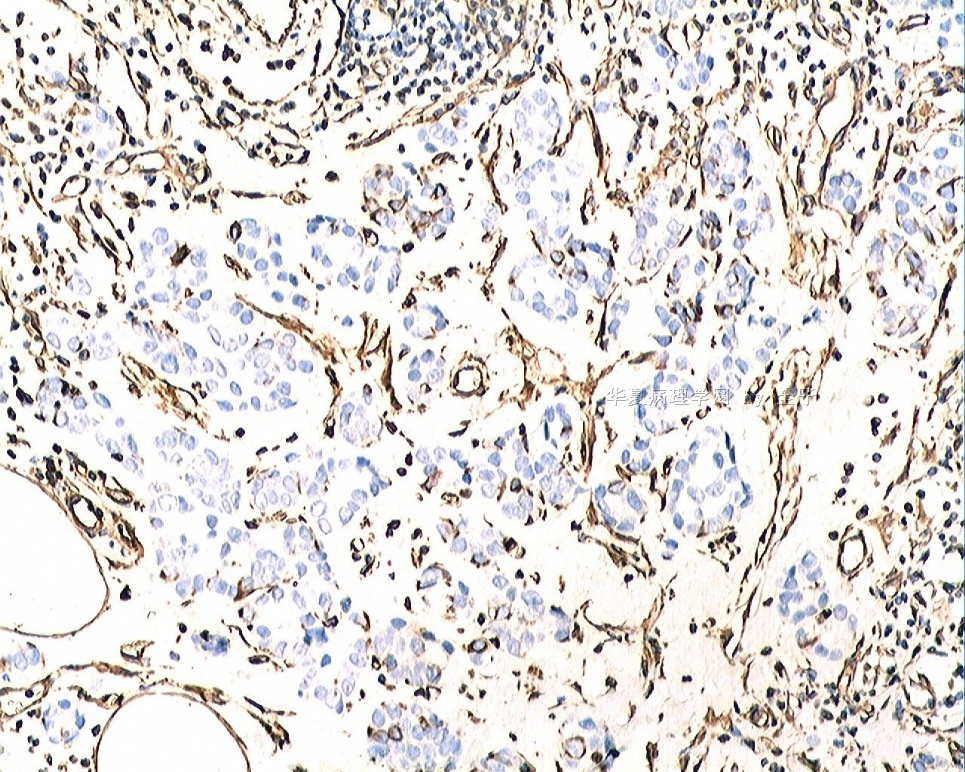
First figs: germ cell tumor-york-sac tumor (kiding in 46 y-breast) angosarcoma (not typical)
Last few photos: microglandular adenosis-pattern, atypical or maligant
One tumor with different growth patterns or two different tomors. I guess it is one tumor.
Anyway waiting for Quan zi's IHC results.
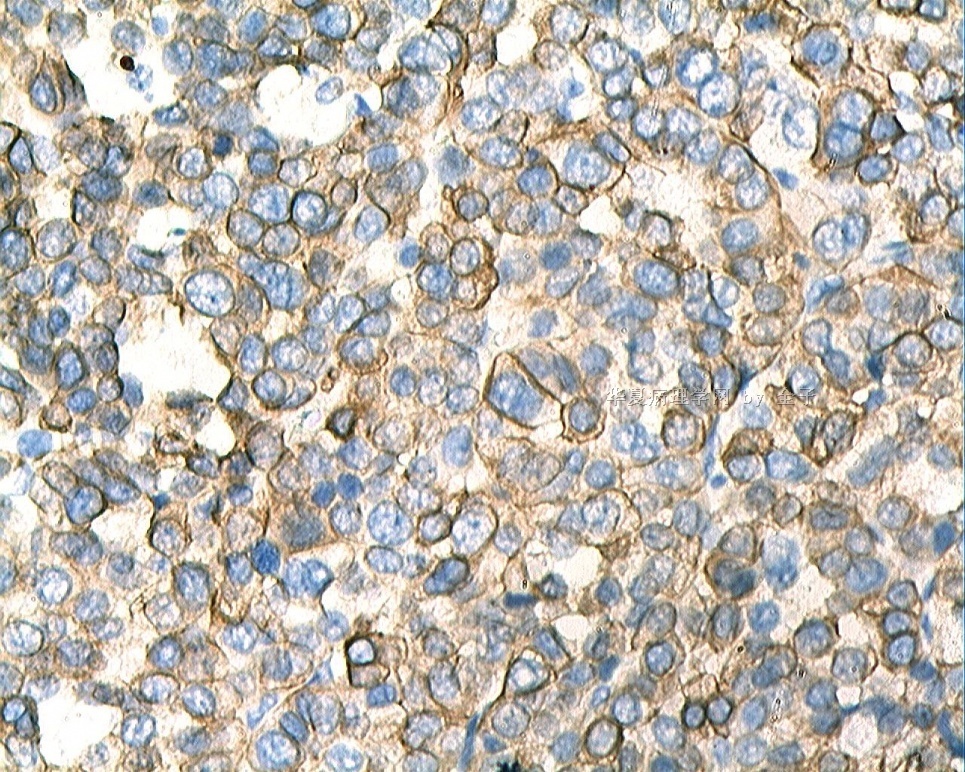
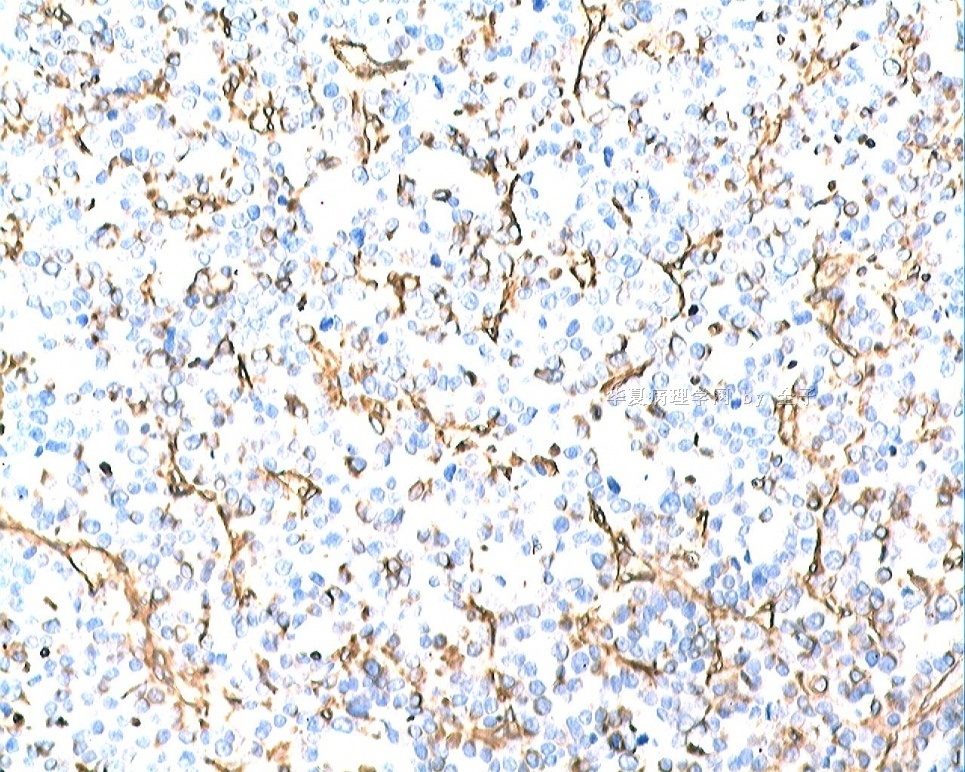
This case does have two different appearances. The poorly differentiated area is composed of rather smallish cells forming sheets or loosely cohesive islands with apparent necrosis. Nucleoli are not conspicuous. This gives me an impression of neuroendocrine tumour. The other apperance I would consider as a classical invasive ductal carcinoma with infiltration of poorly formed glands, pleomorphic tumour cells and conspicuous mitoses.
If neuroendocrine differentiation can be confirmed by immunohistochemistry (CD56, synaptophysin, of chromogranin A in > 50% of tumour cells), the issue of two different appearances would be easily solved.
Before above speculation, I would like to know, like Dr Zhao said, more information about this case. Such as sections showing junction of both appearances, past history of any malignancy, immunostains including cytokeratin, LCA, ER, PR, Her-2.....
