
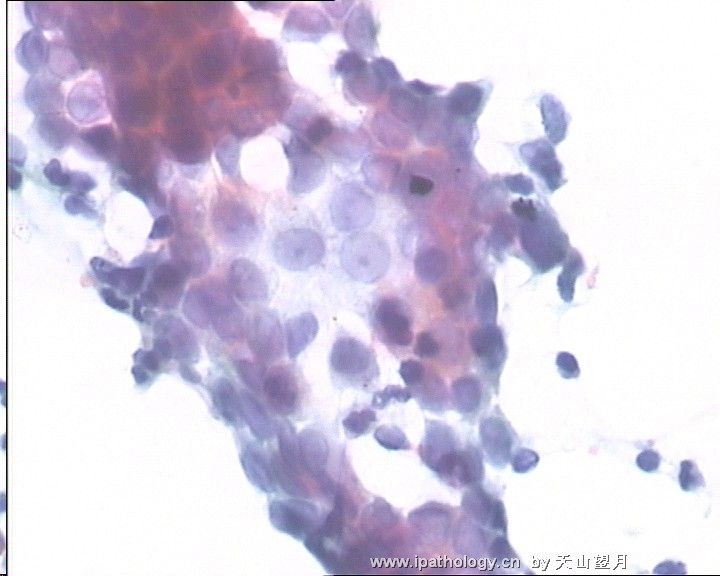
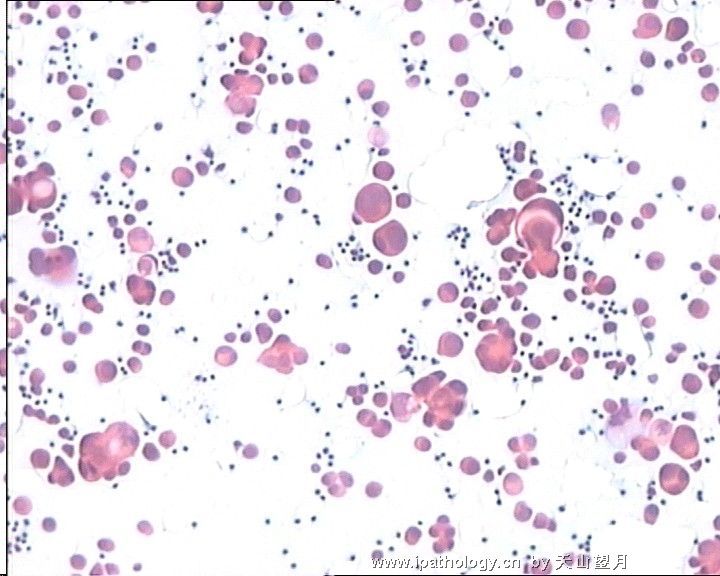
图1")
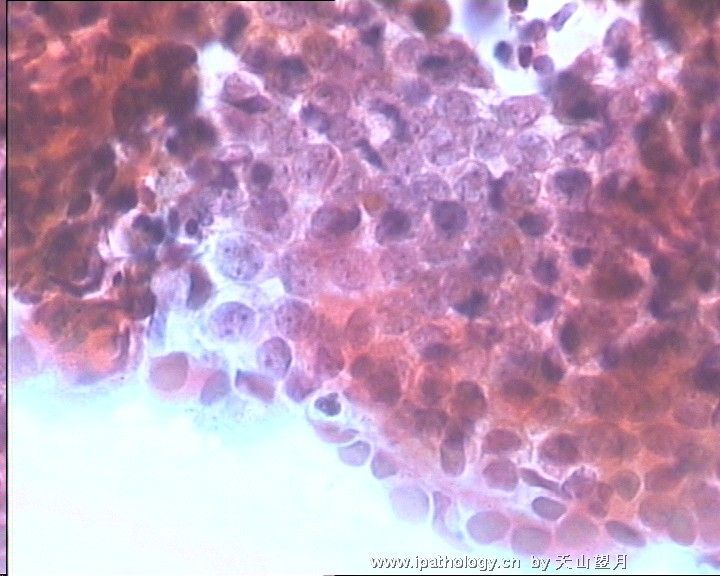
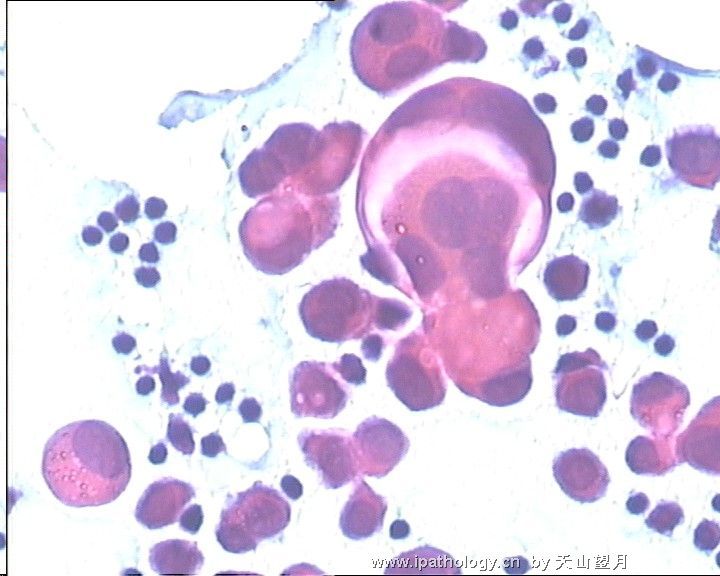
图2")
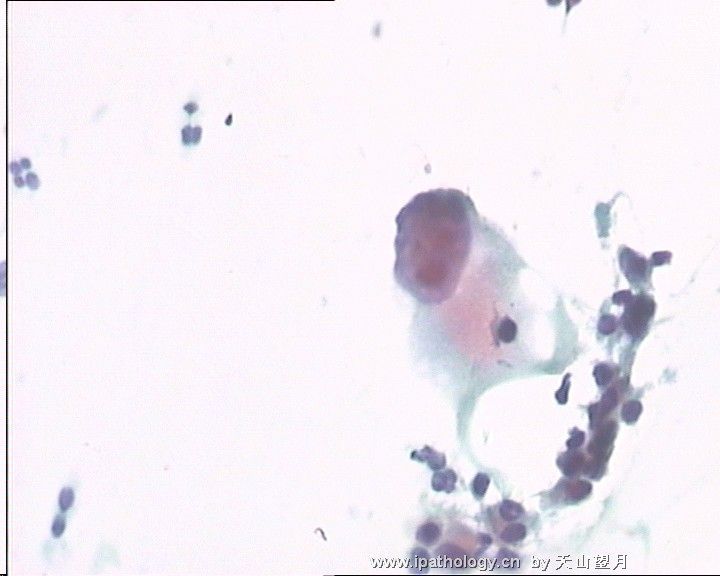
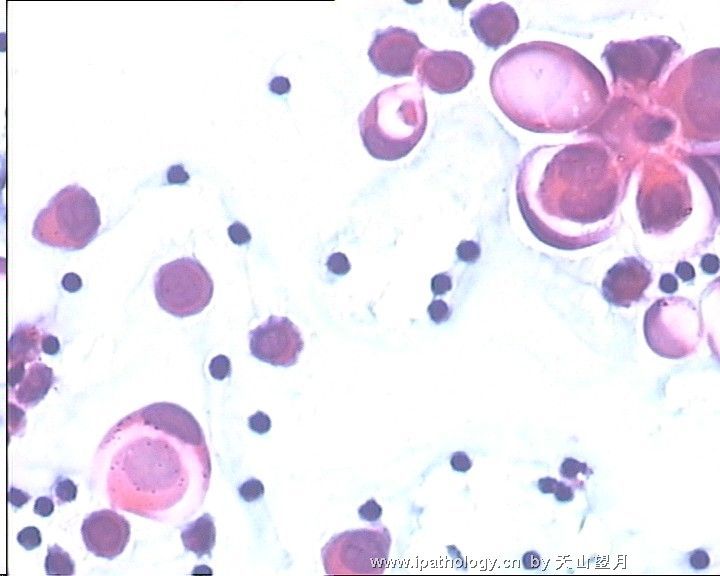
图3")
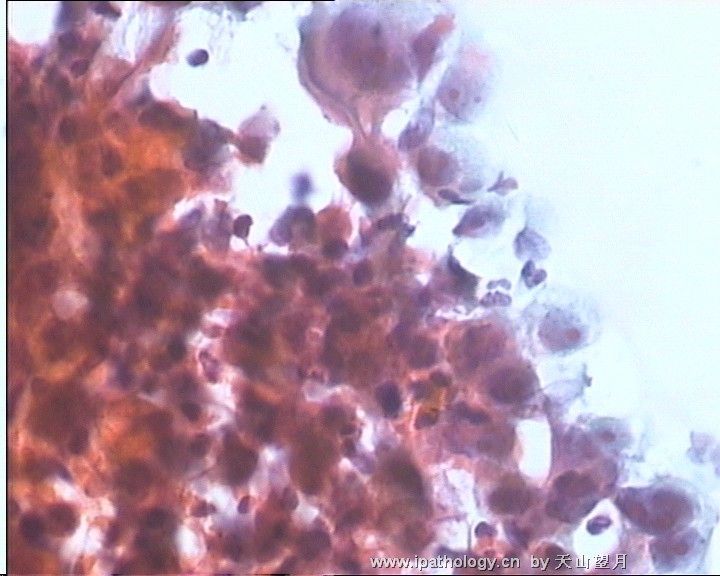
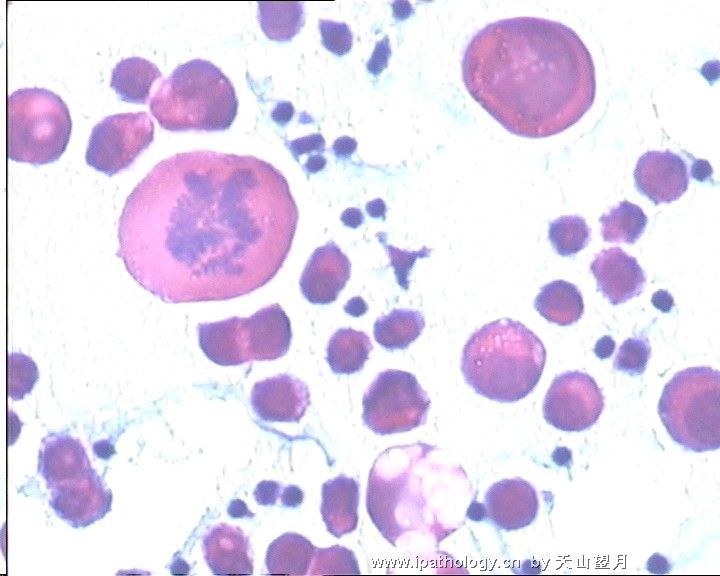
图4")










| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- 从宫颈TCT想到了什么?(更新了,请讨论)
| 以下是引用cqzhao在2009-2-1 0:41:00的发言:
Interesting case. 1. TCT showed only two abnormal cells, one with increased N/C ratio. I may call ASC-US. In the US, for most women reflax hrHPV testing will be done. I will think how to release the TCT report after I get the HPV testing result. 2. The cell block looks hypercellular, but these cells do not look very bad. I will do Ki67 and p16 stains if I am not sure. If both negative, the chance of high grade squamous lesion almost is 0 and the chance of AIS also is very low. Of cause these two antobody stains are no use for endometrial lesions. 