
图1")
图2")
图3")
图4")
图5")
图6")
图7")
 浸润性导管癌
浸润性导管癌 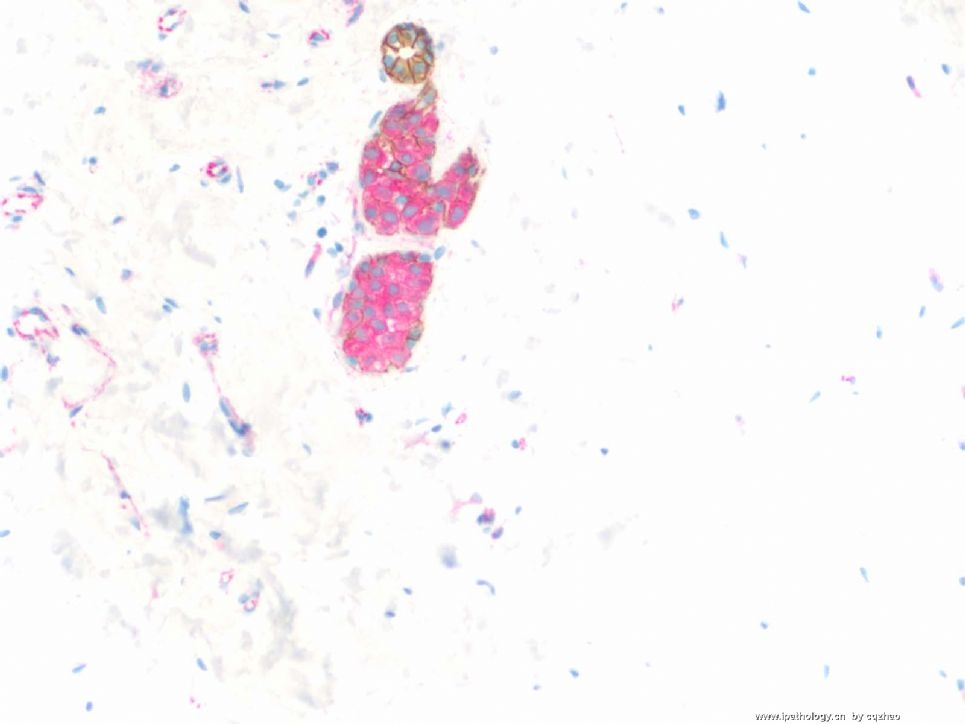
| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- Breast lobular lesions and stains ( cqz 7)
I want to complete this topic. I showed you five cases here. I hope you understand the following
1. Diagnosis of lobular lesion is important.
2. Lobular lesions, especially ALH are easy to be ignorred.
3. Sometimes dx of lobular lesions are very difficult.
4. Lobular lesions can be misdiagnosed as ductal lesions and ductal lesions can be misdiagnosed as lobular lesions too.
5. If you are not sure, please do IHC. In fact now we do IHC for most lobular lesions. Often we can see the unexpected results.
6. E-cadherin and P120 are the best antibodies for lobular lesions.
Now it is close to Chinese New Year. Hope every one has a nice New Year Holiday. I have to work on Monday, the first day of the year. The Eve of New year I will invite some of my friends in my home for a party. We can see the CCTV New Year celeberation also.
I will be very glad if the topic can provide you some information and can give some help in your clinical practice.
