



















| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- 鞍区肿瘤
-
zhongshihua 离线

- 帖子:1608
- 粉蓝豆:0
- 经验:1651
- 注册时间:2006-09-11
- 加关注 | 发消息
-
zhongshihua 离线
- 帖子:1608
- 粉蓝豆:0
- 经验:1651
- 注册时间:2006-09-11
- 加关注 | 发消息
-
本帖最后由 于 2006-11-23 10:18:00 编辑
| 以下是引用zhongshihua 在2006-11-22 20:08:00的发言: 这例可否诊断为“鞍区黄色肉芽肿”。 |
Your photos clearly show keratinizing squamous epithelia and formation of "wet" keratin that are diagnostic of craniopharyngioma (adamantinomatous type) in the sellar region. Sometimes there are numerous Rosenthal fibers in the surrounding gliotic parenchyma. Certainly there are prominent associated xanthogranulomatous inflammation and calcification, but these are probably the result of repeated hemorrhage in the past (hence the deposition of numerous cholesterol crystals) and resultant tissue reaction to the "wet" keratin formed. Pure xanthagranulomas (like that seen in the choroid plexus) are not neoplasms and should not have destructive growth or high risk for local recurrence. Craniopharyngiomas, on the other hand, are truly neoplastic - they grow and destroy local parenchyma, and have the tendency to recur locally even after apparent complete surgical resection. In fact, this is a recurrent case. Sometimes, inflammation around a craniopharyngioma is so severe and prominent that one may miss the diagnostic keratininizing stratified squamous epithelia, stellate reticulum, or "wet" keratin. Because they behave in entirely different fashions, it is essential not to misdiagnose a craniopharyngioma as a xanthogranuloma.
Another important diagnostic consideration is to rule out Rathke cleft cyst in the sellar region. Craniopharyngiomas are often cystic. Rathke cleft cysts are derived from the pituitary gland, and are lined by metaplastic stratified squamous epithelia (without formation of "wet" keratin). Rathke cleft cysts can be large from repeated old hemorrhage into the cystic cavity and be associated with resultant cholesterol crystals, Rosenthal fibers and xanthogranulomatous inflammation. In other words, the two look very much alike. The only morphologic difference is the amount and characteristics of the stratified squamous epithelia present.

聞道有先後,術業有專攻
-
Allow me to share a few more comments on craniopharyngioma.
 图1
图1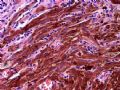 图2
图2
Pathologic subtypes and their clinical significance - Traditionally, craniopharyngiomas are divided into two histopathologic types - adamantinomatous type (mainly in children and young adults) and papillary type (mainly in adults). In addition to peripheral palisades and cystic change, the stratified squamous epithelia in an adamantinomatous craniopharyngioma form nodules of "wet" keratin (see Figures 2 and 11 of this case). "Wet" keratin, under the microscope, appears as cohesive eosinophilic squames arranged in pavement-like sheets. They are often without nuclei, but a central pale nuclear zone is seen in each squame and the cells surrounding "wet" keratin may retain their nuclei. The same kind of "wet" keratin is seen in pilar (trichilemmal) cysts and pilomatrixomas (http://www.dermatlas.com/derm/IndexDisplay.cfm?ImageID=-1267597359) on scalp. "Wet" keratin is different from the mature (orthokeratotic) keratinous squames seen in epidermoid or dermoid cysts. The non-keratinized squamous epithelia in adamantinomatous craniopharyngiomas often show classic stellate reticulum. Papillary craniopharyngiomas, on the other hand, almost never show epithelial keratinization or calcification. They may be cystic, form papillae, and display stellate reticulum, but the cells are actually more like transitional epithelia (small oval nuclei with nuclear grooves) than squamous epithelia. Some earlier reports claimed that the papillary type is less aggressive (regarding risk for recurrence) than the adamantinomatous type, but this has not been shown by later studies. Perhaps a more important determinant of risk for recurrence is the extent of surgical excision. Recently, mutational analysis of beta-catenin gene suggested that adamantinomatous and papillary craniopharyngiomas are indeed different (http://ajp.amjpathol.org/cgi/reprint/161/6/1997.pdf).
Bone invasion versus metaplastic ossification - Potentially any craniopharyngioma at the sellar region may invade into and destroy the underlying sella turcica and clivus (above sphenoid sinus). It is common to have calcification and metaplastic ossification in a given adamantinomatous craniopharyngioma. Therefore, finding trabecular bone in the center of an adamantinomatous craniopharyngioma doesn't mean there has been bone invasion.
