


























| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- 急会诊!请教是什么病原体?
-
Though suspicious, I am not sure there is a pathogenic micro-organism in the macrophages. Was acid-fast stain done? What is 六氨银染色? Is it the same as Grocott methenamine-silver stain for fungus? If no fresh tissue was sent for culture, they should consider getting another fresh specimen for culture.

聞道有先後,術業有專攻
-
lfl001200546 离线

- 帖子:2808
- 粉蓝豆:40
- 经验:2808
- 注册时间:2007-02-14
- 加关注 | 发消息
| 以下是引用mjma在2008-3-15 23:12:00的发言: Though suspicious, I am not sure there is a pathogenic micro-organism in the macrophages. Was acid-fast stain done? What is 六氨银染色? Is it the same as Grocott methenamine-silver stain for fungus? If no fresh tissue was sent for culture, they should consider getting another fresh specimen for culture.
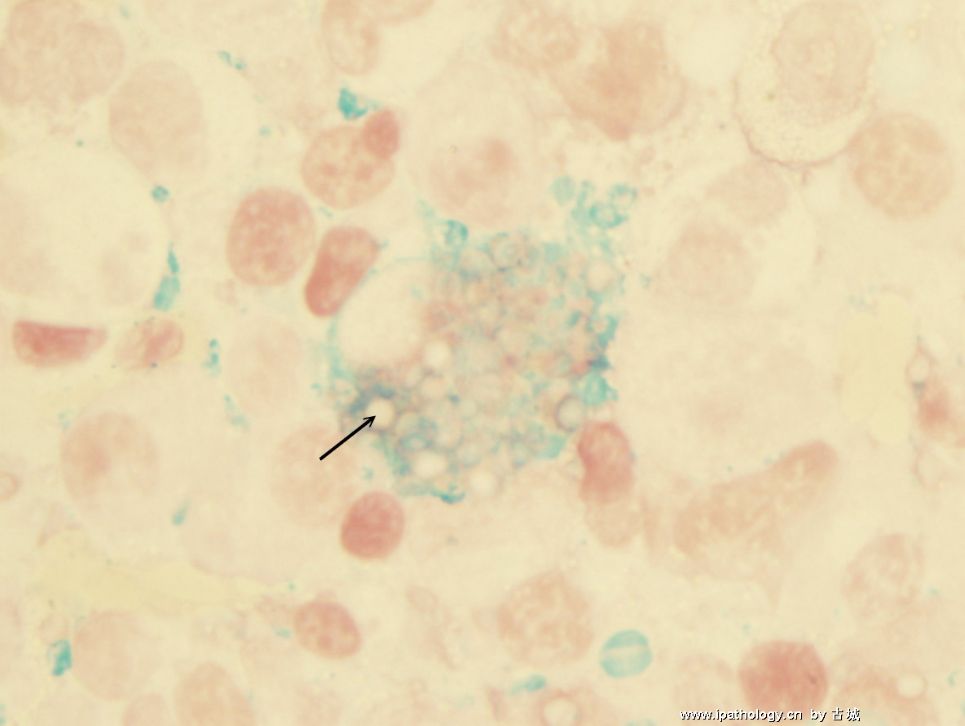
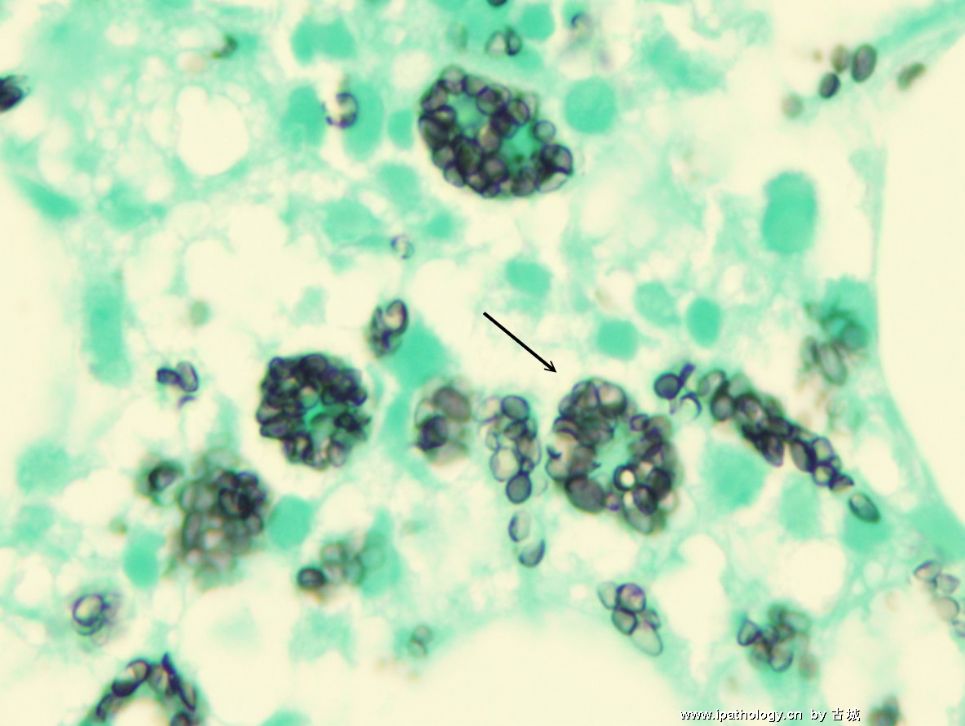
我们常规用PAS和六氨银染色显示真菌。 组织学不像结核,所以没有做抗酸染色。 |
Kitty, This is a challenge case since no culture will confirm our guesses here. I am not an expert in infectioous diseases. I just provide my thinking process of this case.
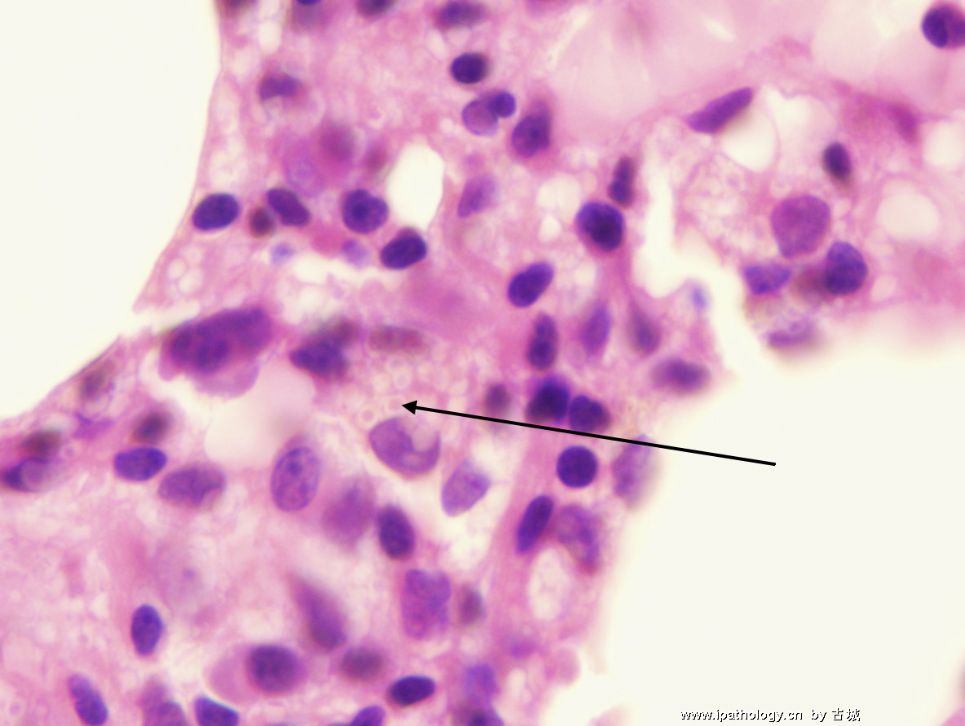
Based on PAS and Silver stains you provided, these are organisms, most likely fungi, resides mainly intracellularly in histiocytes and macrophages. There are several fungi which are facultative intracellular, including but not limited to histoplasma capsulatum, coccidioides immitis and leishmaniasis. Among them, I highly suspicious this is a dissemintaed histioplasmosis. In chronic histioplasmosis, granulomatous inflammation is often prominent. In this case, both clinical systemic presentation and lack of granuloma formation pathologically points to a fulminant dissemintated histoplamosis. I guess you can toss amebiasis in the differential, however, with clinical involvement of lung and pleural, but lack of intestinal symptoms, histoplasmosis rather than amebiasis should be favored. As cell-mediated immunity and T-cells are the main force to fight