





| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- 免疫组化鉴别乳腺导管浸润癌和小叶癌
-
shanghainese 离线

- 帖子:1136
- 粉蓝豆:25
- 经验:1155
- 注册时间:2006-09-26
- 加关注 | 发消息
-
Histology of some ductal carcinomas mimics lobular carcinomas, and this is observed at both in situ and invasive cases. The most useful marker to differentiate ductal from lobular differentiation remains E=Cadherin. Very rare cases of lobular carcinoma (in situ and invasive) will express strong E-Cadherin on immunohistochemistry. As for 34betaE12, it is not as consistent as some have claimed. In other words, some ductal carcinomas have strong expression of this marker just like lobular carcinomas do. My experience with beta-catenin is limited.

聞道有先後,術業有專攻
-
wangzhen_01 离线
- 帖子:197
- 粉蓝豆:3
- 经验:197
- 注册时间:2006-10-04
- 加关注 | 发消息
-
本帖最后由 于 2007-04-29 12:03:00 编辑
马老师发言翻译:
一些导管癌的组织学与小叶癌很相似,这在一些原位导管癌和侵袭性导管癌病例中都可以观察到。E-Cadherin是一个鉴别导管癌向小叶分化的有用的标志。免疫组织化学检测E-Cadherin 蛋白,小叶癌(原位的或者侵袭性的)呈强阳性的很少。至于34betaE12,它并不像某些人说的那样一致,有些导管癌中34betaE12呈现和小叶癌中一致的强表达。而beta-catenin,我还没有什么经验。
- 吾表兄,年四十余。始从文,连考三年而不中。遂习武,练武场上发一矢,中鼓吏,逐之出。改学医,自撰一良方,服之,卒。
-
wangzhen_01 离线
- 帖子:197
- 粉蓝豆:3
- 经验:197
- 注册时间:2006-10-04
- 加关注 | 发消息
-
wangzhen_01 离线
- 帖子:197
- 粉蓝豆:3
- 经验:197
- 注册时间:2006-10-04
- 加关注 | 发消息
-
本帖最后由 于 2007-05-31 18:55:00 编辑
感谢yang老师提供信息,感谢wangzhen_01查阅原文。
Lobular Versus Ductal Breast Neoplasms
The Diagnostic Utility of P120 Catenin
Abstract: The distinction between lobular and ductal lesions of the breast is important in several circumstances.Diagnostic reproducibility of lobular versus ductal lesions, based on histology alone, is less than optimal. The
proper distinction between atypical lobular hyperplasia, lobular carcinoma in situ and low-grade ductal carcinoma
in situ is critical for patient management. Patients who have a core biopsy of invasive lobular carcinoma often
have preoperative magnetic resonance imaging to prepare the surgeon for proper margin attainment. E-cadherin, a
negative membrane marker for lobular neoplasia, is useful in the distinction of lobular versus ductal neoplasia,
but as a negative marker, can be difficult to interpret in particularly challenging cases. In this study, we
surveyed primary and metastatic ductal lesions (62) and lobular lesions (64) of the breast to determine if P120
catenin is useful in the diagnostic distinction between lobular and ductal neoplasia. Primary breast ductal and
lobular preneoplastic and neoplastic lesions were immunostained with E-cadherin and P120ctn and independently
classified as ductal or lobular lesions. In addition, a wide array of carcinomas of different types were surveyed
with P120ctn in tissue microarrays to ascertain whether the cytoplasmic P120ctn immunostaining pattern observed in
lobular neoplasia was unique. Accurate categorization of ductal versus lobular neoplasia in the breast with
P120ctn immunostaining was effective in all cases. Separation of low-grade ductal carcinoma in situ from lobular
neoplasia was efficient. Diagnostically, P120ctn was particularly useful in identifying early lesions of lobular
neoplasia. Of the other tumors that may morphologically mimic lobular carcinoma, only the diffusely infiltrating
variants of rectal and gastric carcinomas showed diffuse cytoplasmic P120ctn immunostaining. Caution should be
exercised when examining tumors in metastatic sites with P120ctn, with the incorporation of an appropriate panel
of immunostains.