3. The cells in pleural fluid look urgly. I am not sure they are the same cells as in the TCT. Generally I still like to do IHC for berep4 (epithelial cells) and calretine (mesothelial cells) to rule out the possibilitity of mesothelial cells. Waiting for your final result. Thanks, cz They must be malignant if they are epithelial cells. Now we need to think about the origins. In the women most common primaries are lung, GYN, breast, colon. CK7/20: lung/gyn/breast Ck7+/ck20-; colonic ca ck7-/ck20+ ER, PR for gynecologic and breast origin WT1, P53 for high rade serous carcinoma (ovary or uterus) TTF-1 for lung In most cases you can firgur out the origins. Of cause sometimes you cannot. Clinical and imaging information may be helpful. |
有趣的病例
1.TCT仅仅看到两个异常的细胞,其中一个核浆比增高。我会诊断为ASC-US.大多数女性被诊断为US后会建议她们做HPV检测。我会在看到HPV检测结果后再考虑如何发这个TCT的报告。
2.细胞团块所制片子中细胞很多,但是这些细胞好像看起来不是恶性的。如果我觉得有疑问我会标记一下Ki67和p16.如果两项都是阴性,那么高级别瘤变可能性基本为零,AIS可能性也很低。当然,这两种标记对内膜来源病变没什么帮助。