against histoplasmosis, I bet this patient is immunocompromised. As most organisms are intracellular, it will be very challenge clinically to eradicate these organisms just using antibiotics. This patient needs to have culture of tissue to confirm the diagnosis from pathologic point of view, but not much help in terms of clinical treatment.
- 不坠青云之志,长怀赤子之心
| 以下是引用杨斌在2008-3-18 1:14:00的发言:
Kitty, This is a challenge case since no culture will confirm our guesses here. I am not an expert in infectioous diseases. I just provide my thinking process of this case. Based on PAS and Silver stains you provided, these are organisms, most likely fungi, resides mainly intracellularly in histiocytes and macrophages. There are several fungi which are facultative intracellular, including but not limited to histoplasma capsulatum, coccidioides immitis and leishmaniasis. Among them, I highly suspicious this is a dissemintaed histioplasmosis. In chronic histioplasmosis, granulomatous inflammation is often prominent. In this case, both clinical systemic presentation and lack of granuloma formation pathologically points to a fulminant dissemintated histoplamosis. I guess you can toss amebiasis in the differential, however, with clinical involvement of lung and pleural, but lack of intestinal symptoms, histoplasmosis rather than amebiasis should be favored. As cell-mediated immunity and T-cells are the main force to fight against histoplasmosis, I bet this patient is immunocompromised. As most organisms are intracellular, it will be very challenge clinically to eradicate these organisms just using antibiotics. This patient needs to have culture of tissue to confirm the diagnosis from pathologic point of view, but not much help in terms of clinical treatment.
非常感谢您对本例提供的诊断思路! 正如您所猜测,病人一年前有过短期的服用激素的病史,可能导致免疫功能低下而诱发感染。 从临床来说,目前病人一般状况明显好转,体温正常,复查血象正常,穿刺物培养结果为阴性。已经出院,继续抗感染治疗,外科医生建议一个月后复查MRI,如果炎症范围局限可以考虑手术切除。 从病理来说,我们又做了组织细胞的免疫组化标记,排除了阿米巴。另外,请了有经验的检验学教授会诊,很明确否定了真菌感染。经专家指点,在100倍油镜下观察,组织细胞胞浆中的吞噬物跟组织胞浆菌的确比较容易鉴别。 |











