
 (2-16-2009)图1")
 (2-16-2009)图2")



| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- B1581Breast lesions cqz (12) (2-16-2009)
 (2-16-2009)图1") 图1
图1 (2-16-2009)图2") 图2
图2
| 姓 名: | ××× | 性别: | 年龄: | ||
| 标本名称: | |||||
| 简要病史: | |||||
| 肉眼检查: | |||||
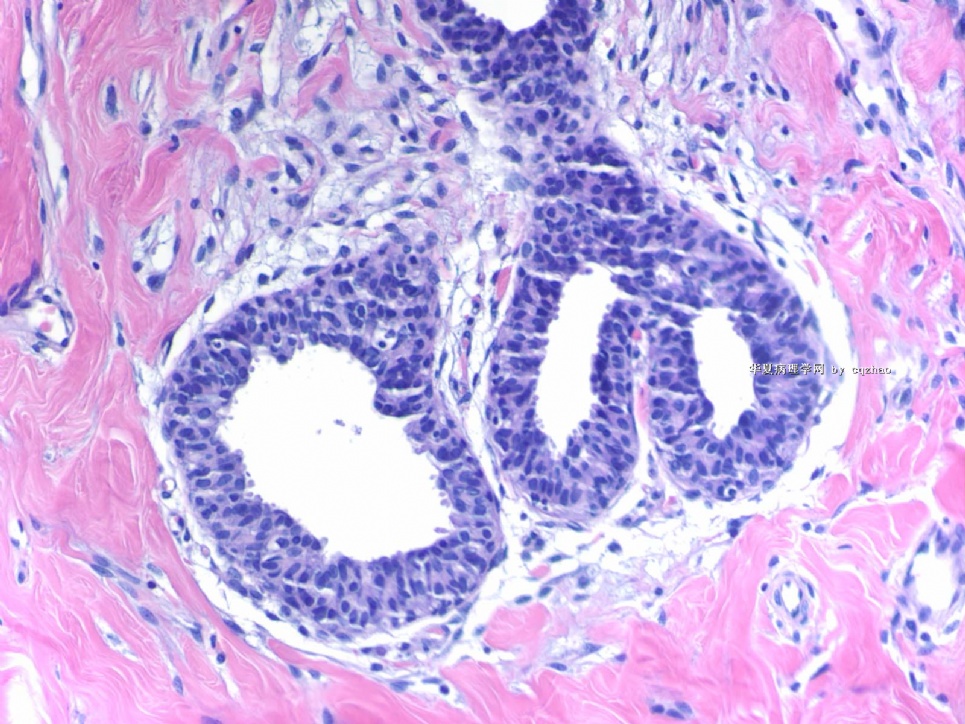
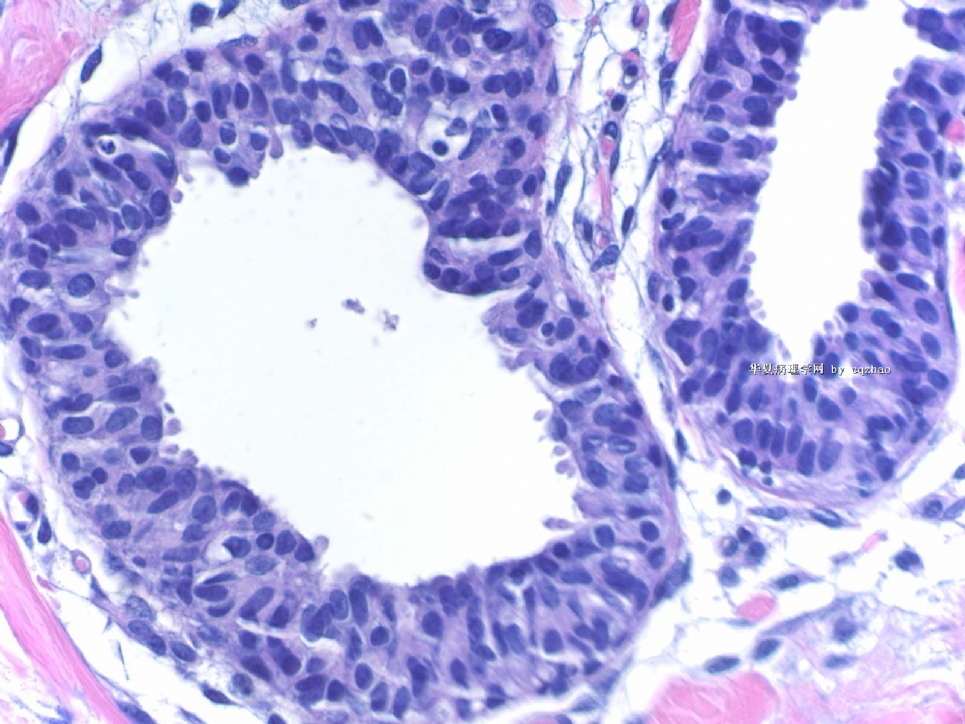
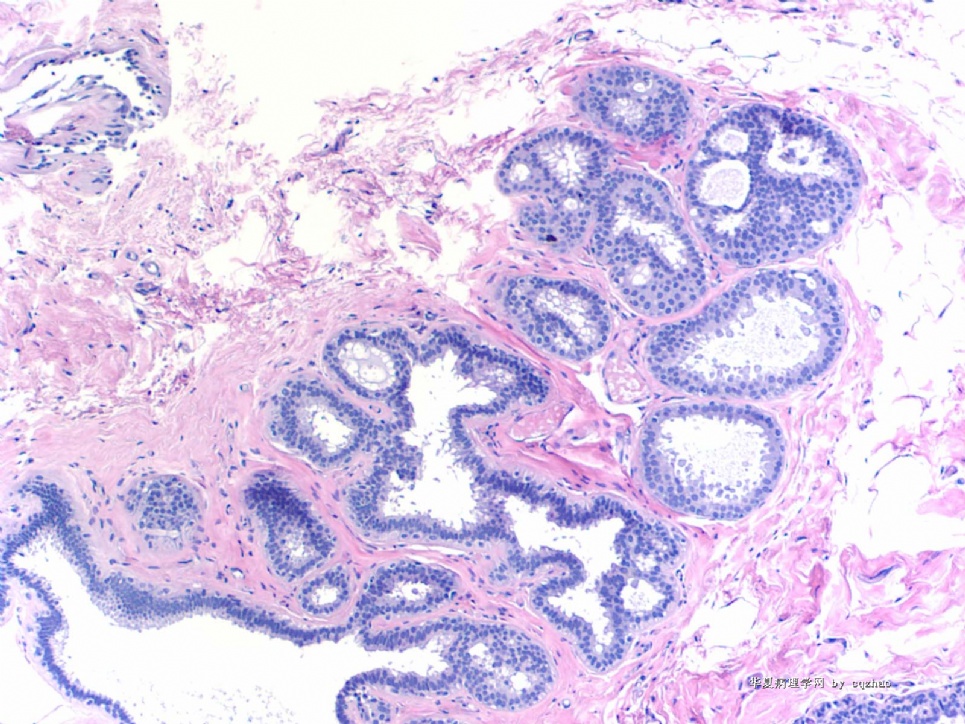
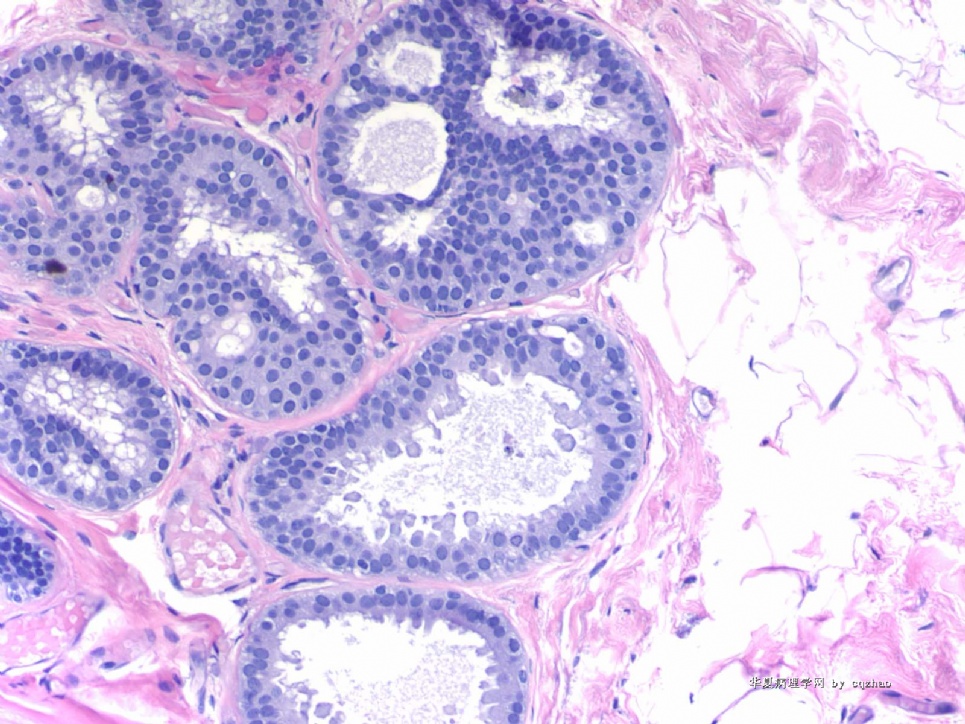
Breast core biopsy with 8 cores. There are multiple breast lesions. Try you diagnosis one by one.
Lesion 1 20x and 400x
标签:LCIS CCC FEA ADH 导管内乳头状肿瘤 放射状瘢痕
-
本帖最后由 于 2009-03-19 23:29:00 编辑
相关帖子
- • 乳腺癌?
- • 女性 冰冻为乳腺浸润性导管癌,现切除标本,肿块旁组织
- • 女性 33岁 乳腺肿块
- • 乳腺包块
- • 乳腺两个相邻导管内的病变
- • 乳腺肿物
- • 38岁乳腺(新加HE切片)
- • 乳腺包块。33岁
- • 左乳肿块,协助诊断
- • 乳腺肿物求助
×参考诊断
My last four cases:
Case 1 (floor 54) columinal cell change.
Case 2-4: all these three cases were signed out by me as flat epithelial atypia (FEA).
FEA is a debatable new term. Most general pathologists in the USA do not know this lesion well. Different pathologists can have different oppinion for the same lesion.
This is fine if you do not agree above interpretation.
Ok I will complete this topic today.
Thank you for your reading or discussing these cases.
