








| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
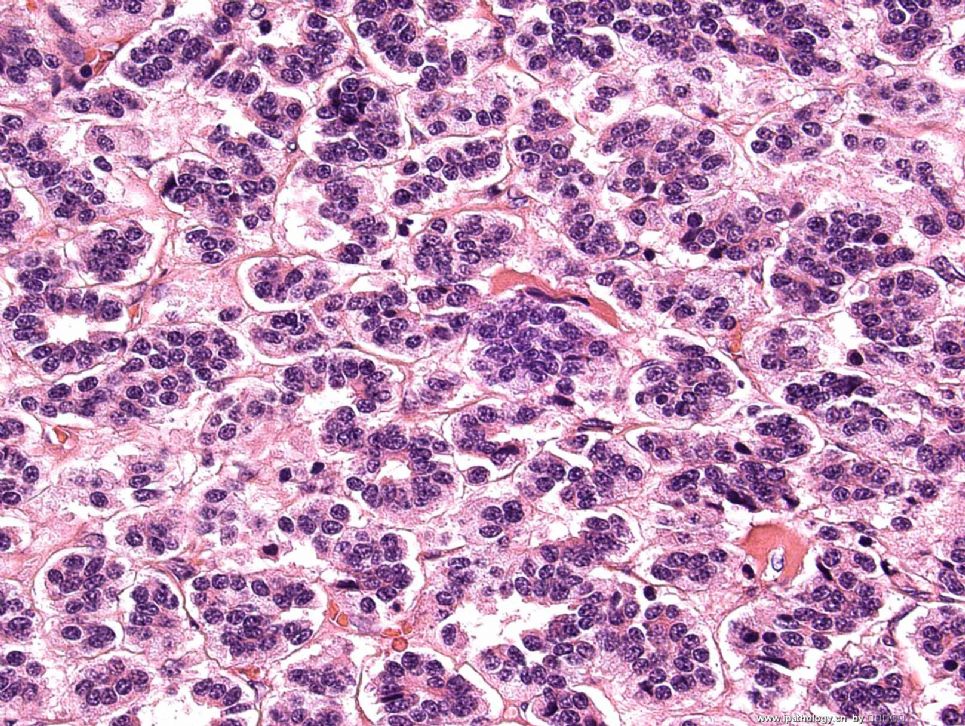
- Lung nodule FNA
 图1
图1 图2
图2
My camera was broken for some days. Have not posted any cases. Here is a recent case. A 42-year-old man with a endobronchial tumor. Broncoscope-guided FNA was done. Please see the above two posted pictures by Pap stain. I think that this case is pretty typical.
标签:
×参考诊断
低度恶性的神经内分泌肿瘤
One of the posters is right on the diagnosis. I am more interested in what's your diagnosis on this case without immunostains? What if you are practise pathology in a very rural setting? no immuno lab exists?
I did NOT do any immunostain in this case, sorry I don't have pictures to share. But, I have the patient follow-up information. Thanks!
| 以下是引用陈隆文博士在2009-3-5 23:35:00的发言:
One of the posters is right on the diagnosis.上帖之一的答案是正确的, I am more interested in what's your diagnosis on this case without immunostains?我更感兴趣的是你没有看到免疫组化凭什么做出的诊断。 What if you are practise pathology in a very rural setting? no immuno lab exists?是否你在偏僻的地区医院工作没有做免疫组化条件? I did NOT do any immunostain in this case, sorry I don't have pictures to share.本例也没有做免疫组化,因此也不能提供给大家分享。 But, I have the patient follow-up information. Thanks!但是我有随访结果。谢谢! 不知道陈老师是不是说我,如果是我那可太好了,猜对了算是蒙的!诊断低度恶性的神经内分泌癌是根据细胞形态,感觉细胞是肿瘤细胞,但没有太大的异形性,细胞较一致。核内染色质有点呈神经内分泌癌的特点。我们医院是省级,1000张床。有免疫组化室。但是病理水平还是不高,特别是免疫组化这一块需要好好学习。 |
 图1
图1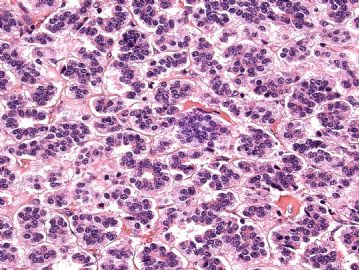 图2
图2
I am a little surprised that some people went for lymphoid lesions. Maybe, the pictures I took are not that representative. I did not think that this is a lymphoma based on 3 features: 1) The cells are very cohesive in some areas, lymphomas are usually more dispersed than this (remember these are smear pictures, not liquid-based slides); 2) I did not see lymphogladular bodies, which are usually seen in lymphoid samples; 3)some cells have more cytoplasm for lymphoid cells.
