















| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- Share an interesting Pap smear
-
本帖最后由 于 2009-01-08 07:06:00 编辑
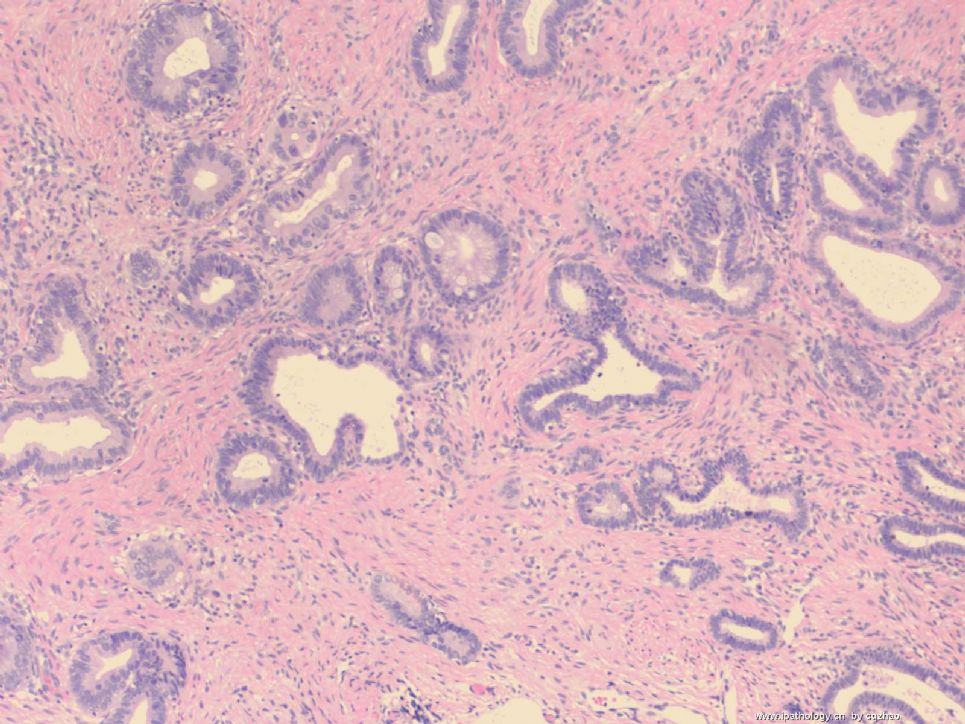
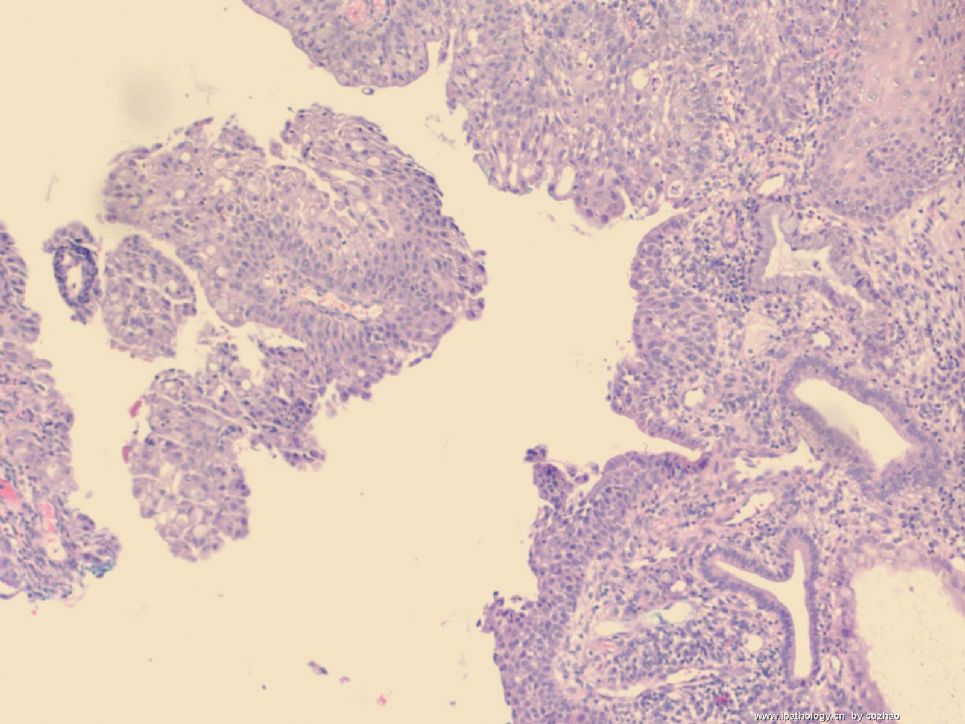
From your questions I can know you all are very thoughtul pathologists. Adenosquamous carcinomas are not uncommon in gynecologic pathology. They account for 5-25% of all cervical ca. They are defined as tumors that contain an admixture of malignant glandular and squamous epithelial components. No creteria mentioned the component should account for ?% of the total tumor volume, like ovarian bordline tumors. 只要两种癌组织都有就可以报. Squamous metaplasia can be present in the cervical endometrioid carcinoma, the same as in endometrial endometrioid ca. For my case most component is adenocarcinoma, endocervical type, and 20% is squamous cell ca. In the last histology photo 2-3 maligant glands are in the right side and most other epithelial components are maligant low grade squamous carcinoma. In the upper right focal bengin squamous metaplasia may be present. Wish you will agree with my interpretaion. I will not change my diagnosis even if you do not agree (Joking). I have to review books to anwer your important and sharp questions.
WHO classification:
A. Adenocarcinoma
1.Mucinous ca
encervical type: most common
Intestinal type
Signet ring cell type
Minimal deviation type
Villoglandular type
2. Endometrioid ca
3. Clear cell ca
4. Serous ca
5. Mesonephric
