
















| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- 颞顶部占位:胶质瘤?增生?
-
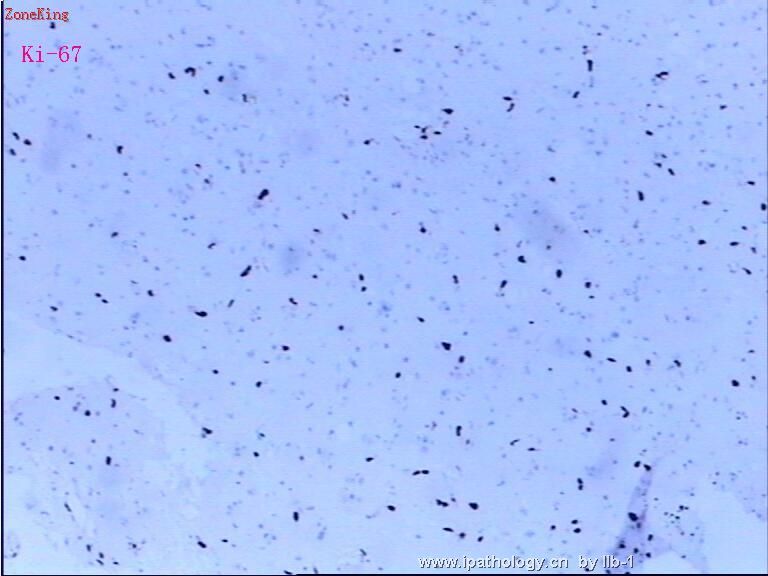
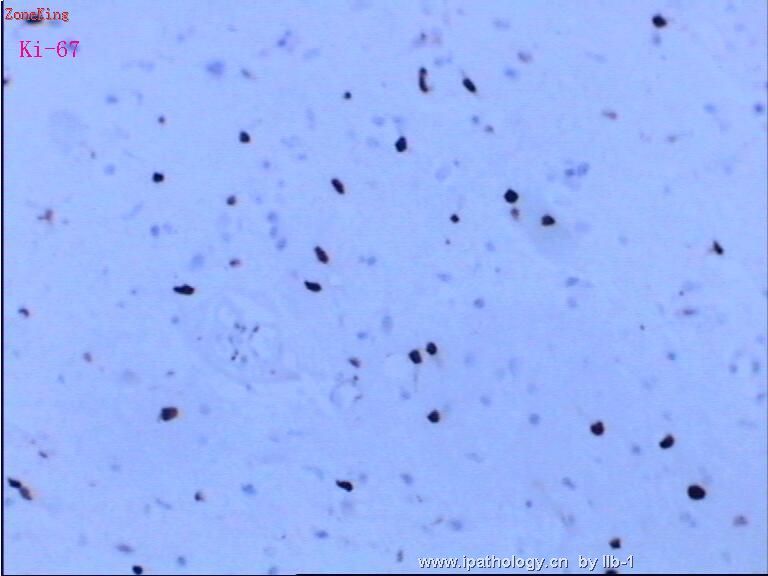
This is not an easy case to interpret. There is edema and gliosis in the brain parenchyma shown. Is the large structure in Figure 8 a large hyperchromatic nucleus? Figure 10 shows a few cells with possible cytologic atypia. Without hypercellularity, the significance of these rare atypical cells is difficult to determine. When in doubt, do immunohistochemical stains of MIB-1 (Ki67) and p53 for additional help.