Thank all of you for reading and discussing this topic.
cz
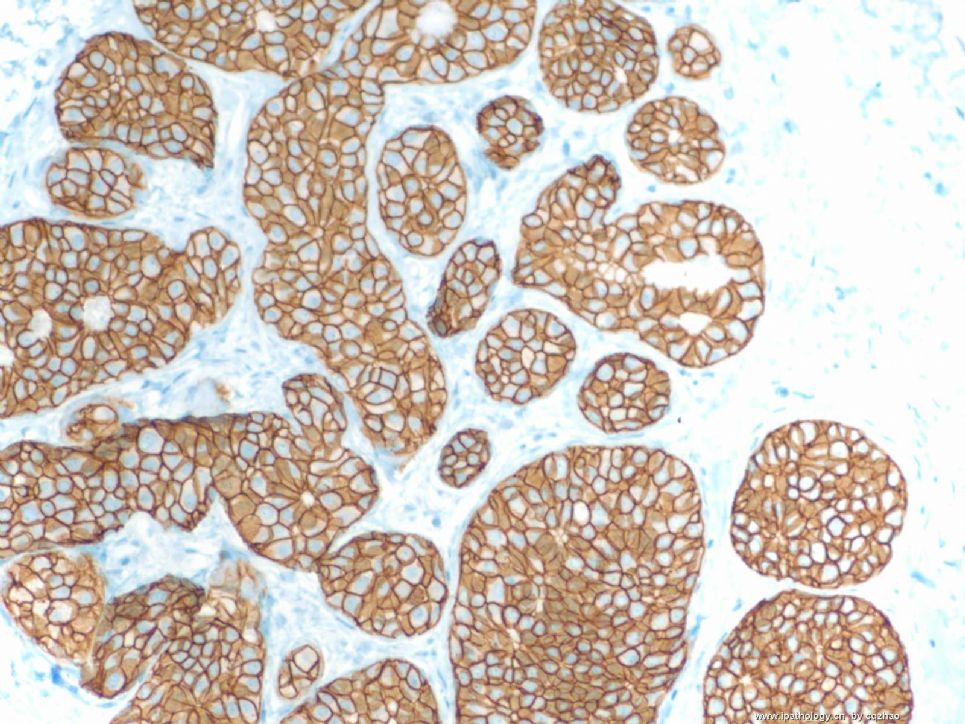
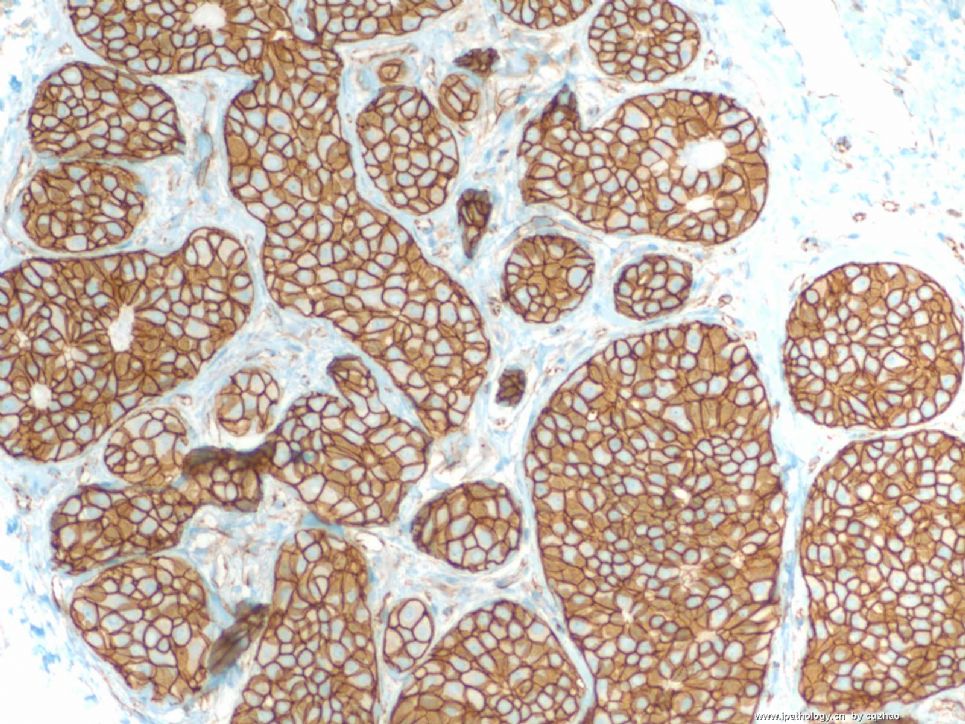
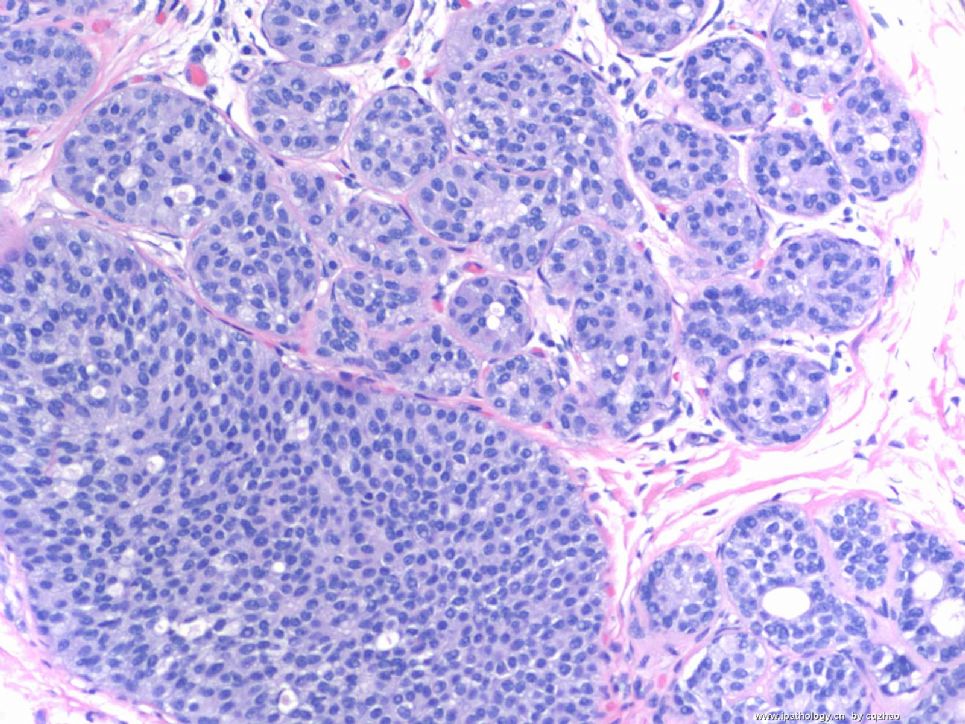
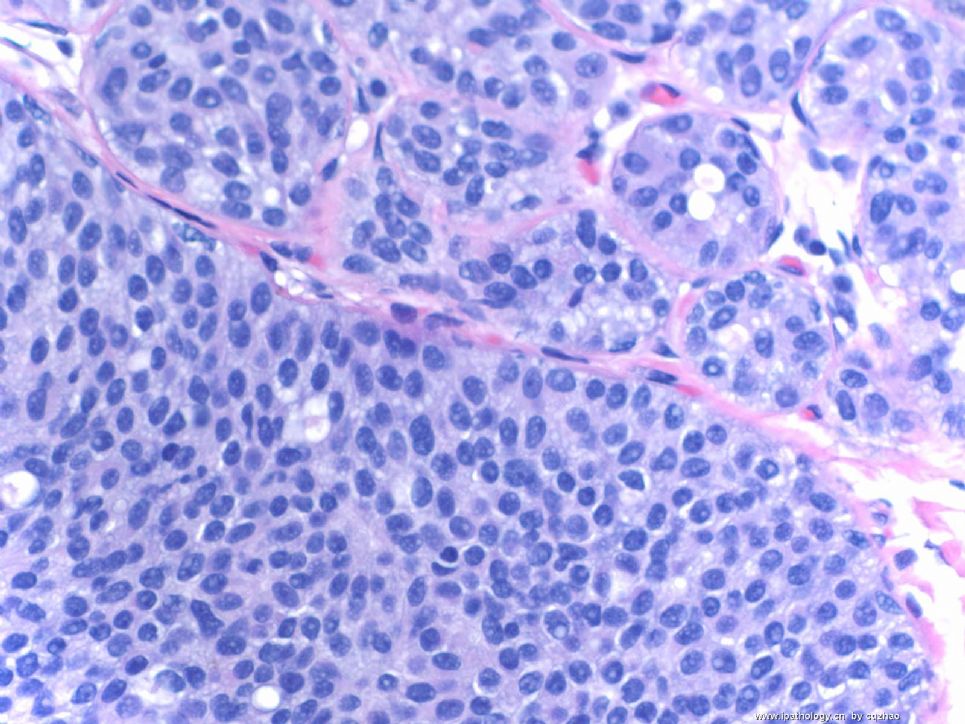
The same as most of you I first considered it was lobular carcinoma in situ in this core biopsy specimen. However, IHC results indicated it was a not lobular lesion. Now we know there are three possibilities, normal