















| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- 颞顶部肿瘤
-
zhongshihua 离线

- 帖子:1608
- 粉蓝豆:0
- 经验:1651
- 注册时间:2006-09-11
- 加关注 | 发消息
| 以下是引用xiaohl 在2006-11-2 0:13:00的发言:
这是一例富于细胞的肿瘤,主要由小到中等大的瘤细胞构成,血管丰富,可见血管周假菊形团和室管膜菊形团,散在或成片脂肪样细胞.细胞密度高,但异型性不明显,核分裂相罕见,无坏死. |
同意,但有个问题请教肖老师和各位老师,这个脂肪化生是何种细胞化生而来?脑组织内脂肪化生有何意义?小脑脂肪神经细胞瘤中脂肪成分实质是不是就是化生?谢谢!!

- 靠树有断,靠墙有塌,靠命有失 所以我只能自强不息!!!!!!
-
zhongshihua 离线
- 帖子:1608
- 粉蓝豆:0
- 经验:1651
- 注册时间:2006-09-11
- 加关注 | 发消息
-
This unusual tumor is listed as a "temporo-parietal" tumor. I wonder whether the tumor is associated with the ventricular wall or not. Also, can you let us know how frequent did you find mitoses? Is the tumor sharply circumscribed and demarcated from the surrounding parenchyma? Or is it infiltrative at the edge?
The neoplastic cells are relatively uniform in size between abundat small but somewhat hyalinized blood vessels with perivascular arrangement, formation of Flexner-Wintersteiner rosettes (Figures 9~12) (http://www.mrcophth.com/ophthalmologyhalloffame/wintersteiner.html), possible Homer Wright rosettes (Figures 5~8) and many vacuolated (probably lipidized) cells. Homer Wright rosettes and Flexner-Wintersteiner rosettes are both seen in PNET (retinoblastoma, pineoblastoma, esthesioneuroblastoma, medulloblastoma, neuroblastoma) ans some cases of better differentiated neuronal tumors. Flexner-Wintersteiner rosette is very similar to true ependymal rosette. Whether there are Homer Wright rosettes is important, for these structures indicate neuronal differentiation. The perivascular arrangement of neoplastic cells suggest pseudorosettes of ependymomas, but similar perivascular arrangement can be seen in papillary glioneuronal tumor and some cases of diffuse fibrillary astrocytomas and pilocytic astrocytomas. I am not entirely convinced that this is an ependymoma based on histoarchitecture and cytology of neoplastic cells.
Lipidized cells can be seen in only a few types of primary CNS tumors - (1) cerebellar and, very rarely, supratentorial (http://www.dustri.com/ze/np/samplecopy/march06/np02086.pdf) liponeurocytomas, (2) ependymomas, (3) meningiomas, and (4) glioblastomas/gliosarcomas. I am not sure how mitotically active the neoplastic cells are. I have not seen dysplastic neurons or large ganglion cells to lend support for a neuronal/neurocytic tumor. With no easily identified mitosis or anaplastic features on the uploaded photos, I suspect this case is still a well to moderately differentiated neuronal (neurocytic) neoplasm. If it is associated with the lateral ventricular wall, it would invite the diagnosis of rare supratentorial liponeurocytoma. In my personal opinion, liponeurocytoma is rare and can potentially occur at any location in the CNS.
