
图1")
图2")
图3")
图4")






 I will look forward to the final answers too...
I will look forward to the final answers too... 


| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- B1760Breast LCIS involving sclerosing adenosis+ADH (cqz 11)
图1") 图1
图1图2") 图2
图2图3") 图3
图3图4") 图4
图4
| 姓 名: | ××× | 性别: | 年龄: | ||
| 标本名称: | |||||
| 简要病史: | |||||
| 肉眼检查: | |||||
I assume that all of you still are enjoying your New Year Holiday. Send here a case for your consideration.
F/50y Breast core biopsy (5 cores)
Lesion 1
Fig 1 10x
Fig 2 20x
Lesion 2
fig 3 10x
Fig 4 20x
标签:LCIS ADH
-
本帖最后由 于 2009-02-22 10:46:00 编辑
相关帖子
- • 乳腺肿物
- • 导管原位癌or不典型增生
- • 乳腺癌?
- • 女性 冰冻为乳腺浸润性导管癌,现切除标本,肿块旁组织
- • 女性 33岁 乳腺肿块
- • 乳腺包块
- • 乳腺两个相邻导管内的病变
- • 乳腺肿物
- • 乳腺包块。33岁
- • 左乳肿块,协助诊断
×参考诊断
I just play half hour of Ping ba. The lesion 2 demonstrates relatively uniform cell population, similar to low grade DCIS and focally second population of cells similar to the UDH. Some round lumens are noted. The lesion is very focal. After the lobular lesion was ruled out, ADH is a reasonable call, I think.
Lession: Breast lesions can be very complicated. They can be easily missed. We have to read the slides very carelly. We need to work out the cases (IHC, consult with others), think over and over if we are not sure.
Thank for reading the case and shared your oppinion.
cz
Agree with Dr. Elizabeth and 天山望月 .
1. LCIS involving the sclerosing adenosis, as mentioned by 漫游人 .
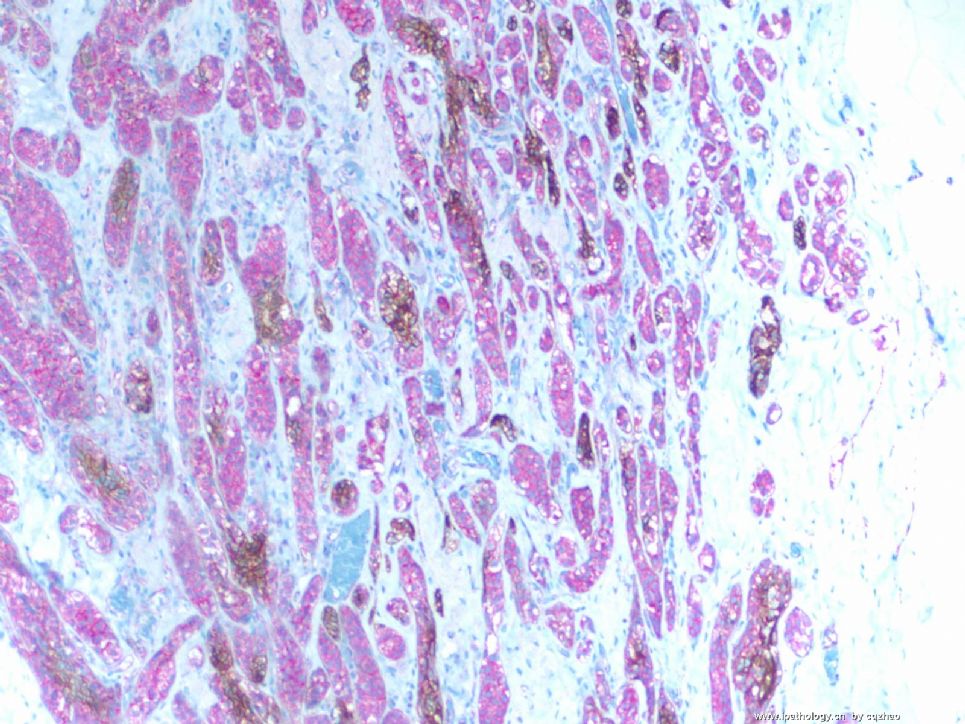
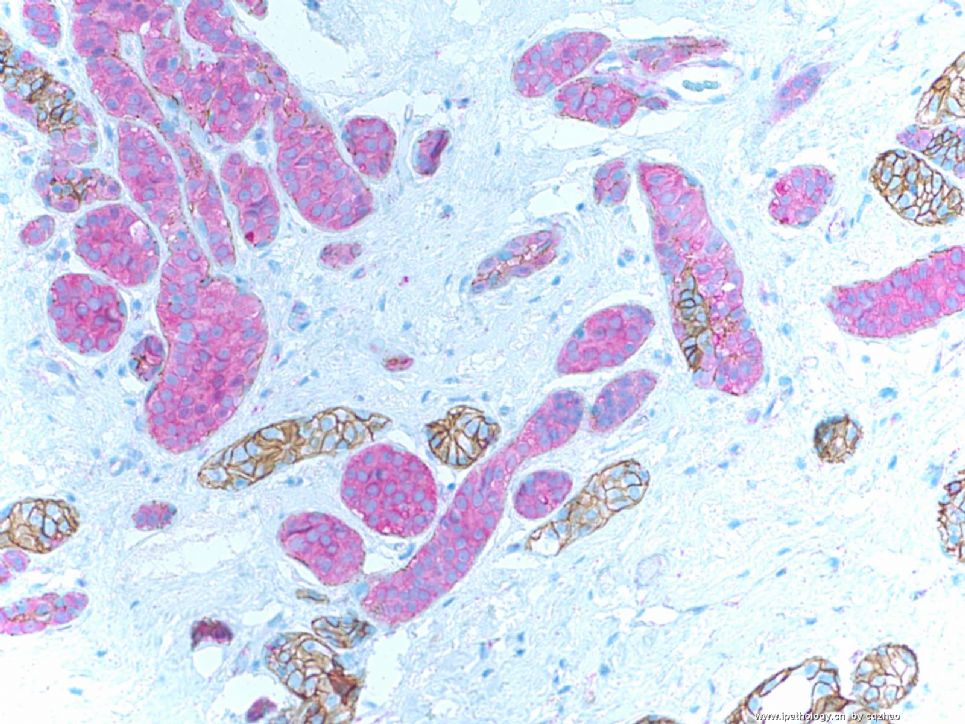
It looks like sclerosing adenosis or invasive tumor in the low power. We have to do myoepithelial stain. This is the priciple for pathologists. We must work out for these cases if we are not 100% sure of the diagnosis in clinical practice. Myoepithelial stain indicates no evidence of invasive tumor. When you observe the cells carefully especially in the high power you will notice that the cells show monotonous proliferation. We must do the stain for lobular lesion. p120 and e-cadherin stains confirm the lobular lesion.
Now the question is that it is ALH or LCIS. There are no good criteria to distingush ALH from LCIS. In this case, the lobular lesion extensively involves the sclerosing adenosis. It is better to call LCIS involving sclerosing adenosis. It is strange if we call ALH involving sclerosing adenosis.
Ok, my wife calls me to play Bing Ba ball (now. I have to observe wife's decision. I will come back to finish the discussion for lesion 2.
-
本帖最后由 于 2009-02-11 07:59:00 编辑
I reviewed above dx, differential dx and interpretation. I think most of you catch the main points.
IHC results:
Lesion 1: Fig 1-4
F1 smooth muscle myosin heavy chain
F2-4 dual stains (p120 and E-cad)
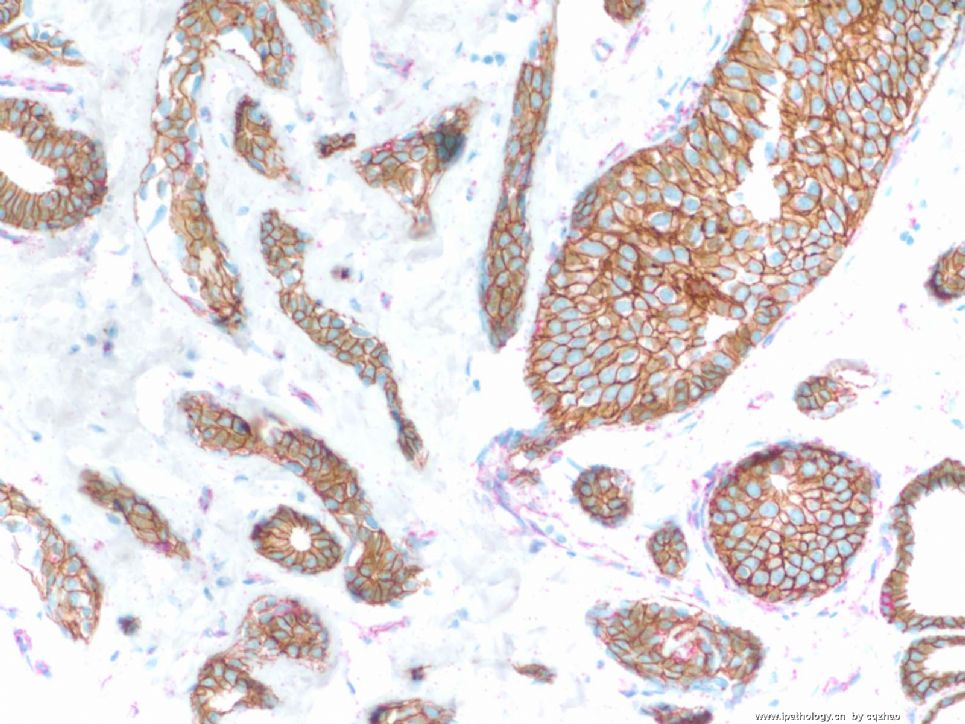
F5: dual stains for lesion 2.
Now your diagnosis please. If you are not familar with the dual stains, please check http://www.ipathology.cn/forum/forum_display.asp?keyno=111923
where I have detailed explaination.
Thanks,
cz