聞道有先後,術業有專攻
看了马老师的这段帖子,马老师认真工作的精神正是我所缺乏的,一点点小的病变他都要花那么大的精力,我们以后的工作也需要学习马老师的这种精细作风。为此我译了这段,供大家参考:
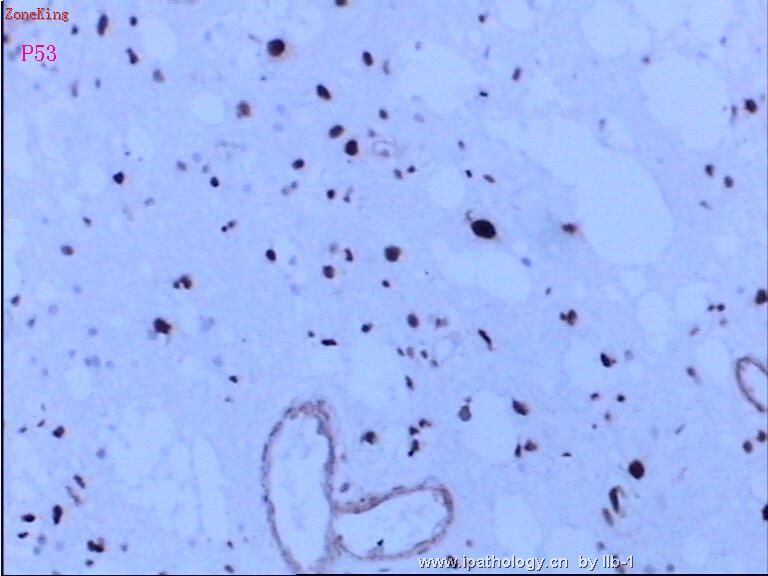
本例免疫组化非常明确地显示P53和MIB-1强阳性, 可以诊断为细胞数较少的浸润性纤维性星形细胞瘤,有了这些图片我就可以不用去数分裂相. 有点奇怪的是瘤细胞数目这么少,却有许多的阳性表达的细胞,这也提醒我是不是取材部位是高度恶性的星形细胞瘤的边缘,高度恶性星形细胞瘤的边缘可以类似WHO分类的星形细胞瘤II 级.因此,这个肿瘤的分级可能是非常复杂的,确诊取决两方面:1、你接受的病理检查组织有多少,2、术前术后的核磁共震所见。需要认真考虑避免分级过低,露掉了真正高度恶性之星形细胞瘤。
如果活检标本太少,诊断病理医师要考虑标本能否代表核磁所反映的全部病变。再看一看核磁上肿瘤大小,形状,解剖部位,是否多灶性,病变的质地,周围有无水肿,对比增强改变。这些改变放射科医生诊断了什么?如果核磁考虑是高度恶性肿瘤或胶母细胞瘤,本例表现出的类似WHO分类的星形细胞瘤II 级或弥漫浸润性的星形细胞瘤诊断可能是错的。这是因为外科医生取活检的部位是肿瘤之边缘,并非中心,也不是分级最恶性的代表区域。
如果活检标本太少,诊断病理医师要考虑标本能否代表核磁所反映的全部病变。再看一看核磁上肿瘤大小,形状,解剖部位,是否多灶性,病变的质地,周围有无水肿,对比增强改变。这些改变放射科医生诊断了什么?如果核磁考虑是高度恶性肿瘤或胶母细胞瘤,本例表现出的类似WHO分类的星形细胞瘤II 级或弥漫浸润性的星形细胞瘤诊断可能是错的。这是因为外科医生取活检的部位是肿瘤之边缘,并非中心,也不是分级最恶性的代表区域。
从该病例的大体标本的描写来看,送检标本可能是开颅活检或者是次全切除,有时我们试验室接受的标本并不是手术切除标本的全部,有些神经外科医生送给病理医生的标本只是他们大体检查后认为有代表性的部分标本,而不是标本的全部,这些送检的标本有时候经过冰冻切片确诊,有时候根本没有做冰冻诊断。他们找出认为异常的组织送检病理试验室,然后继续切除他们认为是异常的组织,常常借助于超声吸引器将病变的软组织抽吸到吸引器中,这些异常或正常组织被抽吸到吸引器中,与泡沫状的盐水和血液混合,由于这种操作,使病理医师很难接受到足够量的病理标本,有些神经外科医生根本就不送检这些吸引器里的标本,甚至直接丢弃。我们所接受的标本实际上只是外科医生切除标本的其中一部分。因此,我常常观看术前术后的核磁片子,自己亲自看手术记录单,以核实手术标本的多少(是小标本还是大标本),核实术前和术后的核磁,了解他们取活检的部位。只有这样认真校对之后,才能考虑本例是否为WHO分类的弥漫性浸润性星形细胞瘤II 级。其实,中老年人的WHO分类的星形细胞瘤II 级远比星形细胞瘤级IV少见的多。
-
The immunostains clearly show many cells with strong nuclear immunoreactivity to antibodies against p53 and MIB-1 (Ki-67). These findings are diagnostic of an infiltrating fibrillary astrocytoma with low cellularity and, to the best I can tell from the photos, no readily identified mitoses. I am somewhat surprised to see so many positively stained cells in such low cellularity. This warns me to consider whether this is the edge of a high grade astrocytoma. The infiltrative borders of a high grade astrocytoma may look identical to the center of a WHO grade II astrocytoma. Therefore, grading of this tumor presented can be very tricky and depends on (1) how much tissue you have received for pathologic examination, and (2) pre- and post-surgical MRI findings. This needs to be carefully considered to avoid under-grading of a high grade astrocytoma.