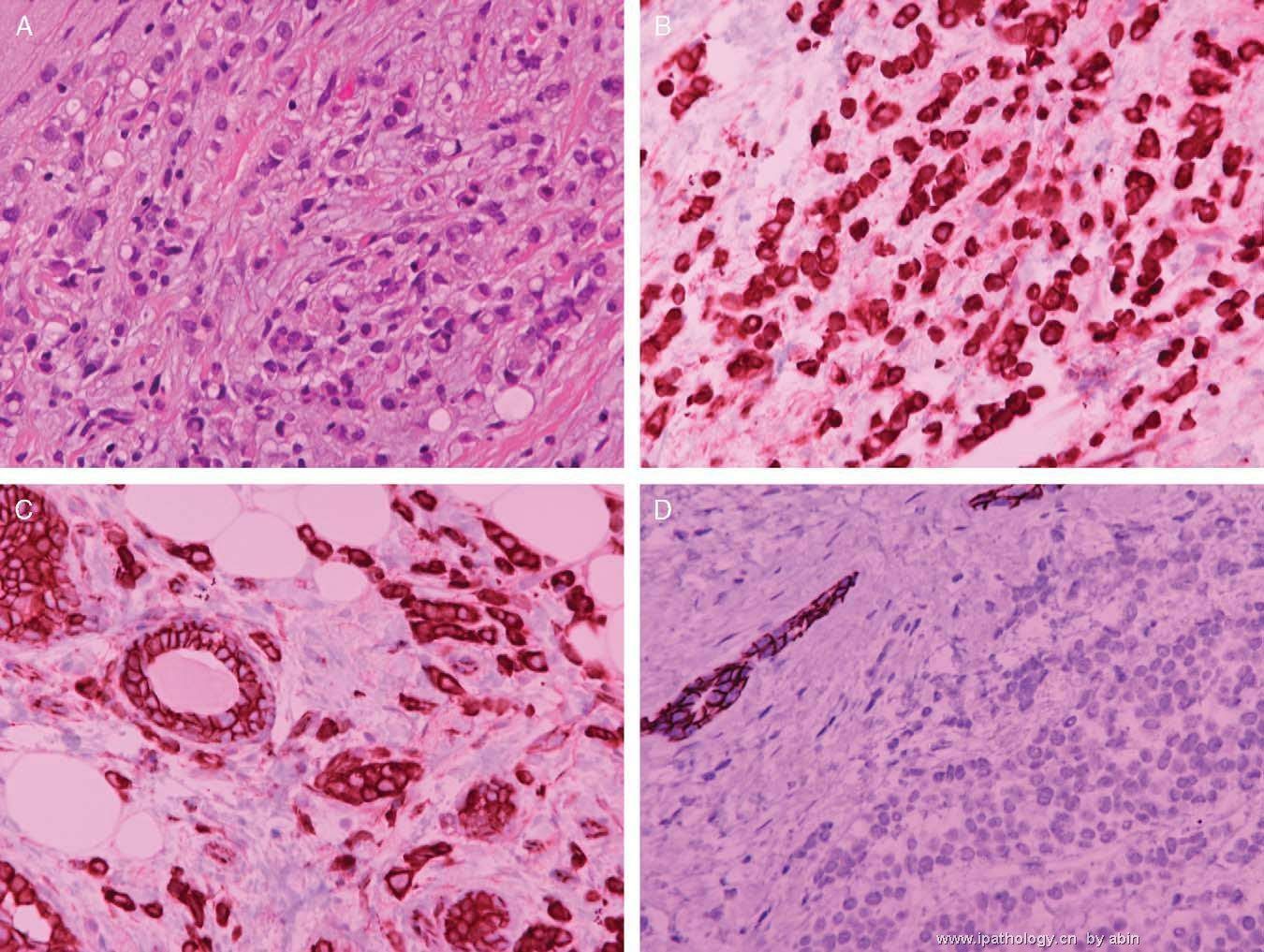
FIGURE 1. Lobular versus ductal neoplasia.
A, Invasive lobular carcinoma, hematoxylin/eosin.
B, P120ctn: invasive lobular carcinoma with diffuse cytoplasmic stain.
C, Comparison of membranous P120ctn staining in normal duct to the cytoplasmiconly staining of lobular carcinoma.
D, Negative E-cadherin of the same case in (C), membranous pattern in normal duct.
A, Invasive lobular carcinoma, hematoxylin/eosin.
B, P120ctn: invasive lobular carcinoma with diffuse cytoplasmic stain.
C, Comparison of membranous P120ctn staining in normal duct to the cytoplasmiconly staining of lobular carcinoma.
D, Negative E-cadherin of the same case in (C), membranous pattern in normal duct.