名称:图1
描述:图1
名称:图2
描述:图2

名称:图3
描述:图3
名称:图4
描述:图4
名称:图5
描述:图5
-
stevenshen 离线
- 帖子:343
- 粉蓝豆:2
- 经验:343
- 注册时间:2008-06-03
- 加关注 | 发消息
| 以下是引用abin在2009-2-2 23:48:00的发言:
Dr. Zhao的意思,大家以后可以直接称呼Zhao或者Dr. Zhao 这个病例很有趣,鉴别范围很广泛(不许笑话我,呵呵),包括UDH,ADH,IDC 因为不存在小叶结构,图1和图2中硬化性背景上那些模糊的小管结构和近似实性的条索,需要排除浸润癌(尽管不太像,因为可以辨认肌上皮细胞,可是……小心一些没坏处,呵呵),可以染肌上皮标记。 这例UDH与ADH的区分对我来说真的太困难了。似乎皆有(我汗,再次强调,不许笑话我)。是否还有可能ALH/LCIS累犯小叶,E-ca和p120有帮助。 期待Dr.Zhao解惑,谢谢! |
I am just a normal pathologist as your guys. I may know a little more gynecologic and breast pathology. However I almost forget all other subspecielties of pathology. You know all areas of pathology.
Most people's analyses are very reasonable. Let see if others want to join in the discussion.