3.胸水中的细胞看起来是恶性的。但是它们是不是和TCT中的细胞是一样来源的还不敢确定,因此我会标记一下berep4和calretine看是不是有间皮细胞存在。
等待最后的结果,谢谢。
这些细胞如果是上皮来源的那么是恶性无疑了。现在的问题是找到转移来源,对女性来说比较常见的有肺,妇科方面,乳腺,结肠等。可作标记如下
CK7/20: lung/gyn/breast 肺、妇科方面、乳腺。Ck7+/ck20-; colonic ca 结肠
ck7-/ck20+
ER, PR for 妇科方面、乳腺
WT1, P53 for high rade serous carcinoma (ovary or uterus)卵巢 子宫
TTF-1 for 肺
大部分病例可以找到原发灶,当然有时候找不到。临床和影像学资料应该会有帮助。

- 赚点散碎银子养家,乐呵呵的穿衣吃饭
-
本帖最后由 于 2009-02-01 11:54:00 编辑
Interesting case.
1. TCT showed only two abnormal cells, one with increased N/C ratio. I may call ASC-US. In the US, for most women reflax hrHPV testing will be done. I will think how to release the TCT report after I get the HPV testing result.
2. The cell block looks hypercellular, but these cells do not look very bad. I will do Ki67 and p16 stains if I am not sure. If both negative, the chance of high grade squamous lesion almost is 0 and the chance of AIS also is very low. Of cause these two antobody stains are no use for endometrial lesions.