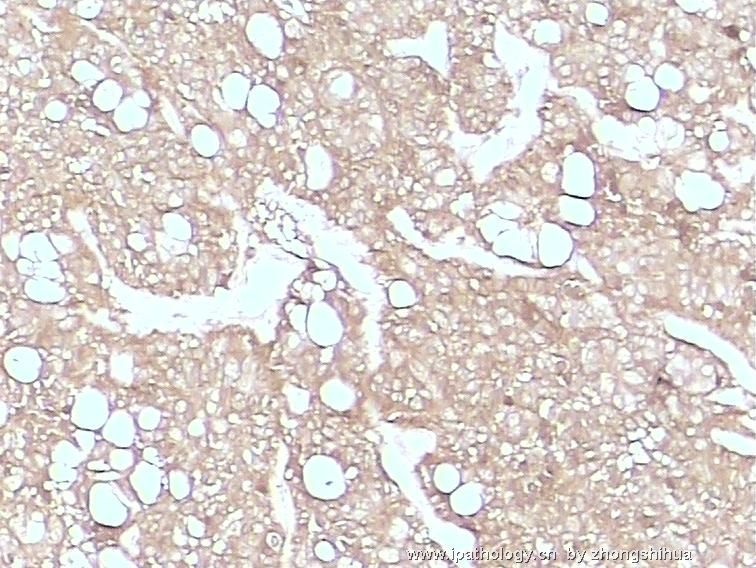
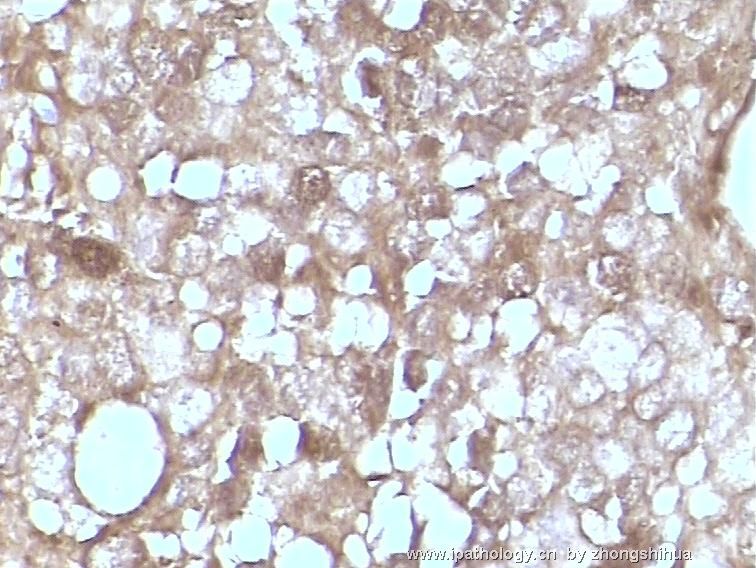
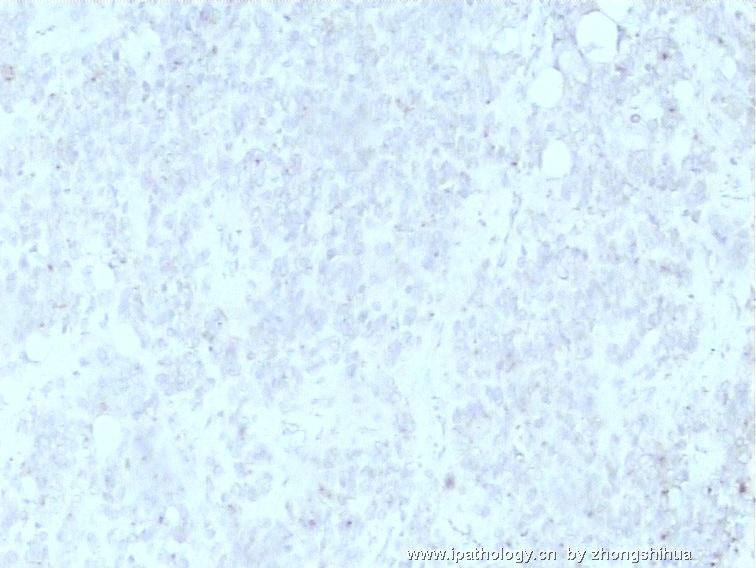
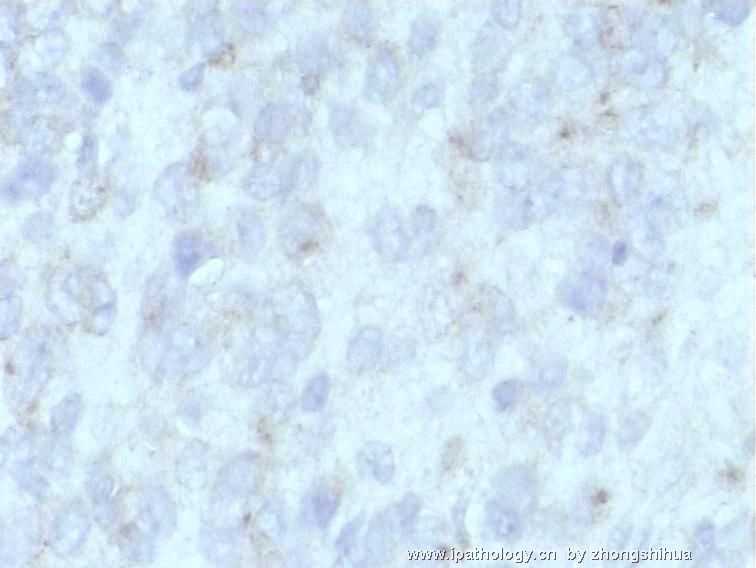
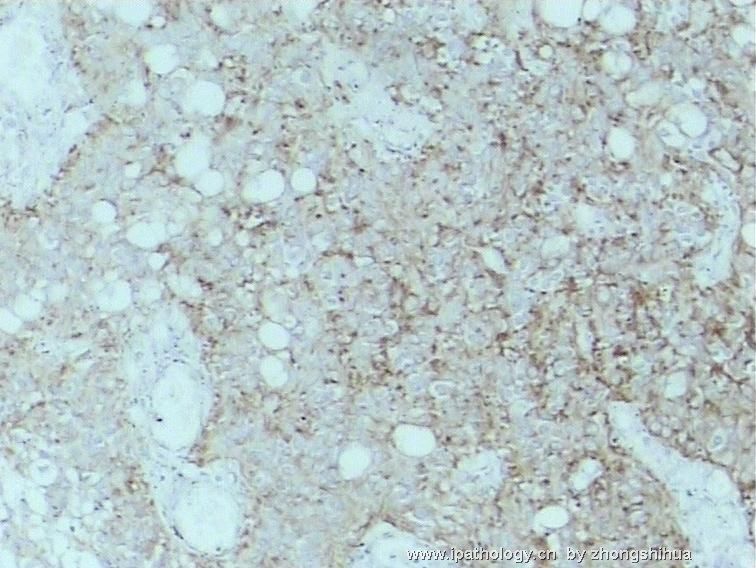
