










| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- Anterior Mediastinal FNA
-
liguoxia71 离线
- 帖子:4174
- 粉蓝豆:3122
- 经验:4677
- 注册时间:2007-04-01
- 加关注 | 发消息
-
本帖最后由 于 2009-01-06 23:01:00 编辑
谢谢陈博士! 好病例!值得推敲!
好病例!值得推敲!
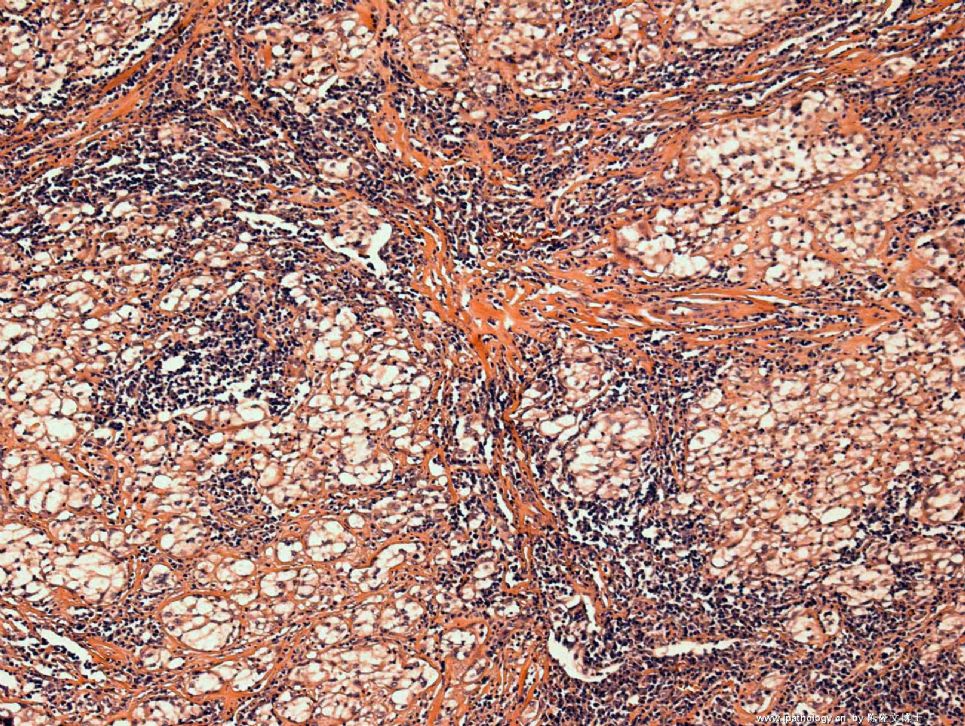
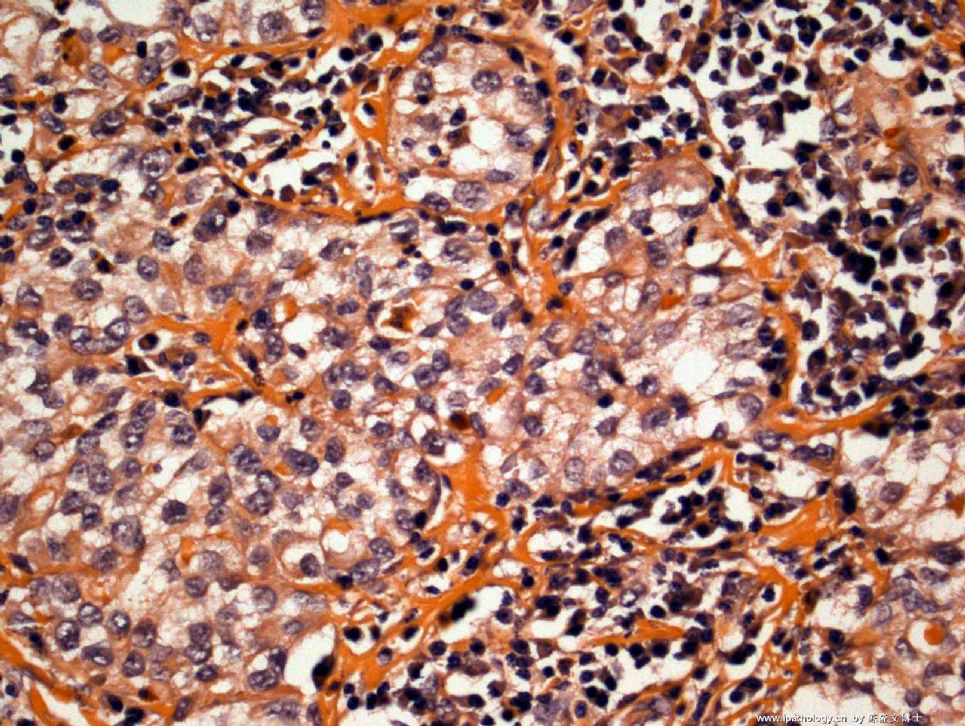
形态特点:淋巴细胞、中性粒细胞、红细胞背景上,散在、网状、镶嵌状(图3下方)排列的上皮样瘤细胞,大小不等,多边形或不规则形,胞浆丰富,红染,有胞浆突,核圆形、卵圆形,核膜不规则,核染色质稍粗,异型性明显,隐约见核仁,可见核沟、核内包涵体,易见双核、多核瘤细胞。
恶性肿瘤。根据部位、背景、上皮样细胞,考虑胸腺或淋巴结病变:1、胸腺癌?2、淋巴结转移癌(肺、甲状腺、食管等)3、淋巴瘤(大B细胞型)?4、神经内分泌肿瘤?再考虑生殖细胞肿瘤?
IHC标记:CK-pan, CK18, CK7, EMA, LCA, CD20, CD10, CD30, PLAP, TTF1, Tg, Calcitonin, Syn, CgA, Ki67
呵呵,需要太多了,可以先标记几项考虑的方向,然后再标。
不知当否?请专家赐教!谢谢!

- 广州金域病理
Those are good differential diagnosis. This was a case I was on cytology service last week and the clinician did a FNA on this 3.5 cm anterior mediastinal mass. Patient has no history of other malignancy.