B. Other epithelial tumor
adenosquamous ca
adnoid cystic ca
adenoid basal ca
neuroendocrine tumor
undifferentiated ca
-
lfl001200546 离线

- 帖子:2808
- 粉蓝豆:40
- 经验:2808
- 注册时间:2007-02-14
- 加关注 | 发消息
-
本帖最后由 于 2008-10-13 12:46:00 编辑
Very glad to see the interpretaion of above three pathologists. Also notice that few people gave interpretation here. In fact Pap test is the most difficult area in all cytologic areas. AGC is the No 1 difficult of all Pap abnormalities.
These 3 clusters of cells are the only ones with some abnormality. The first impression is that the flat sheets of cells show increased N/C ratio, round nuclei, a little overlapping. The cytologic features are not very bad. You may consider reactive endocervical cells. Patient did not have any history. Looking carefully you will find the cells are too crowed, called hyperchromatic crowed group (HCG). Dx of atypical glandular cells, endocervical, is very good call.
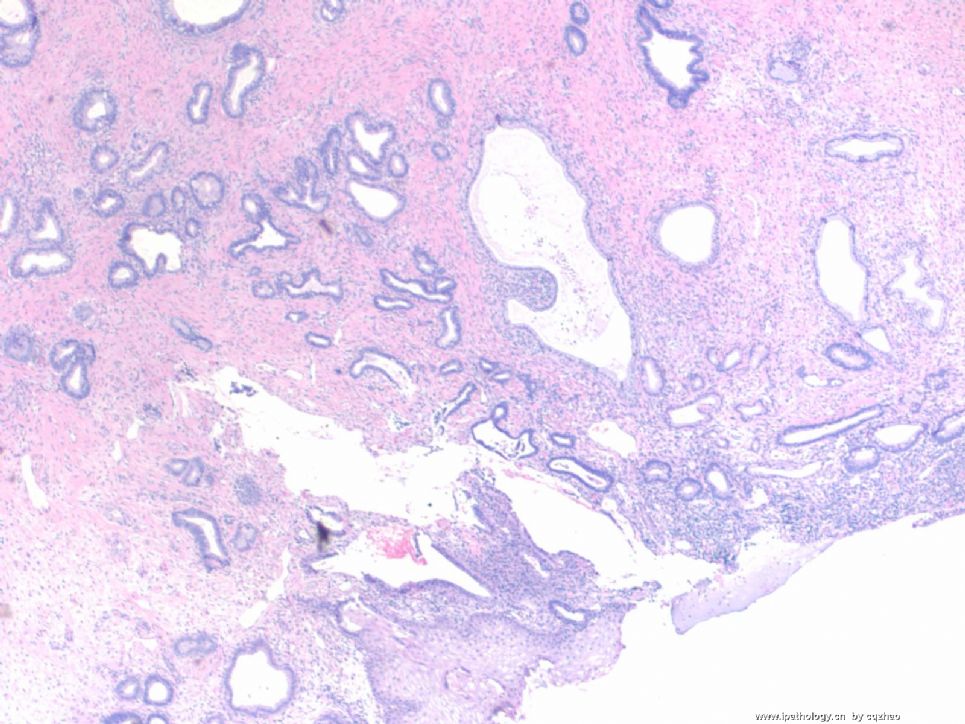
This pt had bx and hysterectomy. See few photos below. Women had invasive adenocarcinoma with some areas of adenosquamous carcinoma. Pay attention to the cytology of the tumor in histology slides. The nucler grade is low.
abin译:
非常高兴看到以上三位病理医生的判读。事实上宫颈细胞学是所有细胞学领域中最困难的领域。而AGC则是宫颈异常细胞学中第一难点。
仅有这三簇细胞显示某种程序的异常。第一印象是平铺的细胞显示核/浆比增高,核圆,有些重迭。细胞学特征并不非常恶。你可能考虑反应性宫颈管细胞。患者也没有什么特殊病史。然而仔细看,你会发现细胞太拥挤,称为深染拥挤的细胞团(hyperchromatic crowed group,HCG)。诊断不典型腺细胞,宫颈管型,是很合适的。
这位患者后来经过了活检并切除了子宫。见以下图片,患者有浸润性腺癌伴部分区域腺鳞癌。注意组织学切片上的肿瘤细胞学特点。核级别低。