If the specimen is from a stereotactic biopsy and small in amount, the interpreting pathologist has to try to determine whether the specimen represents the entire lesion found on MRI. The size, shape, anatomic location, multicentricity, heterogeneity of signal intensity, surrounding edema, and contrast enhancement on MRI are what radiologists look for in brain tumors. If MRI findings are consistent with a high grade tumor or glioblastoma, it would be wrong to grade this case as a WHO grade II fibrillary or diffuse infiltrating astrocytoma. This may happen when the surgeon biopsied the edge and not the center or worst area of the lesion.
From the gross description of this case, the specimen is probably from an open biopsy or subtotal resection. Sometimes, what we receive in the lab is not what the surgeons resect in the OR. A common scenario is that neurosurgeons send some tissue to pathology (with or without FS consultation request) they consider representative by their gross inspection. They will then continue to resect what they perceive as abnormal tissue, often with the help of CUSA (Cavitron Ultrasound Aspirator) that sucks soft abnormal tissue into a collector. These aspirated abnormal and normal tissue is admixed with foamy saline and blood, and often is difficult to harvest for adequate microscopic evaluation due to distortion. Some neurosurgeons don't even send this specimen to pathology and just discard it. In that case, what we receive in the lab is actually only a part of what surgeons resect. For these reasons, I almost always look at pre- and post-surgical MRI and read the operative note myself to be sure of the type of surgery (small biopsy vs resection), the pre-surgical MRI impression, and where the biopsy was on the post-surgical MRI. Only with this exercise would I be confident in diagnosing a WHO grade II diffuse infiltrating astrocytoma. After all, grade II astrocytomas are much less common than WHO grade IV glioblastomas in middle aged or elderly patients.
聞道有先後,術業有專攻
| 以下是引用mjma 在2006-11-18 0:09:00的发言: The immunostains clearly show many cells with strong nuclear immunoreactivity to antibodies against p53 and MIB-1 (Ki-67). These findings are diagnostic of an infiltrating fibrillary astrocytoma with low cellularity and, to the best I can tell from the photos, no readily identified mitoses. I am somewhat surprised to see so many positively stained cells in such low cellularity. This warns me to consider whether this is the edge of a high grade astrocytoma. The infiltrative borders of a high grade astrocytoma may look identical to the center of a WHO grade II astrocytoma. Therefore, grading of this tumor presented can be very tricky and depends on (1) how much tissue you have received for pathologic examination, and (2) pre- and post-surgical MRI findings. This needs to be carefully considered to avoid under-grading of a high grade astrocytoma. |
I agree with Dr. Ma's comment, this tissue dose like so called "CUSA" tissue, Some US pathologist rrefuses to read those cases. please show us some more photos if you have, otherwise, you may need to talk to your neurosurgeons. As a pathologist, educttion is a lifelong duty, sorry.