hyperplasia, ADH, and DCIS. Seeing the H&E slides more carefully, we know it is definitely abnormal. Generally the morphologic features of ADH are not like this. So only one possibility is DCIS with lobular extension or DCIS involving acini of lobules. If the specimens contain DCIS and DCIS with lobular extension, it is relatively easy to recongnize. If only lobular extension of DCIS is present in the specimen, it is difficult to make the diagnosis. But we should consider the possibility. Most of you did not consider the diagnosis. The reasons are you only see the photos, not true slides. Also the photos are not in the high power.
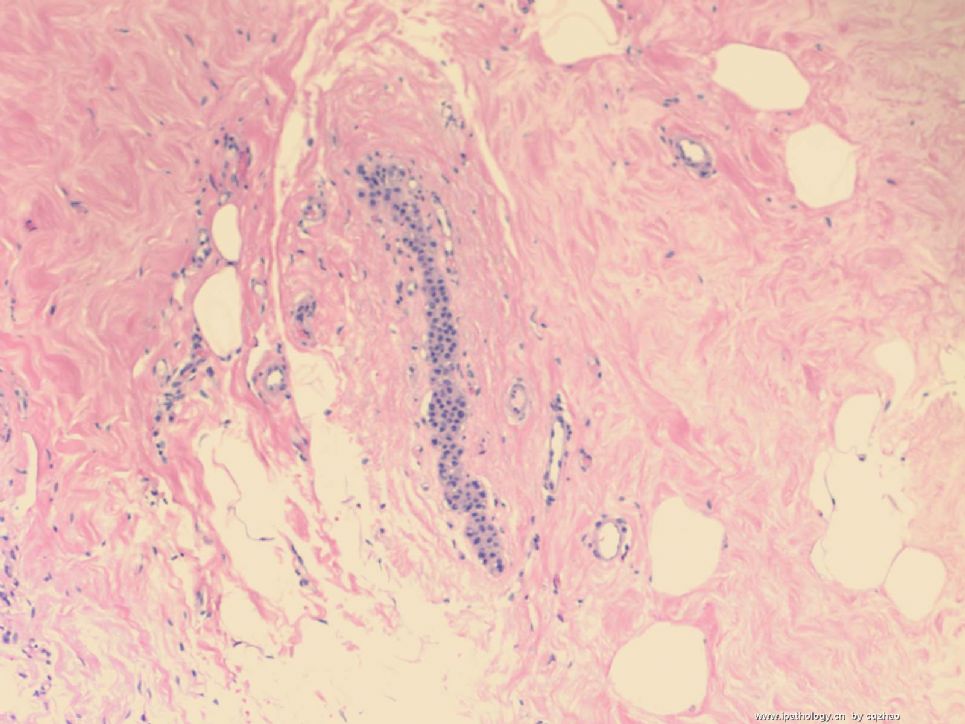
I reported lobular extension of intraductal carcinoma. The women had segmental mastectomy. The mastectomy specimen showed the DCIS closely to the previous core biopsy area.