- History and Current Situation in the
US - SAD Truth
Last week I had a talk about AGC. I like to share some main points about AGC with friends here.
In the 1950s: SCC account for 95% of cervical Ca.
Currently: Incidence of cervical Ca declined markedly, but rate of ADC increased.
Proportion SCC:ADC: SCC 70-75%, ADC up to 20-30% (double)
Increase of ADC mainly in young women
The incidence rate of cervical ADC never reduced
Pap test has never been proven effective in preventing cervical ADC
3. TBS 2001 Atypical Glandular Cells
• AGC
• -Endocervical cells
• -Endometrial cells
• -NOS
• AGC, favor neoplastic
• -Endocervical
• -NOS
• Endocervical AIS
• Adenocarcinoma
4. AGC Prevalence
• Kim TJ et al. Gynecol Oncol 1999;73:292
• 0.07% (
• Geier CS et al. Am J Obstet Gynecol 2001;184:64
• 5.96% (
5. AGC Prevalence
Summarized 24 studies
2,389,206 Pap
AGC 6829
AGC rate 0.29%
Schnatz PF et al. Obstet Gynecol 2006;107:701
6. AGC Prevalence
• Bethesda 2001
• Conventional Pap
– 184 Labs 0.45%
• LBP (LBP-T+S)
– 180 Labs 0.37%
– Davey DD et al: Arch Pathol Lab Med 2004;128:1224
7. AGC Prevalence-my hospital (largest study)
June 2005-August 2007 (27 months)
247,131 Pap
AGC 1021
0.41%
8. AGC Follow-up TBS2001
• Benign (>60%)
• -Polyps, endocervical, endometrial
• -Tubal metaplasia
• -Microglandular hyperplasia
• -Endometritis
• -S/P cone bx
•
• Significant lesions up to 38%
• CIN 2/3, CIN 1
• AIS
• Adenocarcinoma
9. AGC Follow-up (U of
• 82 AGC Pap tests (0.15%) (CP, LBC?)