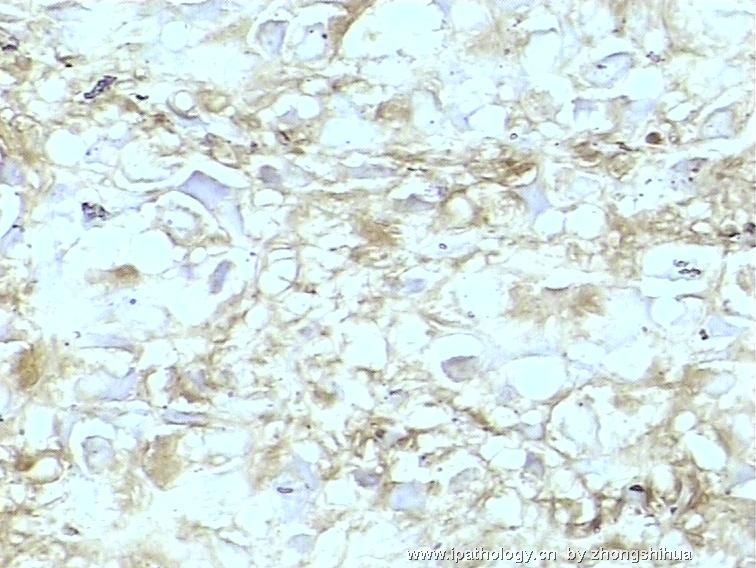
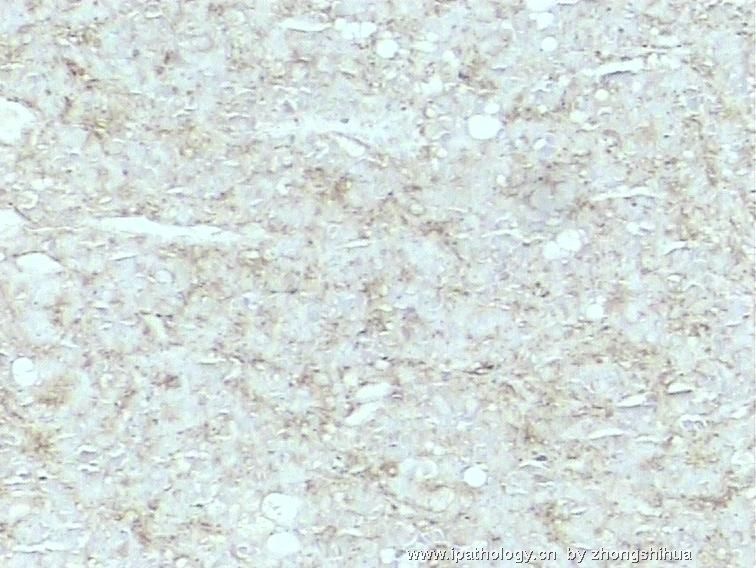
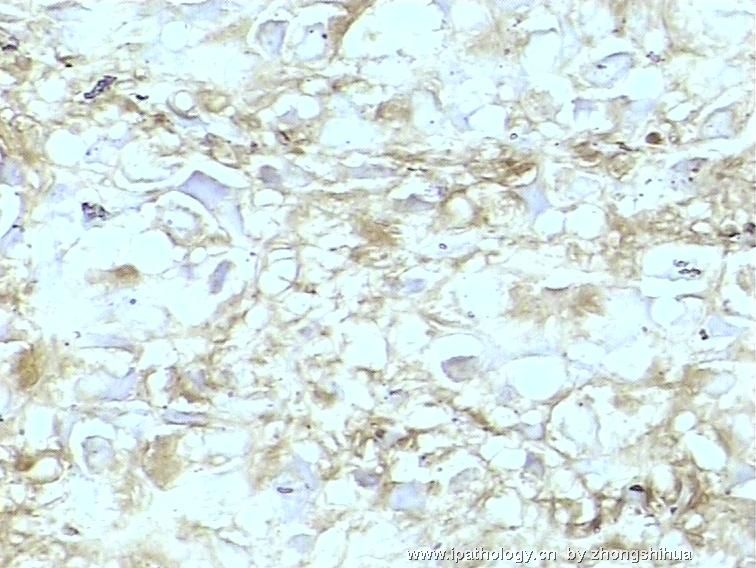
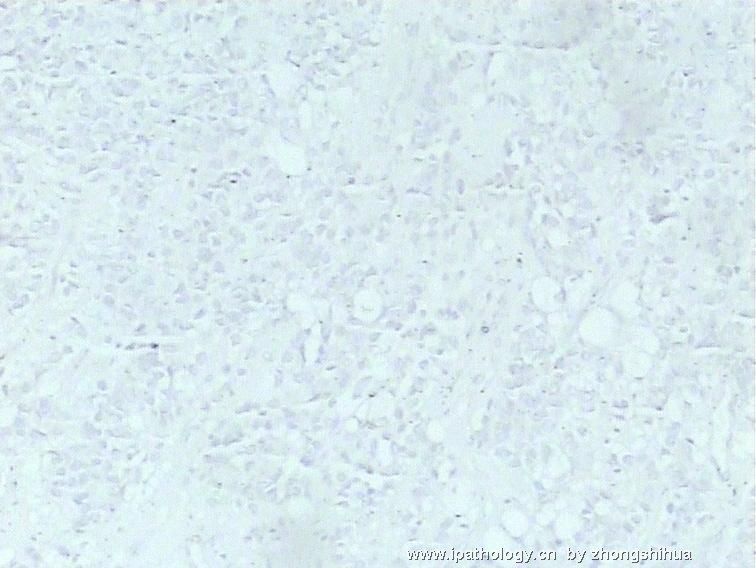
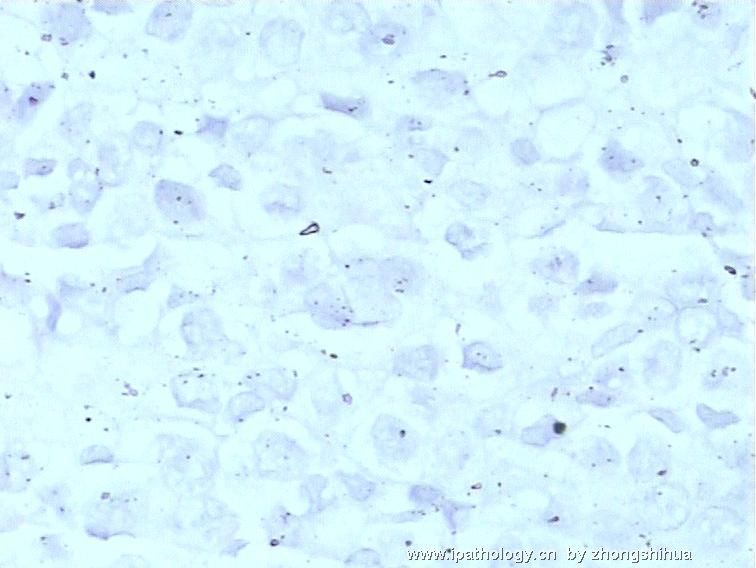
I do believe immunohistochemistry would help characterize this enigmatic neoplasm further. I would employ the following antibodies and see what is found - GFAP, EMA, synaptophysin, NSE, and MIB-1 (Ki67). I look forward to seeing photos of your immunostains.