This is for this case. Thanks.
-
本帖最后由 于 2008-12-27 12:12:00 编辑
For 天山望月 's beautiful flower, I took photos from one of my today's cases and sent here.
F1 100x
F2 200x
F3 400x
Middle aged women with core biopsy due to the abnormal mammogram imagines. Only lesion in three cores showed in the photos.
What do you think?
名称:图1
描述:图1
名称:图2
描述:图2
名称:图3
描述:图3
-
本帖最后由 于 2008-12-24 19:43:00 编辑
I am doing breast core biopsy service this week. Give you another example of very focal ALH from my today' s cases.
Just hope whoever read this topic from this web can think about the lesions in your practice. Do stains if you are not sure.
We should learn some priciple from the case study, but not only one case interpretation.
这周我做乳腺粗针穿刺活检。从我今天的病例中提供另一例非常局灶性的ALH。
希望看过这个主题贴的人在实际工作中能够考虑到这种病变,如果不确定,做免疫组化。
我们应该从病例学习中学到一些原则,而不只是一个病例解读。
____abin译
名称:图1
描述:图1
名称:图2
描述:图2
-
本帖最后由 于 2008-12-24 19:40:00 编辑
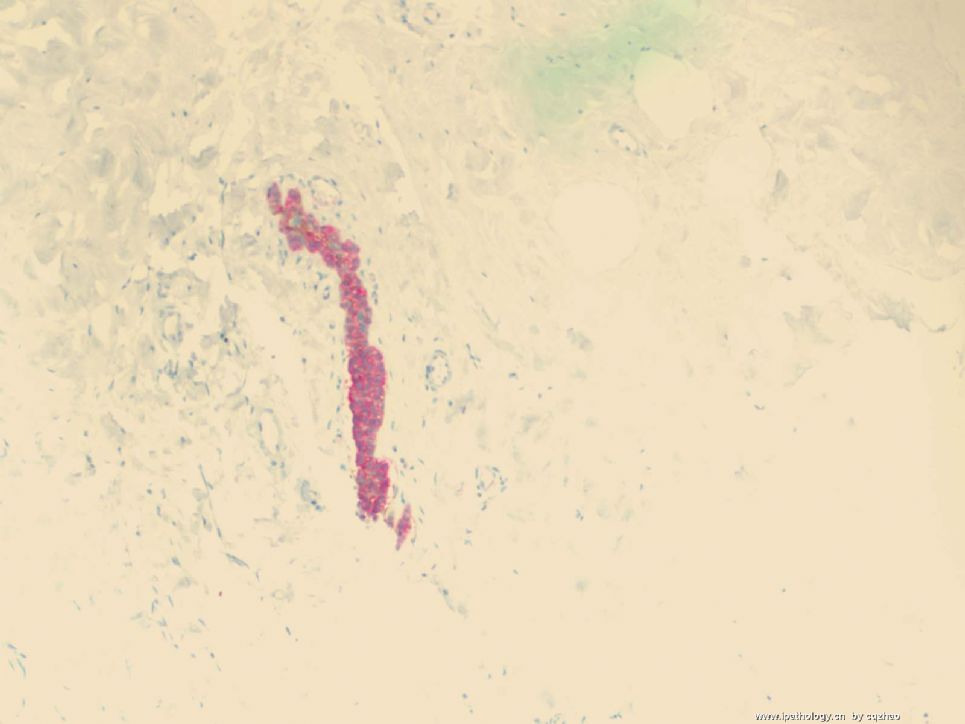
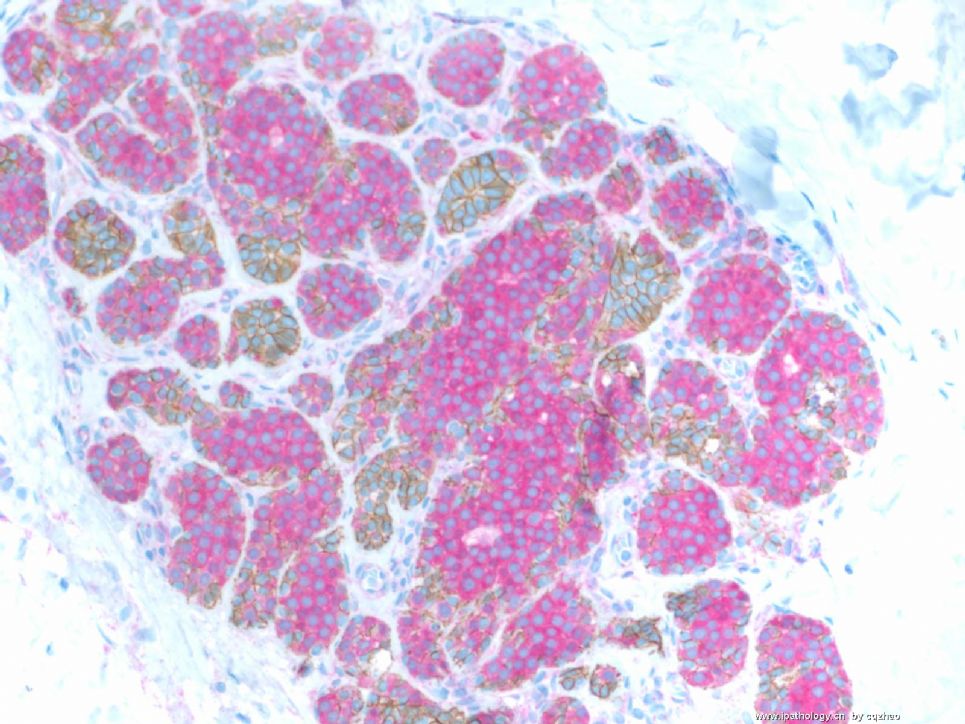
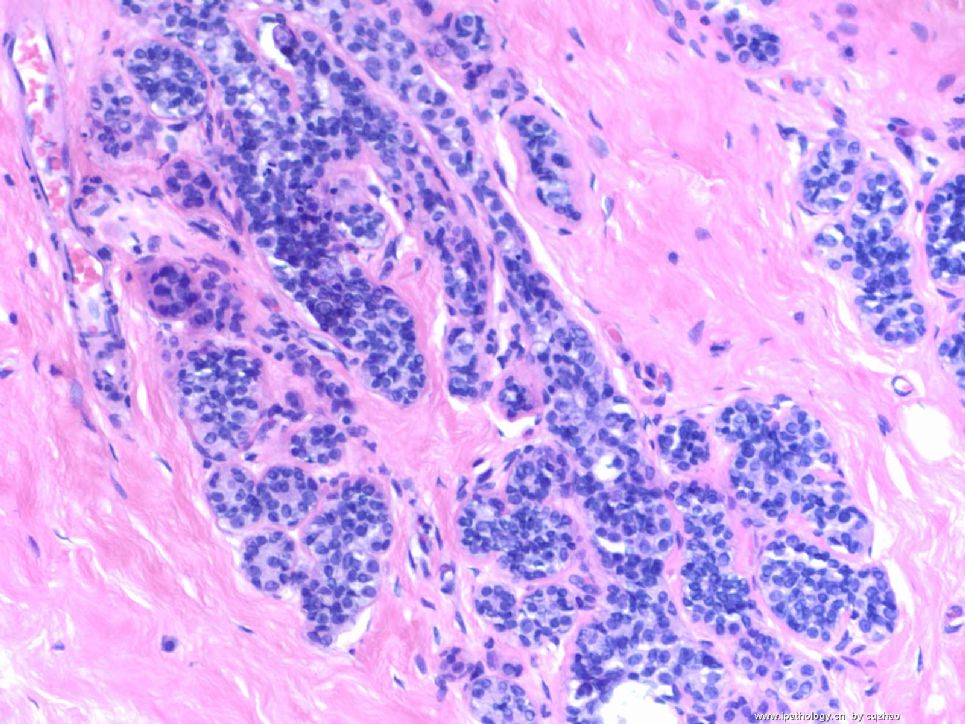
Dual stain (p120 and e-cad) for above case
Clearly it is ALH lesion. The H&E morphology is very minimal. It is very easy to be missed for every one.