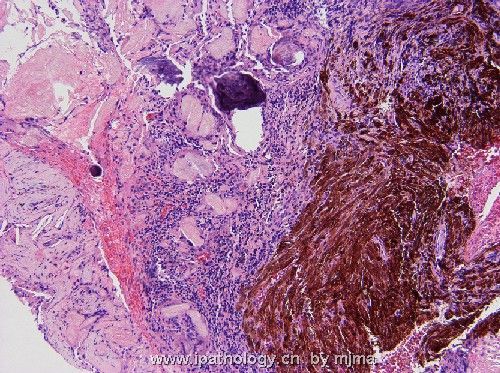
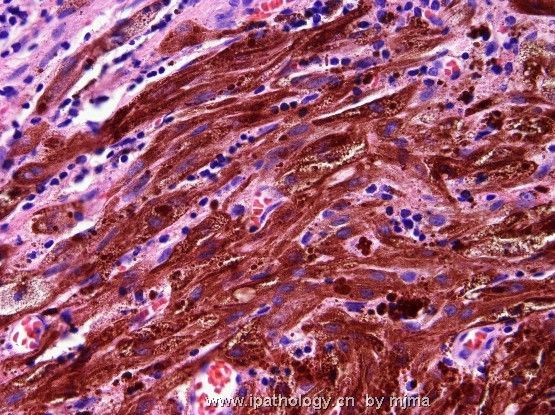
Melanin pigment - Rare craniopharyngiomas may for bone fide melanin pigment in some neoplastic cells. The pigments are very fine and granular, rather than clumped in varying sizes as hemosiderin in siderophages that also exist in many craniopharyngiomas. This fact has been reported (http://www.springerlink.com/content/bv84w0l49y60c76d/) and I have observed it once (see photos below). It doesn't impart a different prognosis. This has been used to imply pharyngeal pouch as the common histologic origin of both craniopharyngiomas and Rathke cleft cysts.
Malignant change - The squamous epithelia in craniopharyngiomas may rarely undergo malignant transformation into squamous cell carcinoma, usually as recurrence.
聞道有先後,術業有專攻
-
zhongshihua 离线
- 帖子:1608
- 粉蓝豆:0
- 经验:1651
- 注册时间:2006-09-11
- 加关注 | 发消息
-
本帖最后由 于 2006-11-24 12:28:00 编辑
我请
Allow me to share a few more comments on craniopharyngioma. 二次评论如下:Pathologic subtypes and their clinical significance – 颅咽管瘤病理和临床特点如下:Traditionally, craniopharyngiomas are divided into two histopathologic types - adamantinomatous type (mainly in children and young adults) and papillary type (mainly in adults).传统组织学分类将其分为两型,造釉细胞型颅咽管瘤(见于儿童和青年)和乳头型颅咽管瘤(见于成人)。 In addition to peripheral palisades and cystic change, the stratified squamous epithelia in an adamantinomatous craniopharyngioma form nodules of "wet" keratin (see Figures 2 and 11 of this case). 造釉细胞型颅咽管瘤镜下可见鳞状上皮细胞团外围呈栅栏状排列,囊性变,并有湿角化蛋白结节形成(图2图11)。"Wet" keratin, under the microscope, appears as cohesive eosinophilic squames arranged in pavement-like sheets. 湿角蛋白镜下是鳞状细胞排列呈致密的嗜酸性团块。They are often without nuclei, but a central pale nuclear zone is seen in each squame and the cells surrounding "wet" keratin may retain their nuclei. 湿角蛋白的鳞状细胞常常没有细胞核,中心区可以看到单个鳞状细胞的浅色之细胞核,湿角化蛋白周围的鳞状细胞都有细胞核。The same kind of "wet" keratin is seen in pilar (trichilemmal) cysts and pilomatrixomas (http://www.dermatlas.com/derm/IndexDisplay.cfm?ImageID=-1267597359) on scalp.这种湿角蛋白也见于毛囊囊肿和钙化上皮瘤。 "Wet" keratin is different from the mature (orthokeratotic) keratinous squames seen in epidermoid or dermoid cysts.湿角化蛋白不同于表皮囊肿和皮样囊肿的成熟角化鳞状上皮。 The non-keratinized squamous epithelia in adamantinomatous craniopharyngiomas often show classic stellate reticulum. 造釉细胞瘤型颅咽管瘤其非角化鳞状上皮常呈典型之星网状结构。Papillary craniopharyngiomas, on the other hand, almost never show epithelial keratinization or calcification. 乳状型颅咽管瘤没有上皮角化或钙化。They may be cystic, form papillae, and display stellate reticulum, but the cells are actually more like transitional epithelia (small oval nuclei with nuclear grooves) than squamous epithelia. 乳头型颅咽管瘤呈囊性,形成乳头,有星网状结构,但是其细胞的确像移行上皮(比鳞状上皮小,核卵圆形,有核沟)。Some earlier reports claimed that the papillary type is less aggressive (regarding risk for recurrence) than the adamantinomatous type, but this has not been shown by later studies. 有些早期报告乳头型颅咽管瘤复发少,侵袭性弱,但是未被以后的研究所证实。Perhaps a more important determinant of risk for recurrence is the extent of surgical excision.更重要的是手术需要做彻底,避免复发。 Recently, mutational analysis of beta-catenin gene suggested that adamantinomatous and papillary craniopharyngiomas are indeed different (http://ajp.amjpathol.org/cgi/reprint/161/6/1997.pdf).最近研究显示两型颅咽管瘤的基因的确是不同。