3. The cells in pleural fluid look urgly. I am not sure they are the same cells as in the TCT. Generally I still like to do IHC for berep4 (epithelial cells) and calretine (mesothelial cells) to rule out the possibilitity of mesothelial cells.
They must be malignant if they are epithelial cells. Now we need to think about the origins. In the women most common primaries are lung, GYN, breast, colon.
CK7/20: lung/gyn/breast Ck7+/ck20-; colonic ca ck7-/ck20+
ER, PR for gynecologic and breast origin
WT1, P53 for high grade serous carcinoma (ovary or uterus)
TTF-1 for lung
In most cases you can firgur out the origins. Of cause sometimes you cannot.
Clinical and imaging information may be helpful.
Waiting for your final result. Thanks, cz
-
本帖最后由 于 2009-02-01 20:55:00 编辑
| 以下是引用兰青风采在2009-2-1 12:42:00的发言: 说实话,这个主题我没有弄懂。但是楼主的工作的认真态度值得我们大家学习和借鉴。 |
呵呵,可能主题有些不明白啊,抱歉。
此例差点漏诊,所以想到了许多:
1、临床病史非常重要,开始妇科医师提供病史:宫颈糜烂,接触出血,病人仅述白带多,当地B超无异常,而查到异常细胞后,再次追问,病人有3个月子宫不规律出血,当地治疗不详。
2、如有一点异常,尤其40岁以上的病人,建议多做几项相关检查,宁愿花费多点,不能漏诊。如此,我们曾发现6例宫颈癌(在其他医院做TCT没查出)。
3、如赵博士所述,液基的残液非常有用,明显提高检出率。
- 广州金域病理