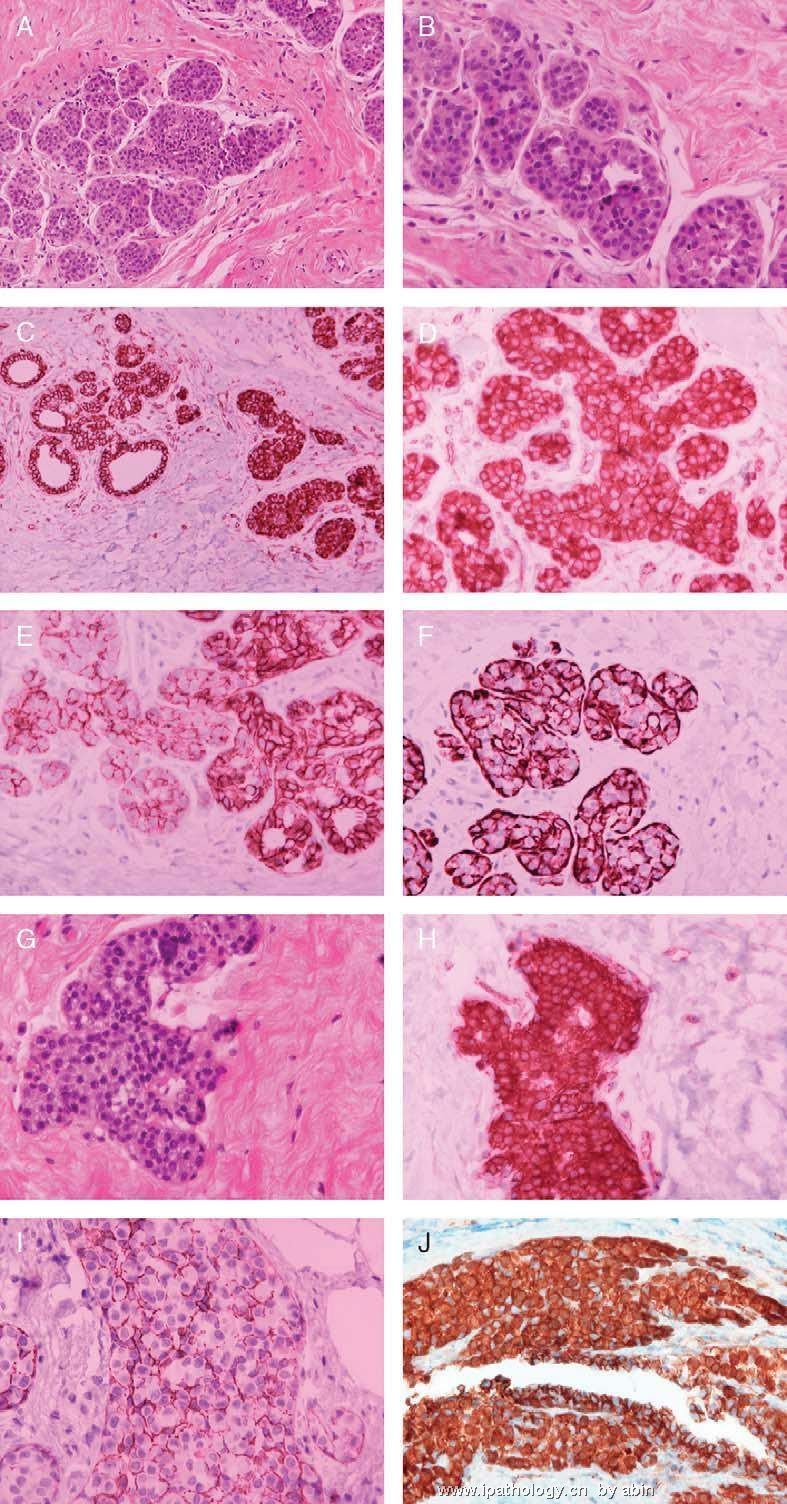
FIGURE 2. A to J, P120 ctn in challenging diagnostic cases:
A and B, duct epithelial hyperplasia or emerging lobular neoplasia (ALH)?
C, P120ctn shows intense cytoplasmic immunostaining of ALH cells appearing in the lobule; compare with the left side
of the photograph where P120ctn shows membranous immunostaining of the terminal lobule cells.
D, Higher magnification of lobular neoplasia (ALH) in 2C.
E, E-cadherin result of this same case is less conspicuous, but shows lack of membrane immunostaining of ALH cells.
Myoepithelial cells are stained with E-cadherin.
F, Shows immunostaining of myoepithelial cells with smooth muscle myosin heavy chain in the section
adjacent to (E).
G, Low-grade ductal neoplasia, or lobular neoplasia with microcalcification?
H, P120ctn confirms lobular neoplasia with characteristic intense, diffuse cytoplasmic immunostaining.