月新is right, this is a low-grade neuroendocrine tumor (carcinoid) and it is pretty classic on cytology. In our hospital, we as pathologists are regularly communicate with our clinicians to try to get the best patient care. This case, the pulmonologist talked with me before I signed-out the case and his clinical impression is carcinoid tumor too. He said to me that the clinical management of the patient will be surgical resection of the tumor as long as it is a low-grade epithelioid neoplasm. So, I felt that it is not necessary to do immunostains in this case and charge the patient unnecessary money. Thus, my diagnosis is low-grade epithelioid neoplasm, consistent with low-grade neuroendocrine tumor. I post two pictures of the resection specimen of the tumor.
I feel that as pathologists, we are a important part of the patient care team, we are like director of a movie, so communication with other clinicians (radiologists, surgeons, oncologists, etc.) are very important, these communication will not only benefit clinicians and patients, but also benefit us. Staying in your own office and just look at slides without communication and do a lot of unnecessary immunostains to get a diagnosis is not a good practice. For cytology, just giving a diagnosis without thinking about patient management is also very dangerous. Sorry for the long message, just my thoughts.
I am a little surprised that some people went for lymphoid lesions.我有点惊奇,有些人猜是淋巴瘤。 Maybe, the pictures I took are not that representative.可能是我采的图代表性不强, I did not think that this is a lymphoma based on 3 features我感觉不能根据这三幅图说是淋巴瘤: 1) The cells are very cohesive in some areas, lymphomas are usually more dispersed than this (remember these are smear pictures, not liquid-based slides)1、这些细胞非常集聚,淋巴瘤细胞比较分散,请注意这是穿刺涂片不是液基涂片,; 2) I did not see lymphogladular bodies, which are usually seen in lymphoid samples;我没有看到淋巴腺小体,也就是我们在淋巴结活检应该看到的的淋巴样细胞和结构。 3)some cells have more cytoplasm for lymphoid cells.3、有些细胞有淋巴样细胞的较多的胞浆。月新is right,月新答案是对的, this is a low-grade neuroendocrine tumor (carcinoid) and it is pretty classic on cytology.最后诊断是低度恶性的神经内分泌肿瘤。细胞学改变是非常典型的。 In our hospital, we as pathologists are regularly communicate with our clinicians to try to get the best patient care.在我们医院做为我们病理医生要常规的和临床医生构通,为了得到更多的患者的信息,能使病理诊断更好。This case, the pulmonologist talked with me before I signed-out the case and his clinical impression is carcinoid tumor too. 在我没有做此诊断以前,肺科专家也已经从临床角度考虑为肺类癌。He said to me that the clinical management of the patient will be surgical resection of the tumor as long as it is a low-grade epithelioid neoplasm.他给我说,如果咱们都认为是低度恶性神经内泌癌,就准备用手术切除这个肿瘤。 So, I felt that it is not necessary to do immunostains in this case and charge the patient unnecessary money. 因此我们感觉没有必要再做免疫组化,省点钱。Thus, my diagnosis is low-grade epithelioid neoplasm, consistent with low-grade neuroendocrine tumor. 我的诊断是低度恶性神经内分泌上皮样肿瘤,符合低级别神经内分泌肿瘤。I post two pictures of the resection specimen of the tumor.我再把术后切除肿瘤帖上来,让大家欣赏。I feel that as pathologists, we are a important part of the patient care team, we are like director of a movie, so communication with other clinicians (radiologists, surgeons, oncologists, etc.) are very important, these communication will not only benefit clinicians and patients, but also benefit us.我感觉做为一个病理医生,我们是治疗病人团队中的重要成员,相当于一部电影中的导演,所以和临床的交流,和放射医生和外科医生和肿瘤医生的交流,都是非常我重要的。这种交流不仅有利于临床医生,有利于患者,也有利于病理医生。 Staying in your own office and just look at slides without communication and do a lot of unnecessary immunostains to get a diagnosis is not a good practice.光坐办公室死看片子,缺乏交流,做一大堆没有必要的免疫组化,得到的诊断很可能还是错误的。 For cytology, just giving a diagnosis without thinking about patient management is also very dangerous.做为细胞学报告,做出的诊断不考虑病人的处理方式和处理结果是非常危险的。 Sorry for the long message, just my thoughts.抱欠,话有点多,但是这是我心意。
听陈博士的留言都象是上课.
我们和临床医生沟通不够,这应该是国内医生的弊病,可是国内的病理科医生的地位远远没有国外的高,让我们和临床医生沟通上存在很大的局限性,这是我们在短期内都没有办法解决的.在陈博士的医院,你们的病理科医生在治疗病人的团队中占很重要的地位,甚至是主导地位,而我们,在病人和医生的心中,我们都只能算是检验医生.虽然说病理很重要,是金标准,可我们的重要性和我们在医院中的地位是不相符的.所以无论我们是在病人还是在和医生方面的沟通都很局限.不过,陈博士给我们提了一个很好的建议,我确实应该在这方面多注意!