Bone invasion versus metaplastic ossification 骨浸润与化生性骨化:- Potentially any craniopharyngioma at the sellar region may invade into and destroy the underlying sella turcica and clivus (above sphenoid sinus).任何蝶鞍部的颅咽管瘤都有潜在性的侵袭破坏蝶鞍和筛窦。 It is common to have calcification and metaplastic ossification in a given adamantinomatous craniopharyngioma.但是在造釉细胞型的颅咽管瘤常发生钙化和化生性骨化。 Therefore, finding trabecular bone in the center of an adamantinomatous craniopharyngioma doesn't mean there has been bone invasion. 因此肿瘤中心发现骨小梁并不意味着骨浸润。
Melanin pigment – 黑色素:Rare craniopharyngiomas may for bone fide melanin pigment in some neoplastic cells. 颅咽管瘤的瘤细胞有黑色素极其罕见,The pigments are very fine and granular, rather than clumped in varying sizes as hemosiderin in siderophages that also exist in many craniopharyngiomas. 这种色素颗粒很细,并非大小不等的含铁血黄素(许多颅咽管瘤有吞噬铁的巨噬细胞)This fact has been reported (http://www.springerlink.com/content/bv84w
-
zhongshihua 离线
- 帖子:1608
- 粉蓝豆:0
- 经验:1651
- 注册时间:2006-09-11
- 加关注 | 发消息
-
本帖最后由 于 2006-11-24 12:30:00 编辑
这是马老师的第一个帖子,为了方便大家学习,中英对照如下:
| Your photos clearly show keratinizing squamous epithelia and formation of "wet" keratin that are diagnostic of craniopharyngioma (adamantinomatous type) in the sellar region. 本例图片清楚地显示了角化鳞状上皮和湿角化蛋白(此为蝶鞍造釉细胞瘤型颅咽管瘤的诊断性标志)。Sometimes there are numerous Rosenthal fibers in the surrounding gliotic parenchyma. 有时可见肿瘤周围胶质增生的组织中有许多Rosenthal纤维,Certainly there are prominent associated xanthogranulomatous inflammation and calcification, but these are probably the result of repeated hemorrhage in the past (hence the deposition of numerous cholesterol crystals) and resultant tissue reaction to the "wet" keratin formed. 颅咽管瘤常常伴发明显的黄色肉芽肿性炎和钙化,可能因过去局部反复出血或大量的胆固醇沉积所致,也可能因湿角化蛋白形成刺激局部组织所致。Pure xanthagranulomas (like that seen in the choroid plexus) are not neoplasms and should not have destructive growth or high risk for local recurrence. 单纯性黄色肉芽肿(见于脉胳丛)并不是肿瘤,也不呈破坏性生长,更不会局部复发。Craniopharyngiomas, on the other hand, are truly neoplastic - they grow and destroy local parenchyma, and have the tendency to recur locally even after apparent complete surgical resection. In fact, this is a recurrent case. 换言之,颅咽管瘤是真性肿瘤,其生长并且破坏局部组织,甚至你感觉已经完整切除后,它都会局部复发。事实上,本例就是复发病例。Sometimes, inflammation around a craniopharyngioma is so severe and prominent that one may miss the diagnostic keratininizing stratified squamous epithelia, stellate reticulum, or "wet" keratin. 有时,颅咽管瘤周围的炎症病变非常明显,甚至我们根本看不到诊断性的角化复层鳞状上皮、星网状结构以及湿角化蛋白。Because they behave in entirely different fashions, it is essential not to misdiagnose a craniopharyngioma as a xanthogranuloma.但是因为颅咽管瘤和黄色肉芽肿有明显不同的生物学行为,因此不能将两者搞混。Another important diagnostic consideration is to rule out Rathke cleft cyst in the sellar region. 另一个需要鉴别的诊断是蝶鞍部的Rathke裂囊肿,Craniopharyngiomas are often cystic. 颅咽管瘤常为囊性,Rathke cleft cysts are derived from the pituitary gland, and are lined by metaplastic stratified squamous epithelia (without formation of "wet" keratin). Rathke裂囊肿起源于垂体,囊肿内衬化生性复层鳞状上皮,没有湿角蛋白形成。Rathke cleft cysts can be large from repeated old hemorrhage into the cystic cavity and be associated with resultant cholesterol crystals, Rosenthal fibers and xanthogranulomatous inflammation. Rathke裂囊肿也可有许多继发性的病理改变,如反复的陈旧性出血,囊腔形成,继发胆固醇结晶的沉积,伴发Rosenthal纤维增生,甚至也可有黄色肉芽肿形成。In other words, the two look very much alike. The only morphologic difference is the amount and characteristics of the stratified squamous epithelia present. 换句话说,两者非常相似,形态区别只有依靠综合分析和观察复层鳞状上皮的特点。 |