• -38% significant pathology
– 21% pre-invasive disease (CIN2+ 11%, AIS 8.5%, EH)
– 17% invasive adenocarcinoma (ec-ca 6%, em-ca 11%)
DeSimone, CP et al. Obstet Gynecol 2006;107:1285-91
10. 460 AGC Cases with Preneoplastic or Neoplastic Lesions in Tissue Biopsies (
CIN2+ 6%
AIS+ 4%
Complex atypical hyperplasia+ 12%
Ovarian ca 1%
Total 23%
Zhao et al. Acta Cytol. 2008 (will be published soon)
11. Histologic Follow-up Study of 662 AGC (TP). My study in current hospital.
• Squamous lesions (CIN1+) 23%
• ---CIN2+ 42 (6%)
• Glandular lesions (AIS+) 3%
• Endometrial Lesion 8%
• ---EM-CA 34 (5%)
• Total 33%
• Significant 17%
• PPV for cervical glandular lesion 3%
12. Histopathologic Follow-up of 317 Patients with AEC, AGC-NOS (
• Endometrial Lesions 3.8%
• CIN1 5.0%
• CIN2+ 7.3%
• AIS+ 6.6%
• Benign 77.3%
• PPV for cervical glandular lesion 6.6%
• Chen L & Yang B. Cancer Cytopath 2008;114:236
13 HPV Positive Rate in AGC (the largest two studies)
• MWH: 75/309 24%
My study. 2008 USCAP meeting abstract. I am working on the manuscript
•
Chen L. & Yang B. Cancer Cytopathol 2008;114:236
14. Histologic Follow-up of 317 Patients with AEC, AGC-NOS (
|
|
HPV+ (n=64) |
HPV- (n=253) |
|
Benign |
16% |
93% |
|
EMH+ |
0 |
5% |
|
CIN1 |
22% |
0.8% |
|
CIN2 |
34% |
0.4% |
|
AIS+ |
28% |
1.2% |
15. HPV testing to Detect Clinically Significant Lesion (my study)
|
|
HPV+ (n=75) |
HPV- (n=234) |
|
CIN 2+ |
17% |
0.4% |
|
AIS+ |
17% |
0.4% |
|
EMH+ |
0 |
6% |
16. Reproducibility-Interlaboratories, Interobservers
• There was no consensus for both the origin of the cells and the diagnosis, poor agreement
• Kappa-type statistical analysis:
• Kappa value:<0.4 poor, 0.4-0.7 good, >0.7 excellent
17. Reproducibility-interlaboratories, interobservers
|
Authors |
Attendant |
Kappa value |
|
Confortini1 ( |
167 labs |
0.21 |
|
Simsir2 (2 universities) |
6 observers |
0.002 (CP) |
|
Lee3 |
5 experts |
<0.3 in C+LBC |
|
Raab4 |
4 experts |
0.16-0.27 |
• 1. Cytopath 2006;17:353
• 2. Cancer 2003;99:323
• 3. Am J Clin Pathol 2002;117:96
• 4. Am J Clin Pathol 1998;110:653
18. Facts: AGC
• 0.2-0.5% of Pap results
• High incidence of underlying neoplasia (>CIN II, AIS, Cancer)
• Common error: following with Paps, missing invasive cancer
• Neither HPV testing nor repeat pap is sensitive enough to be used alone as triage
• Poor agreement
• Poor PPV for glandular lesions
• Most interesting (?) AND the most difficult of all cervical cytology
• Strongly suggested
• PPV is markedly increased compared with Pap only
• NPV is very high
19. When in Doubt
• Carefully check clinical data
– recent pregnancy?
– patient wears IUD?
– recent Bx/LEEP?
– Hx of GYN, radiation, chemo
• Second opinion, even though agreement is very poor
20. Balance: Overcall vs Undercall
• Misinterpretation is potential delay in patient tx & increased risk for development of invasive ADC
• May lead to over-diagnosis of AGC-over treatment
• Fine balance to maintain sensitivity and specificity;
pressure to NOT undercall OR overcall
Thank for reading the long mail,
cqz
•