I had a similar differential as yours on the rapid read. I worried that the cell block will not be enough for immunostains, I suggest the clinician to do a biopsy. On the cytology, I favor a malignant germ cell tumor.
I will keep you posted on the follow-up.
-
译上楼:Those are good differential diagnosis. 这些鉴别诊断提的非常好,This was a case I was on cytology service last week and the clinician did a FNA on this 3.5 cm anterior mediastinal mass.患者是上周我手上的病例, 临床只做了前纵隔针吸活检,包块大小为3.5CM,Patient has no history of other malignancy.患者没有肿瘤病史。I had a similar differential as yours on the rapid read. 我和大家快速读片意见一样,I worried that the cell block will not be enough for immunostains, 我担心该患者标本做出来的细胞块不足以做免疫组化,I suggest the clinician to do a biopsy. 因此我建议临床做活检。On the cytology, I favor a malignant germ cell tumor.单纯根据细胞学结果我倾向于恶性生殖细胞肿瘤。I will keep you posted on the follow-up.有了结果我继续粘帖。供大家高兴。
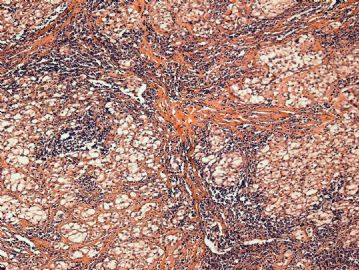 图1
图1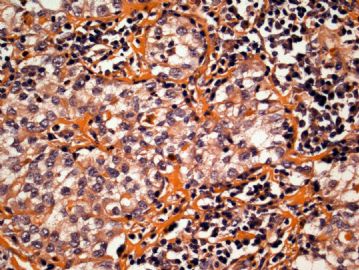 图2
图2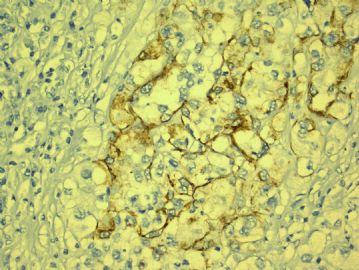 图3