cz
-
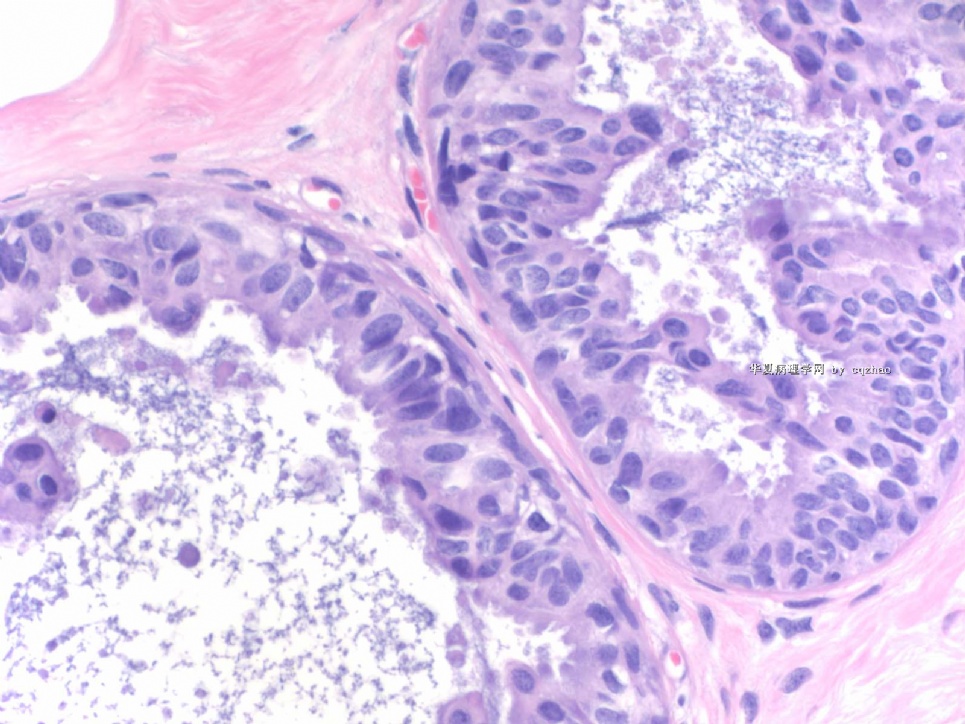
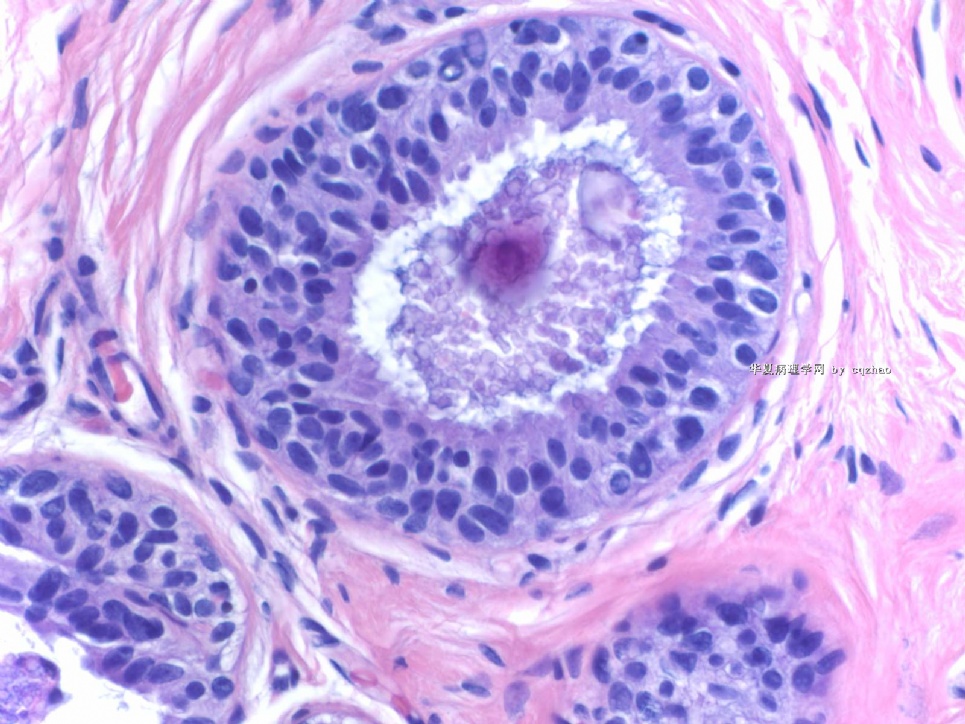
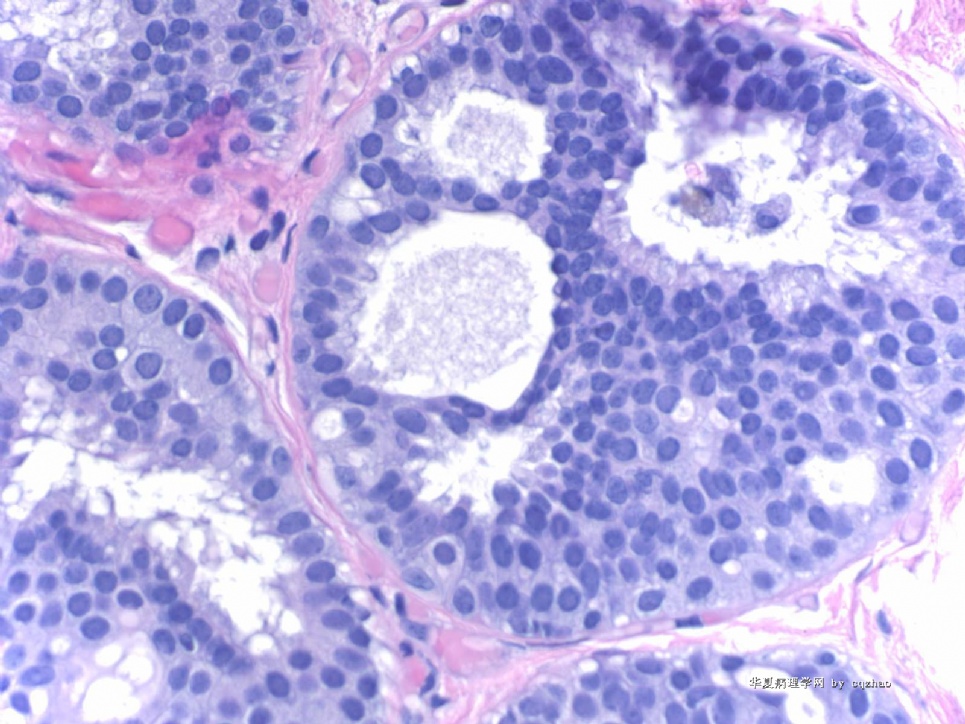
Lesion 7 demostrates focal ductal epithelial cell proliferation with uniform size in the back ground of CCC or focal FEA. It is reasonable for diagnosis of ADH. The lesion does not meet the DCIS criteria by 2-3 mm or 2-3 ducts. Hope your guys will agree.
-
本帖最后由 于 2009-03-20 02:28:00 编辑
