以下是引用xljin8在2010-2-7 7:31:00的发言:
Dr.Chiang 提出外周性血管母细胞的诊断非常好,我检索了PubMed 有三篇报道,供大家参考:
1. Patton
KT, Satcher RL Jr, Laskin WB.Capillary
hemangioblastoma of soft tissue: report of a case and review of the literature.
Hum Pathol. 2005;36:1135-9.Department
of Pathology, Feinberg School of Medicine, Northwestern University, Chicago, IL
60611, USA.
Capillary
hemangioblastoma (CH) is a tumor of unknown histogenesis that arises primarily
in the posterior cranial fossa, either as a sporadic event or in association
with von Hippel-Lindau disease. To date, only 6 examples of a tumor with
morphological features of CH arising in the somatic soft tissues have been documented
in case reports and small series, and 3 of these tumors were associated with a
peripheral nerve. Herein, we report a case of CH arising in the gastrocnemius
muscle and not associated with a peripheral nerve in a 53-year-old woman with no clinical stigmata or family
history of von Hippel-Lindau disease.
2. Michal
M, Vanecek T, Sima R, Mukensnabl P, Boudova L, Brouckova M, Koudepa K. Primary
capillary hemangioblastoma of peripheral soft tissues. Am J Surg
Pathol. 2004;28:962-6.Department
of Pathology, Faculty Hospital, Pilsen, Czech Republic.michal@medima.cz
A case of
capillary hemangioblastoma located in the peripheral soft tissue of the inner ankle
in a 74-year-old woman is presented. The tumor was an unencapsulated but sharply
circumscribed nodule 2.5 cm in size, of a yellow-white color. It showed
reddish-brown spots with small cysts up to 2 mm filled with blood. Grossly the
tumor was not attached to any peripheral nerve. Signs of von Hippel-Lindau's disease
were excluded by thorough clinical evaluation. No additional tumor or erythrocytosis
was found in the patient clinically. Immunohistochemically, the tumor stromal
cell reacted strongly with antibodies to S-100 protein, NSE, and calponin and
they were negative with antibodies to GFAP, CD34,CD31,cytokeratins, actin,
desmin, EMA, and HMB-45. Endothelium of the capillaries reacted positively with
antibodies to CD31, CD34, and Factor VIII-related protein. Capillary pericytes
were actin-positive. All cells of the tumor stained positively with antibody to
vimentin. MIB1 antibody reacted only in very few cells (<1%).
Ultrastructurally, the stromal cells contained electron lucent cytoplasm with
lipid droplets, a small amount of rough endoplasmic reticulum, and glycogen particles.
No electron-dense structures typical of secretory granules were seen in the
stromal cells. No mutation of coding sequence of VHL gene was found.
3. Fanburg-Smith
JC, Gyure KA, Michal M, Katz D, Thompson LD.
Retroperitoneal
peripheral hemangioblastoma: a case report and review of the literature.
Ann Diagn
Pathol. 2000;4:81-7.
Department
of Soft Tissue Pathology, Armed Forces Institute of Pathology,Washington,
DC 20306-6000, USA.
Central
nervous system hemangioblastomas are uncommon tumors of controversial etiology
that are usually found in the posterior fossa of the cranial cavity,retina, and
spinal cord. Peripheral involvement is rare; only isolated case reports
have been identified. We report an unusual case of hemangioblastoma involving
the retroperitoneum. A 47-year-old African-American man presented with polycythemia
on routine laboratory testing. Computed tomography revealed a large retroperitoneal
mass near the pancreas, in a left suprarenal location, without adrenal
involvement and without attachment to a nerve. Although hemangioblastoma may be
associated with the von Hippel-Lindau syndrome, this patient did not have any of the
stigmata of this disease. The
histologic features included a highly vascular tumor with cellular areas
composed of plump, pleomorphic spindled and epithelioid (stromal) cells with
variable cytoplasmic lipid vacuoles and hypocellular areas with inflammatory
cells and collagenous fibrils. Immunohistochemical staining showed that the
tumor (stromal) cells were positive for vimentin, calponin, S-100 protein,
neuron-specific enolase, and CD57 and negative for glial fibrillary acidic
protein, cytokeratins, epithelial membrane antigen, CD34, HMB-45, desmin, and
the actins. These morphologic and immunohistochemical
findings are consistent with hemangioblastoma. To our knowledge this is the
first reported case of a hemangioblastoma in this location.Based on this case
we conclude that hemangioblastoma may occur in the retroperitoneum and outside
of the central nervous system in a patient without von Hippel-Lindau syndrome. The immunoprofile of this case suggests
that hemangioblastomas are mesenchymal neoplasms exhibiting both neural and myofibroblastic
differentiation.  ![]() onmouseout="this.style.opacity=0.5" onmouseover="this.style.opacity=1" style="opacity: 0.5; cursor: pointer; left: 1px; position: absolute; top: 0pt;" src="file:///C:/Users/XIAOLO~1/AppData/Local/Temp/msohtmlclip1/01/clip_image002.gif" alt="" /> onmouseout="this.style.opacity=0.5" onmouseover="this.style.opacity=1" style="opacity: 0.5; cursor: pointer; left: 1px; position: absolute; top: 0pt;" src="file:///C:/Users/XIAOLO~1/AppData/Local/Temp/msohtmlclip1/01/clip_image002.gif" alt="" />
|























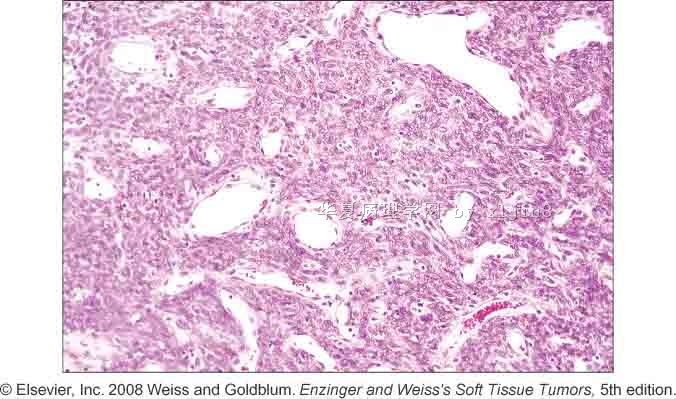


 图1
图1