图3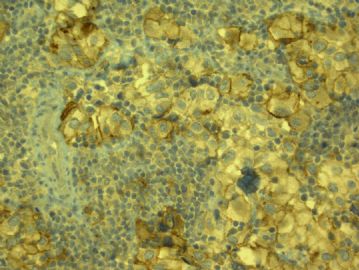 图4
图4
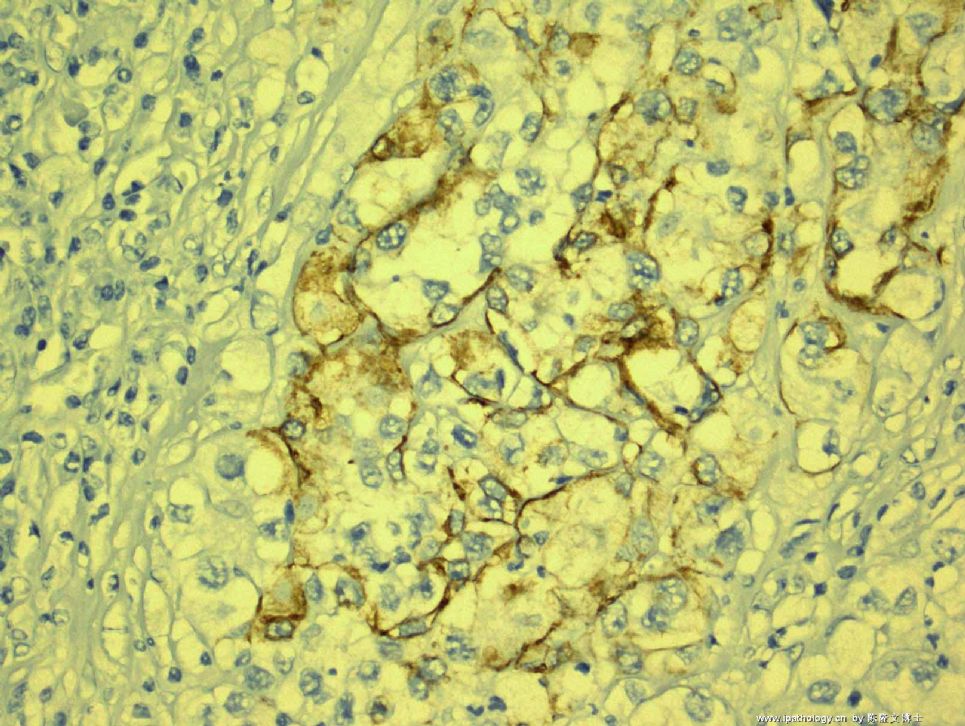
From the cytology, I think that everyone agree that it is malignant. The location of anterior mediatinum will let us think the following differential diagnosis: 1) Thymic Carcinoma; 2) Malignant lymphoma; 3) Malignant germ cell tumor; 4)Malignant thyroid carcinoma. I am glad that you are all considering the above possibility. But, remember that we most likely need immunostains to make a definitive diagnosis and sometimes, cytology has its limitation of not getting enough cells for cell block. So, in this case I asked for a biopsy. My colleague, Dr. Hansel, just brought the biopsy and a LOT OF immunostains to me. I just took some pictures and I am summarizing the immunostains:
Positive results: Only AE1/AE3 focally and CD30
Negative results: CAM5.2, TTF-1, CD20, CD45(LCA), ALK-1, PLAP, CD117,OCT3/4,bcl-2, p53, AFP.