| 以下是引用cqzhao在2009-2-17 9:21:00的发言:
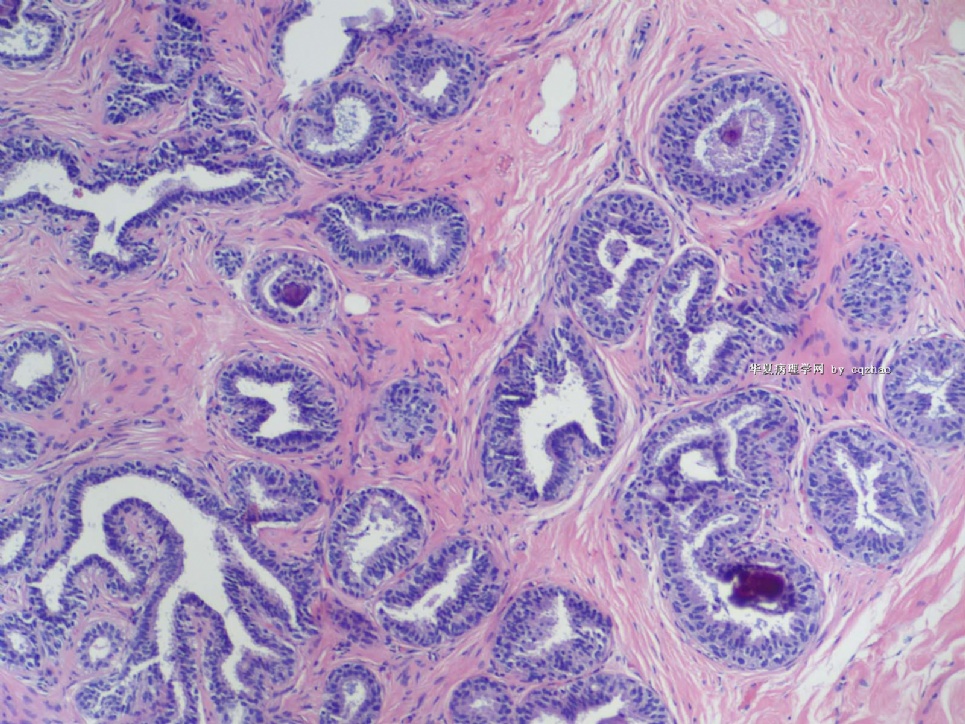
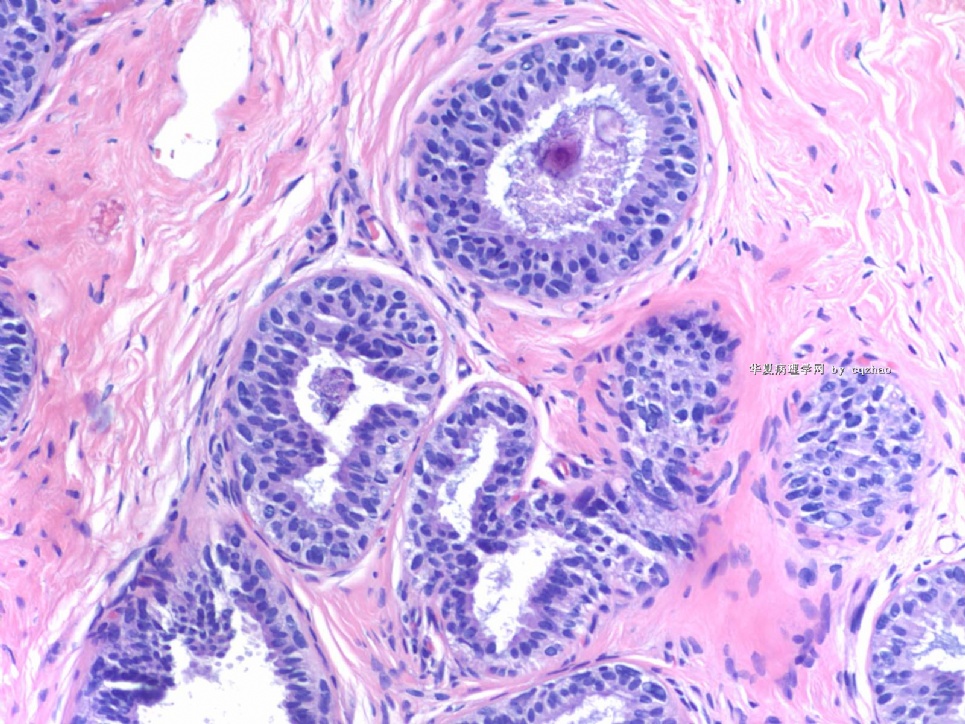
Lesion 7 Fig 1 100x Fig 2-5 200x Fig 6 400x Hope you can appreciate three diagnoses (or three terms) in this focal area. |
There are some different oppinion about this lesion. Pasted the figs again.
CCC, FEA, ADH.
Question is if the dianosis of DCIS should be rendered.
Is the severe lesion in this area ADH or DCIS?
Please share your oppinion and the reasons.
Thanks, cz
名称:图1
描述:图1
名称:图2
描述:图2
名称:图3
描述:图3
名称:图4
描述:图4

名称:图5
描述:图5
名称:图6
描述:图6
-
Lesion 3: 导管囊性扩张伴分泌物潴留 is a good call. If you call CCC it is ok. Anyway I cannot appreciate atypia here. It is not a FEA or carcinoma in situ. Compared with the photos on 41 floor we will know what is carcinoma, flat type, even though these figures are not very typical ones.
Thank Dr. Chiang' s interpretation.
