














| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
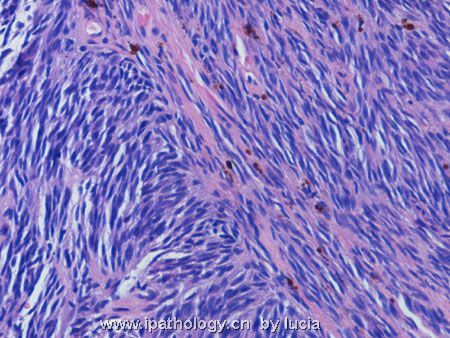
- 颅内肿瘤-转移性恶黑
Thank Dr Mjma very much for the differential diagnosis.
The diagnosis is metastatic melanoma.
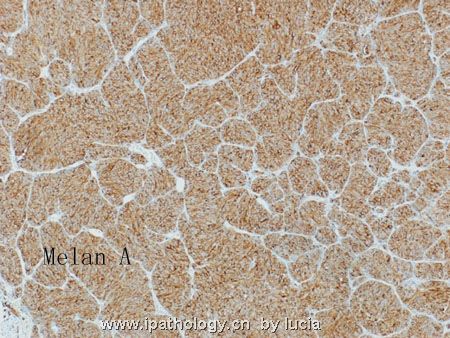
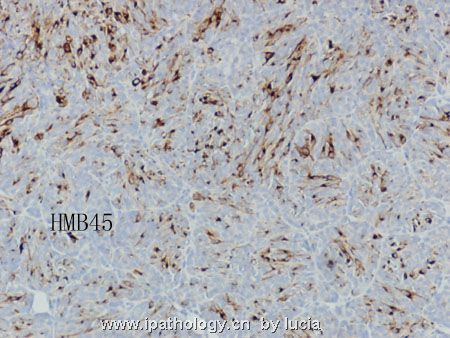
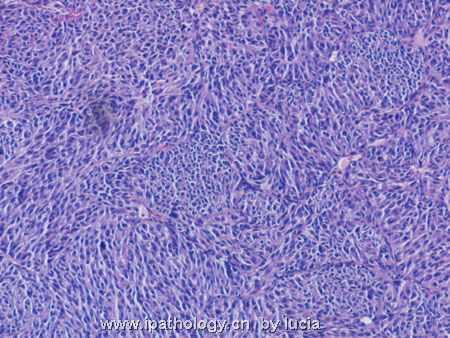
This tumour demonstrated two different morphologies. In most areas the tumour cells are oval and arranged in nests separated by thin fibrovascular tissue. In other areas the tumour cells show elongated nuclei and arranged in fascicles (not shown last time). With these morphologies, both primary, ie gliosarcoma and malignant meningioma, and metastatic tumour have to be considered. With no identifiable fibrillary background in the entire tumour, glial tumour can be readily ruled out. Because of entirely intracerebellar growth, meningeal origin is also unlikely. Metastatic tumours should consider melanoma (coexists of both nested and spindled areas), neuroendocrine tumour (nests separated by fibrovascular septa) and poorly differentiated carcinoma. Immunohistochemistry shows that the tumour is positive for S-100, Melan-A and HMB45. However, no melanin pigments are identified. It is negative for cytokeratin, synaptophysin, chromogranin and GFAP.
The patient presented with no history of any primary lesion. She died soon after operation. The cranial lesion is solitary.
名称:图1
描述:图1
名称:图2
描述:图2
名称:图3
描述:图3
名称:图4
描述:图4
-
本帖最后由 于 2006-10-09 09:50:00 编辑
Key features observed are circumscribed tumor border (assuming this is representative of the entire tumor border), high cellularity, focal nesting pattern, oval to slightly elongated nuclei, faintly eosinophilic cytoplasm, and poor differentiation towards epithelial, glial or neuronal lineages. A cerebellar tumor in a 61-yr-old woman with such histopathology and strong S100 immunoreactivity has two directions of diagnostic interpretation - secondary (metastasis) or primary tumor. Clinical implication and further management of the two directions are very different, and pathologists are charged with this important responsibility. If this is a primary brain tumor, possibilities include medulloblastoma (rare, but does occur in older individuals) and small cell variant of glioblastoma. S100 immunoreactivity effectively rules out large B cell lymphoma. The circumscribed tumor border is not that seen in glioblastomas. If this is a case of medulloblastoma, the large cell/anaplastic variant has to be considered. For some reasons, cerebellum is a preferred site of metastasis in older adults. This preference is disproportionate to its relative volume in CNS and so far has not been satisfactorily explained. Two important differential diagnoses exist in this direction - metastatic melanoma and metastatic small cell (or neuroendocrine) carcinoma. The presence of faintly eosinophilic cytoplasm (without melanin pigment) is against the possibility of metastatic small cell (neuroendocrine) carcinoma. It is hard to tell nuclear chromatin pattern from the uploaded photos. Small cell carcinomas usually do not show large prominent nucleoli, whereas melanomas often do, accompanied by occasional intranuclear pseudoinclusions. Strong and diffuse S100 immunoreactivity is probably the diagnostic clincher of this case. This certainly favors metastatic melanoma over the other possibilities discussed. Before doing more immunohistochemical stains (Melan A, HMB45, GFAP, cytokeratin, synaptophysin) to rule in melanoma and to rule out small cell carcinoma and medulloblastoma, I would check the patient's history to see if a known melanoma of skin exists currently or in the past, and whether this is a solitary lesion in CNS (metastasis to brain are often multifocal). If history of melanoma is positive and this is just one of several CNS lesions, the diagnosis of metastatic melanoma is definite. If no such history exists and the lesion appears solitary, I would then proceed with additional stains as listed above to delineate its nature. This case demonstrates a common scenario in our clinical practice - very educational. Thanks.

聞道有先後,術業有專攻