Any thoughts on what this is?
I am surprised that now I gave you the biopsy and the immunostain results, I did not get much response. At least, I would like to know how you are going to sign-out this case???
Remember, sometimes in pathology, there is no absolute "right" or "wrong" diagnosis, it is very important to think outside the box and get the patient treated appropriately!
-
本帖最后由 于 2009-01-14 09:41:00 编辑
Quickly see the case. It is an excellent teaching case with cytology, surgical and IHC results. Few people are intrerested.
Based on the Cytologic surgical and IHC results the first year of residents In the US should know the diagnosis after reviewing the book. The second year of residents should know the diagnosis or at least which category of the tumor .
When we have problem in study, we need to check book for help.
I assume that most of pathologists in China do not systemically learn FNA cytology or seldom sign out fna cases. This may be the reason why few people here are not interested in FNA cases.
I may be wrong.
-
本帖最后由 于 2009-01-14 10:58:00 编辑
译上楼:Quickly see the case. 快速阅读本例, It is an excellent teaching case with cytology, surgical and IHC results. Few people are intrerested.该例是非常好的教学病例,但是关注的人极少。Based on the Cytologic surgical and IHC results the first year of residents In the US should know the diagnosis after reviewing the book. 根据细胞学,手术标本活检病理及免疫组化,美国第一年的病理住院医生看过病理教课书之后,都应该了解病理结果The second year of residents should know the diagnosis or at least which category of the tumor . 第二年的病理住院医生应该知道诊断结果,至少应该知道肿瘤的范围。When we have problem in study, we need to check book for help.如果有问题应该及时查书。I assume that most of pathologists in China do not systemically learn FNA cytology or seldom sign out fna cases.可能中国的病理医生没有系统学习过细针穿刺细胞学,很少签发细针穿刺病理报告。 This may be the reason why few people here are not interested in FNA cases. I may be wrong. 这就是为什么很少有人关注细针穿刺的帖子。也许我说的不对。
-
本帖最后由 于 2009-01-14 11:32:00 编辑
赵老师说的对,中国的细针穿刺病理学开展的不算广泛,就算广泛开展也好象并不入主流,许多签发细针穿刺病理报告的或许还不是病理医生,是病理技师,是细胞人员,这是非常不合理的。也是很危险的。根本没有细针穿刺病理系统训练,人人都是自学成才,或者单挑拜师学艺。话说长了,不在此展开,国家花费大量时间大量的金钱培养所谓的博士硕士,搞大量所谓的科研,给祖国医学的宝库里增添一堆堆的垃圾,根本不接触临床病理,毕业后直接当病理高级医生用,非常可怕,非常可恨,非常荒唐,但这些不是我们所能管的事情。
本例有明显的上皮样细胞,AE1/AE3 focally and CD30阳性,还有明显的淋巴样细胞,两种成份,上皮样细胞呈巢状,围绕以淋巴样细胞。考虑生殖细胞肿瘤,精原细胞瘤。
| 以下是引用陈隆文博士在2009-1-15 12:16:00的发言: It is negative for PLAP, CD117, and OCT3/4. You still think it is seminoma? |
OK! I think that everybody agrees that this is a malignant germ cell tumor. The question is how to subtype it. The immunoprofile is not for typical seminoma and it fits more for embrynocarcinoma. But, the morphology favors seminoma. My colleague (he is a very good pathologist)signed this case out as "malignant germ cell tumor, unclassifiable", I am not entirely agree with him. The ponit is that if the clinical management is no difference, then it should not matter.
I also agree with Dr. Zhao that we hope that our Chinese cytopathologists will be more proactive to participate in discussions. We as american trained Chinese pathologists working in the US are usually very busy in our daily diagnostic work and we spend our time here on the web is because we want cytopathology in China will catch up sooner than later. Thanks all for participation.