I, This area of LCIS lacks E-cadherin stain but shows myoepithelial cell staining, which some may find confusing.
J, Same area as (H) which intensely displays P120ctn characteristic for LCIS.
A and B, duct epithelial hyperplasia or emerging lobular neoplasia (ALH)?
C, P120ctn shows intense cytoplasmic immunostaining of ALH cells appearing in the lobule; compare with the left side
of the photograph where P120ctn shows membranous immunostaining of the terminal lobule cells.
D, Higher magnification of lobular neoplasia (ALH) in 2C.
E, E-cadherin result of this same case is less conspicuous, but shows lack of membrane immunostaining of ALH cells.
Myoepithelial cells are stained with E-cadherin.
F, Shows immunostaining of myoepithelial cells with smooth muscle myosin heavy chain in the section
adjacent to (E).
G, Low-grade ductal neoplasia, or lobular neoplasia with microcalcification?
H, P120ctn confirms lobular neoplasia with characteristic intense, diffuse cytoplasmic immunostaining.
I, This area of LCIS lacks E-cadherin stain but shows myoepithelial cell staining, which some may find confusing.
J, Same area as (H) which intensely displays P120ctn characteristic for LCIS.
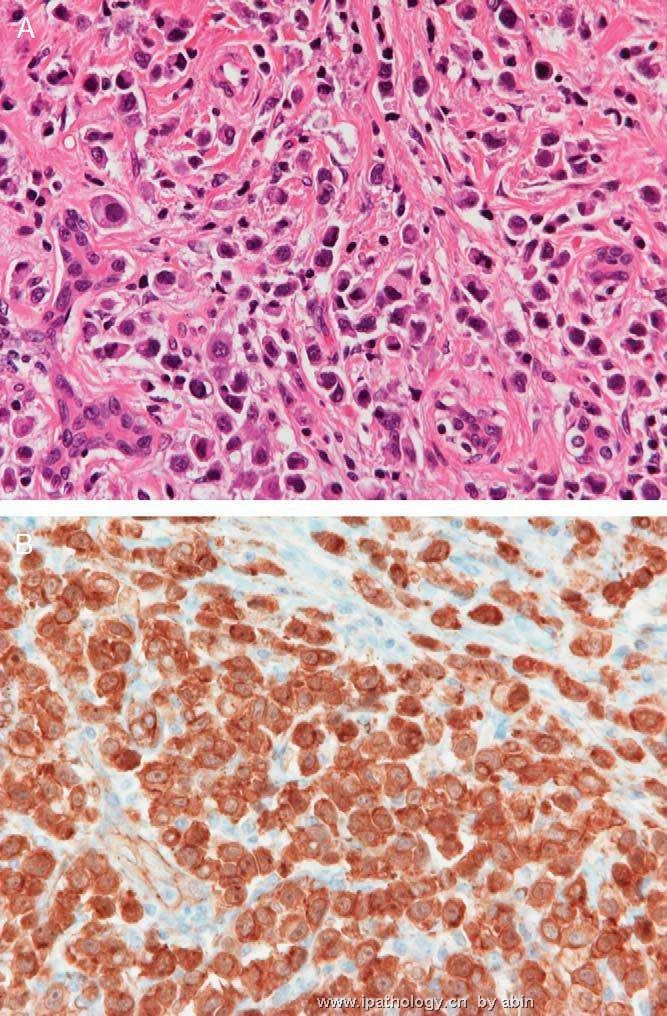
FIGURE 3. A, Pleomorphic variant of lobular carcinoma, hematoxylin/eosin.
B, Diffuse cytoplasmic pattern for P120ctn.
B, Diffuse cytoplasmic pattern for P120ctn.
华夏病理/粉蓝医疗
为基层医院病理科提供全面解决方案,
努力让人人享有便捷准确可靠的病理诊断服务。
-
本帖最后由 于 2008-04-20 23:06:00 编辑
本网站有关小叶癌的帖子:
http://www.ipathology.org.cn/forum/forum_display.asp?keyno=2029
http://www.ipathology.org.cn/forum/forum_display.asp?keyno=7516
http://www.ipathology.org.cn/forum/forum_display.asp?keyno=29908
http://www.ipathology.org.cn/forum/forum_display.asp?keyno=62115
华夏病理/粉蓝医疗
为基层医院病理科提供全面解决方案,
努力让人人享有便捷准确可靠的病理诊断服务。
-
hongpinguo 离线

- 帖子:92
- 粉蓝豆:142
- 经验:109
- 注册时间:2009-01-16
- 加关注 | 发消息