ALH is the risk factor of cancers. Women can have more close follow up it we can diagnose the lesion, or excisional biopsy for women with core biopsy.
Can you say you never miss the samll lesions? This is why stains are important sometimes. I remember that we once had argument if stains are needed for lobular lesions in this web.
上述HE图片的IHC双标(p120 and e-cad)。
这是明确的ALH。HE形态学很微小。每个人都容易漏诊。
ALH是进展为浸润性乳腺癌的危险因素。如果诊断了这个病变,患者需要更密切随访,或粗针穿刺活检后作切除活检。你能说从未漏诊过这种微小病变?这就是为什么有时IHC非常重要的原因。记得我们曾经在这个网站上争论过小叶病变是否需要IHC。
____abin译
名称:图1
描述:图1
45 y female for bilateral breast reduction:
Breast reduction is a surgery procedure, not a disease. Some women's breasts are large. They ask the surgeons to take out some of normal breast tissue to make their breast smaller for purpose of beauty. it is a kind of plastic or cosmetic surgery. Breast reduction is opposite of breast augmentation.
-
本帖最后由 于 2008-12-21 22:15:00 编辑
Put here another case.
45 y female for bilateral breast reduction (about 900 grams for each side).
One section as the photo.
Our rule for breast reduction age 40 or above:
10 sections are submitted for microscopic examination for each side.
What do you think? How will you deal with this case?
名称:图1
描述:图1
| 以下是引用abin在2008-12-21 1:31:00的发言:
我理解的分级: ALH-LCIS:明确的小叶病变,一个TDLU内一半以上的腺泡被累及(充满且扩张,中央无腔隙),为LCIS。不足一半的腺泡被累及,仅部分充满腺泡,无或仅有轻度扩张,为ALH。LCIS不分级。 LIN 1,2,3级(Bratthauer GL, Tavassoli FA, 2002):1级相当于ALH,2级相当于LCIS,3级:增殖的细胞完全充满并使末梢导管最大限度地扩张到几乎相互融合,或增殖的细胞有明显异型性(多形细胞型),或增殖的细胞完全由印戒细胞组成(印戒细胞型)。多形细胞型和印戒细胞型可出现坏死和钙化,这两型不要求腺泡明显扩张。 |
Agree with Abin. The most common differential diagnostic dilemma is the distinction of LCIS from ALH. There are many authories who gave the different criteria. It is difficult to handle it. It is more difficult than in distiction ADH from DCIS. You need to get some sense from your own experience and also consider the patients' situation, core biopsy or excisional biopsy et al.
In fact I like LIN system. It is more easy to make dx for pathologists. LIN1 and 3 are easy. If you are not sure, than call LIN2. I learned LIN when I worked at AFIP. But Magee does not it. Tavassoli FA once was Chair, Gyn/breast dept at AFIP. This is why LIN is used at AFIP. Tavassoli is in Yale. She still give talk in national meeting using LIN system. Basically most hospitals still use ALH-LCIS system. Importance is that your physicans know what you are talking about.
LIN1 should ALH
LIN3 should be LCIS
LIN 2 can be alh or lcis.
it seems that I only discuss cases with few good pathologists in China. It is fine for me. Ha, ha.