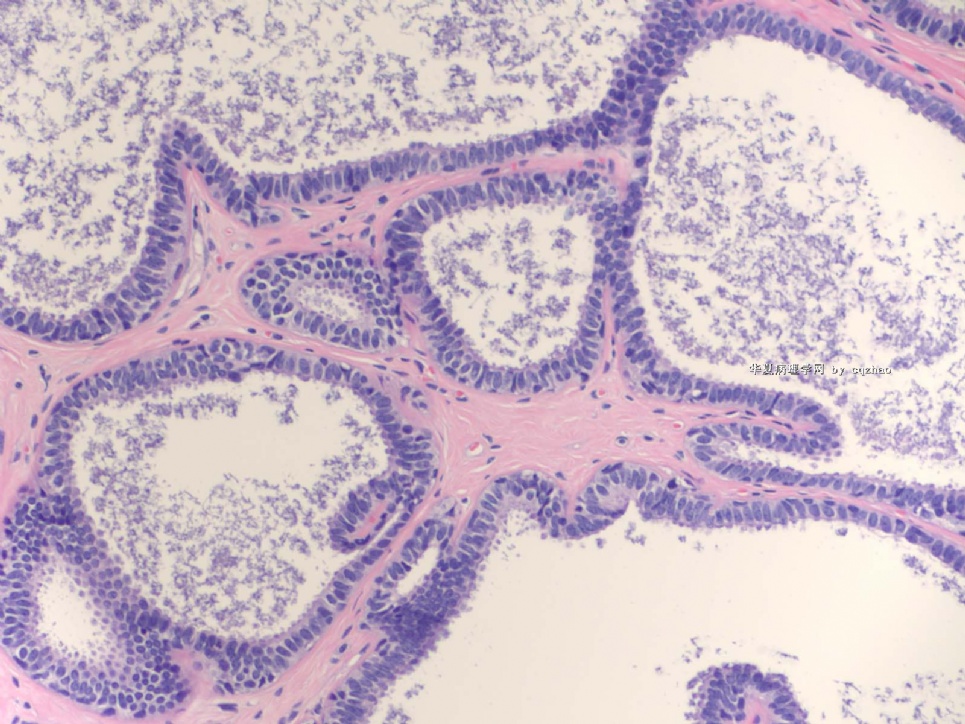
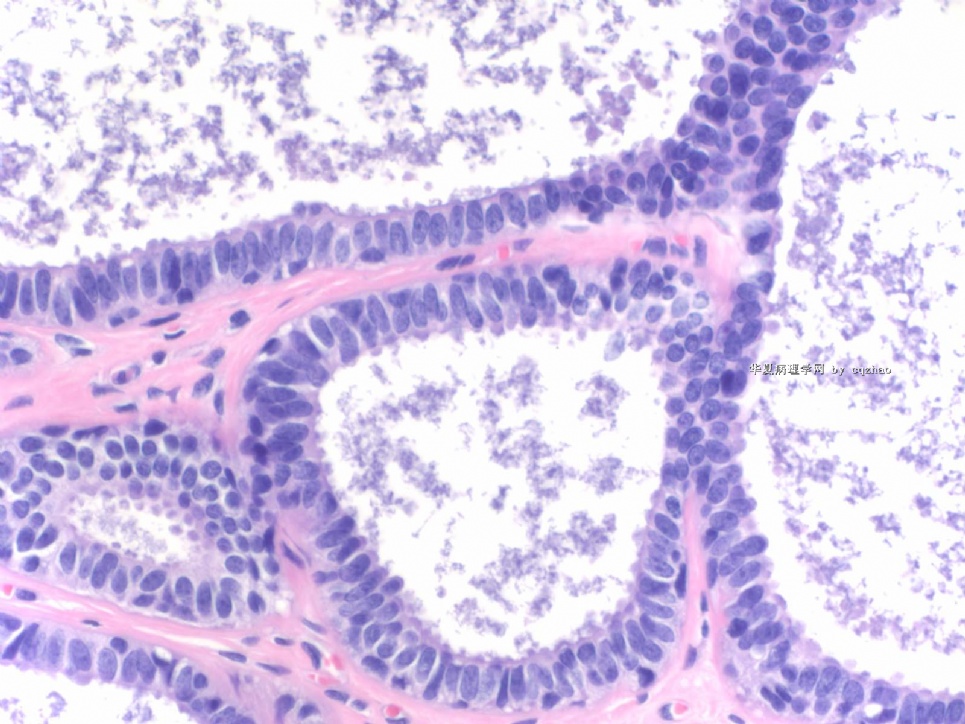
Lesion 2: Apocrine metaplasia or change with micropapaillary or papillary pattern. The nuclei are very uniform, small, evenly spaced, located the botton of the cells. I do not appreciate any cytologic atypia in this case. Cystic papillary apocrine changes are commonly seen in the breast pathology specimens. Generally people will ignorred the lesion even though mild cytologic atypia is present in the apocrine change. True atypical apocrine metaplasia is rare.
