



| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
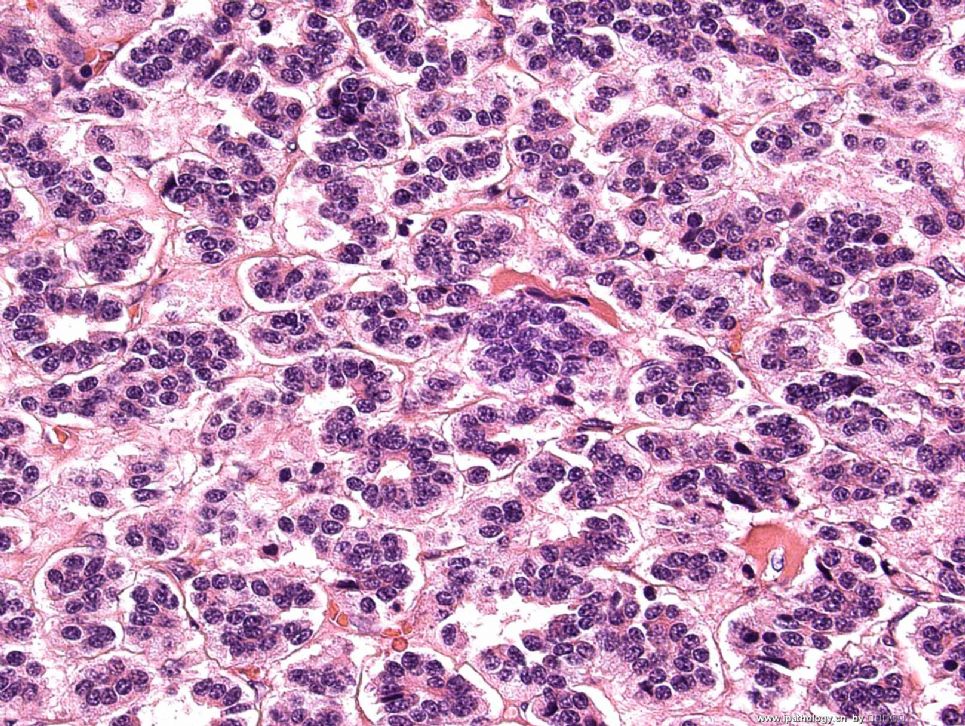
- Lung nodule FNA
 图1
图1 图2
图2
My camera was broken for some days. Have not posted any cases. Here is a recent case. A 42-year-old man with a endobronchial tumor. Broncoscope-guided FNA was done. Please see the above two posted pictures by Pap stain. I think that this case is pretty typical.
标签:
×参考诊断
低度恶性的神经内分泌肿瘤
 图1
图1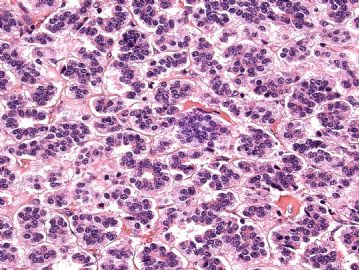 图2
图2
I am a little surprised that some people went for lymphoid lesions. Maybe, the pictures I took are not that representative. I did not think that this is a lymphoma based on 3 features: 1) The cells are very cohesive in some areas, lymphomas are usually more dispersed than this (remember these are smear pictures, not liquid-based slides); 2) I did not see lymphogladular bodies, which are usually seen in lymphoid samples; 3)some cells have more cytoplasm for lymphoid cells.
月新is right, this is a low-grade neuroendocrine tumor (carcinoid) and it is pretty classic on cytology. In our hospital, we as pathologists are regularly communicate with our clinicians to try to get the best patient care. This case, the pulmonologist talked with me before I signed-out the case and his clinical impression is carcinoid tumor too. He said to me that the clinical management of the patient will be surgical resection of the tumor as long as it is a low-grade epithelioid neoplasm. So, I felt that it is not necessary to do immunostains in this case and charge the patient unnecessary money. Thus, my diagnosis is low-grade epithelioid neoplasm, consistent with low-grade neuroendocrine tumor. I post two pictures of the resection specimen of the tumor.
I feel that as pathologists, we are a important part of the patient care team, we are like director of a movie, so communication with other clinicians (radiologists, surgeons, oncologists, etc.) are very important, these communication will not only benefit clinicians and patients, but also benefit us. Staying in your own office and just look at slides without communication and do a lot of unnecessary immunostains to get a diagnosis is not a good practice. For cytology, just giving a diagnosis without thinking about patient management is also very dangerous. Sorry for the long message, just my thoughts.
One of the posters is right on the diagnosis. I am more interested in what's your diagnosis on this case without immunostains? What if you are practise pathology in a very rural setting? no immuno lab exists?
I did NOT do any immunostain in this case, sorry I don't have pictures to share. But, I have the patient follow-up information. Thanks!