-
本帖最后由 于 2008-12-23 23:05:00 编辑
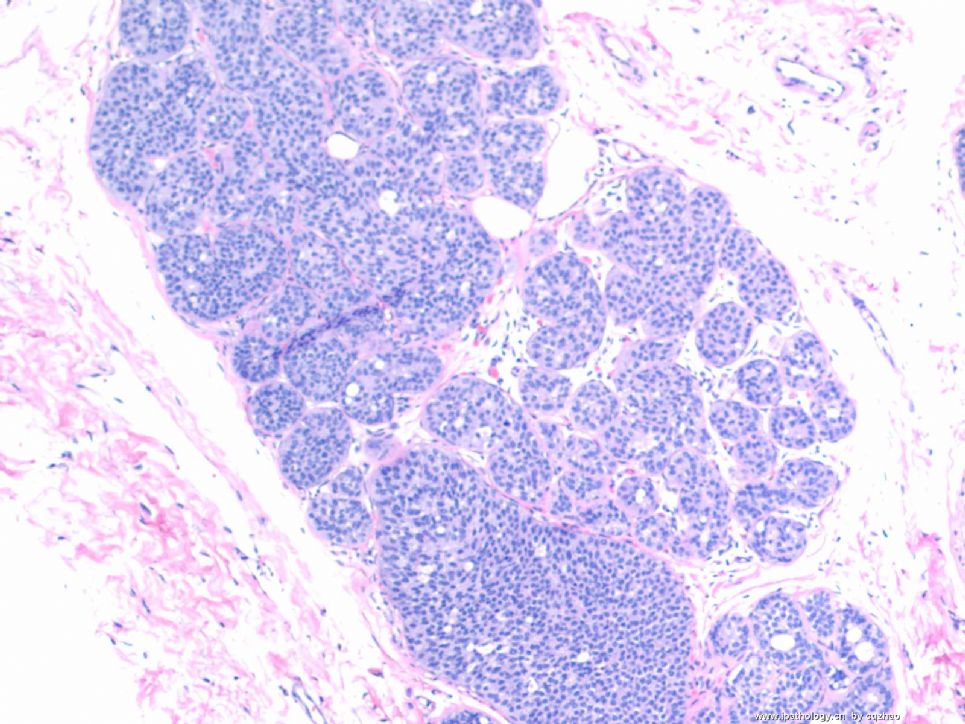
For the women younger than 40 with breast reduction we submit 4 slides each side for microscopic examination. This photo shows focal atypical proliferation. We always order IHC for this kind of lesions. Based on morphology it may be a lobular lesion. If they are not lobular lesion, they are normal ducts. In US, there are two different systems for lobular lesions.
1) ALH-LCIS
2) lobular neoplasia 1, 2, 3
Now most people use ALH-LCIS system.
the lesion is very small. It should ALH, not LCIS.
The reasons I put here for this case are
A. For small lesion as above E-cad or/p120 should be performed to confirm the nature of lobular lesion.
B. We should submit more sections if we confirm it is lobular lesion. We generally submit another 10 sections for breast reduction specimen. Remember that ALH or LCIS is a risk factor for cancer.
abin译:
对于40岁以下妇女的乳房缩小手术标本,我们每侧取4张切片作镜下检查。图示局灶性不典型增生。这种病变我们通常要做免疫组化。根据形态学,它可能是小叶病变。如果它们不是小叶病变,就是正常导管。在美国,小叶病变有两种不同的分类系统:
1)ALH-LCIS(不典型小叶增生-小叶原位癌)
2)小叶瘤变 1,2,3级
现在大多数使用ALH-LCIS系统。
病变很小,应该是ALD,而不是LCIS。
我提供这一例的目的:
A、小灶病变应该做E-cad or/p120 以确定小叶病变的性质。
B、如果确定它是小叶病变,应该更多取材。对于乳房缩小标本我们一般再取10块组织。记住ALH或LCIS是进展为癌的危险因素。