聞道有先後,術業有專攻
-
zhongshihua 离线
- 帖子:1608
- 粉蓝豆:0
- 经验:1651
- 注册时间:2006-09-11
- 加关注 | 发消息
-
zhongshihua 离线
- 帖子:1608
- 粉蓝豆:0
- 经验:1651
- 注册时间:2006-09-11
- 加关注 | 发消息
-
本帖最后由 于 2006-11-16 22:31:00 编辑
马老师,您好!我是病理新手,为了学习,我翻译你的帖子,不当之处请不吝赐教。
这例罕见肿瘤的标题称为“颞顶部肿瘤”。我想知道肿瘤是否与脑室壁有关。并且能否告知核分裂率有多少?肿瘤是否局限,边界是否清晰,还是呈浸润性边界?
这例罕见肿瘤的标题称为“颞顶部肿瘤”。我想知道肿瘤是否与脑室壁有关。并且能否告知核分裂率有多少?肿瘤是否局限,边界是否清晰,还是呈浸润性边界?
肿瘤细胞的大小相对一致,分布于丰富的小而略呈透明化的血管之间,呈血管周排列,形成Homer Wright菊形团(图9-12)、可能Flexner-Wintersteiner菊形团。以及许多空泡细胞(可能是脂肪化)。Homer Wright菊形团和Flexner-Wintersteiner菊形团均可见于PNET(视网膜母细胞瘤、松果体母细胞瘤、感觉神经母细胞瘤即嗅神经母细胞瘤、神经母细胞瘤)以及某些分化较好的神经肿瘤。Flexner-Wintersteiner菊形团和真正的室管膜菊形团非常相似。有无Homer Wright菊形团是很重要的,因为这些结构提示神经元的分化。肿瘤细胞呈血管周排列提示室管膜瘤的假菊形团,但相似的血管周排列也可见于:乳头状胶质神经元肿瘤、某些弥漫性纤维型星形细胞瘤、以及毛细胞型星形细胞瘤。根据肿瘤细胞的组织结构和细胞学,我尚不能确信这就是室管膜瘤。
脂肪化的细胞仅见于少数几种原发性CNS肿瘤,如:(1)发生于小脑和极少发生于小脑幕上的脂肪神经细胞瘤,(2)室管膜瘤,(3)脑膜瘤,(4)胶质母细胞瘤/胶质肉瘤。我不能确定肿瘤细胞的核分裂活性。未见异型神经元或大的神经节细胞以支持神经元/神经细胞肿瘤的诊断。上传图片中没有容易辨别的核分裂和间变性,我怀疑这仍然是一例高~中分化的神经元/神经细胞肿瘤。如果与脑室侧壁有关,则可能会考虑罕见的小脑幕上的脂肪神经细胞瘤。我个人认为,神经胶质细胞瘤虽然很少发生,但能潜在地发生在中枢神经系统的任何地方。
我相信免疫组化能帮助我们进一步解开这个肿瘤的谜团。我会选择GFAP、 EMA、SYN、NSE、MIB-1 (Ki67)的免疫组化,看有何发现。.我期待见到免疫组化图片。 - 华夏病理群1:35164959(已满);华夏病理群2:40555921(已满);华夏病理群3:38905768(已满);华夏病理群4:64603316(请进)
-
zhongshihua 离线
- 帖子:1608
- 粉蓝豆:0
- 经验:1651
- 注册时间:2006-09-11
- 加关注 | 发消息