-
本帖最后由 于 2009-03-19 10:28:00 编辑
Peter Rosen is an excellent breast pathologist. His Book " Rosen's Breast Pathology in the best comprehensive book in the area of breast pathology. His calssification about columnar cell lesion is different from most others. He used the term columinar cell hyperplasia, mild, moderate, and severe atypia. I really do not like his concept about CCC. It is true that intraductal carcinoma, flat pattern, is present. However, I fell reluctant to call the 5 photos Elizabeth took from Rosen's book as carcinoma based on the photos only.
-
本帖最后由 于 2009-03-14 10:40:00 编辑
Compared Rosen fig 11.11 (page 298 in the third edition) with the above lesion 3, we can appreciate the difference in term of cytology, uniform without atypia in lesion 3 and moderate cytologic atypia in Rosen's fig 11.11.
It is very good for the disagreement. I hope more pathologists join in the diacussion.
-
Glad to see Dr. Ciang's input and diagnosis. Different interpretations were noted in lesions 2, 3, 4, and 7. Wish other share your oppinions. Also welcome Dr. Chiang to describe the reasons for the diagnoses. We can understand more by discussion. Thanks, cz
Fig 7 is a very good example showing the spectrum of CCC-FEA-ADH. Focal monotonous proliferation with cribriform pattern shows the features of ADH. Few glands surrounding the focus of ADH demonstrate atypical CCC or FEA. It is not easy to find the good area. Today I joined one day of breast long clourse. There are 8 excellent speakers (pathologists, oncologists, surgeons) from England, austrlia, the US talked about ADH, DCIS, FEA, bx, et al. There are many new and converoversial issue about breast pathology. There are also some difference between contries. I may find a time to review some talks with you in future.
Ok. You can mention your oppinion if you do not agree with my interpretation about this case.
Thanks, cz
-
本帖最后由 于 2009-03-12 12:14:00 编辑
Fig 5.
Right: CCC
Left: Clearly we can appreciate the difference ducts in the right from the right duct. If these are the only few atypicla ducts in a breast core biopsy, I will relactant to call FEA. If there are more ducts with similar features, I may call FEA.
CCC-FEA are a continuous lesion. The cut point is difficult.
Seem most of you agree the interpretation of F 1-4, 6. You can give your reasons if you do not agree.
F 5, 7involve columinar cell change, 平坦型上皮非典型性(FEA) and related lesions. FEA is a very controversial term. There are many issues which are not clear, such as dx criteria, managment: present in in core biopsy, in excisional bx, .in surgical margins. In fact even in the US, many general surgical pathologists do not know the term or do not know how to make the diagnois. Of cause most of surgens know nothing about FEA. We have alot of consult cases from other hospitals. Often we need to talk with primary pathologists. This is why I know a lot of general pathologists do not know the term well.
Interesting to know that our pathologists in China use this term or not. Please share your knowledge about FEA with ours.
Thanks