-
cqzhao老师意见:
同意笃行者意见。
1.最后几幅图显示小的腺体形成,细胞出现不典型性,有核分裂,像是浸润性导管癌。开始的几幅图比较难解释。当然在一个病例中,发生一个肿瘤的可能性比同一乳腺中发生两个不同肿瘤的可能性要大的多。可以做一下CK-Pan染色看这两个区域是否都是阳性。如果前面几幅图染色阴性,那么就要考虑其他的了。
2.如果是腺癌,那么是原发的还是转移的呢?毕竟最后的几幅图也不是很典型的乳腺浸润性导管癌。看一下患者是否有恶性肿瘤病史,临床情况如何,X线检查有无提示。如果还不能确定,可以做CK7,CK20,ER,PR,mamaloglobin,TTF-1.有无可能是妇科肿瘤?肺部肿瘤?消化道肿瘤……等等
3.三思啊……
对此病例的生长方式比较困惑。
实际上如果你的鉴别诊断和免疫组化做的好做的到位,其实并不难做出诊断。
前面几图:生殖细胞肿瘤?在46岁乳腺发病的少见。血管肉瘤?不典型啊。
后面几图:微腺样-腺瘤样生长,不典型,恶性的?
是一个肿瘤有不同的生长方式呢?还是两个不同的肿瘤呢?我认为是一个肿瘤。
不管如何说,都要等全子的免疫组化结果

- 赚点散碎银子养家,乐呵呵的穿衣吃饭
-
漫游人老师意见:
该例确实是有两种不同的表现。低分化区域是由一些很小的细胞形成片状或者疏松的细胞岛样,有明显的坏死。核仁并不显著。这些给我的印象就是个神经内分泌癌。另外一个考虑就是一个典型的浸润性导管癌伴有低分化腺癌的浸润,细胞多形性,并有显著的核分裂。
如果免疫组化可以证实神经内分泌分化(CD56,Syn,CgA等在50%以上的细胞表达),那么两种不同表现的问题就很轻松解决了。
在作出以上结论之前,就像赵老师所说,我想知道关于该病例的更多信息。比如两种不同表现区域之间是怎么样的?过去有无恶性肿瘤病史?免疫组化如CK,LCA,ER,PR,Her-2……
- 赚点散碎银子养家,乐呵呵的穿衣吃饭
I am waiting my slides.
Come here to see this case again.
Quan zi: please show us some low power phtos. I want to know the relation of the first 6 photos to others.
Did you use different stains? Why did two groups of photos show different color?
If you will give us one IHC stain only, I want to know pan-CK for both two areas. Common things are common. I still think it may be one lesion if I do not know any IHC.











