
| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- Lymphadenopathy
-
panzenggang 离线
- 帖子:189
- 粉蓝豆:480
- 经验:246
- 注册时间:2008-01-09
- 加关注 | 发消息
| 姓 名: | ××× | 性别: | Female | 年龄: | 33 |
| 标本名称: | Lymph node | ||||
| 简要病史: | A 33 years old female was diagnosed with Hodgkin lymphoma 3 years ago at an outside hospital, and no outside slides were available for review. Recently she presented with abdominal pain due to umbilical hernia, and image studies revealed a periportal lymph node of 3.9 cm. The lymph node was excised. | ||||
| 肉眼检查: | |||||

名称:图1
描述:图1

名称:图2
描述:图2

名称:图3
描述:图3

名称:图4
描述:图4

名称:图5
描述:图5

名称:图6
描述:图6

名称:图7
描述:图7

名称:图8
描述:图8

名称:图9
描述:图9

名称:图10
描述:图10
标签:
×参考诊断
T-Cell/Histiocyte-Rich Large B-Cell Lymphoma
-
panzenggang 离线
- 帖子:189
- 粉蓝豆:480
- 经验:246
- 注册时间:2008-01-09
- 加关注 | 发消息
- A variant of DLBCL with prominent CD8+ T cells and histiocytes
- M:F=2:1, 60-70 years of age
- Mostly in lymph node, but more frequently presents with high-stage disease (about two thirds in stage III-IV) in bone marrow and spleen, compared with conventional DLBCL
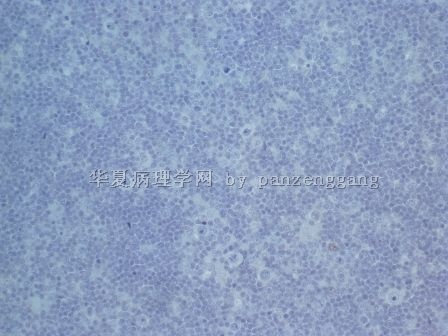
- Diffuse effacement of lymph node with polymorphic cellular population, lack of nodular pattern or sclerosis
- Scattered large tumor cells, <10% of the cellular population, dispersed singly, without the formation of discrete aggregates or sheets
- Morphology of tumor cells: centroblasts, immunoblasts, pleomorphic, LP (or L&H) cells, or Reed-Sternberg cells
- Background: small lymphocytes with mostly CD3+CD8+ T cells; variable numbers of histiocytes; scant plasma cells or eosinophils
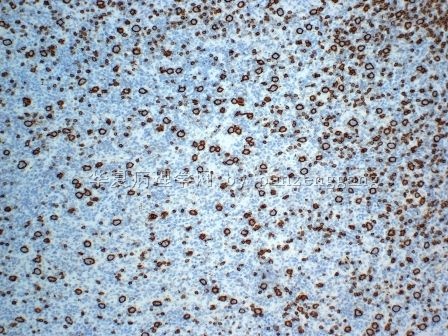
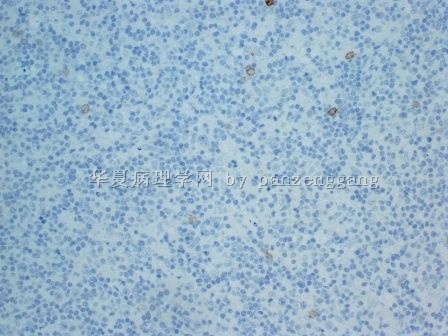
- Tumor cells: pan-B+, CD30−, CD15−, EMA+/−, BCL6+/−
- Background lymphocytes: CD3+, CD8+
- Background histiocytes: CD68+
- Lack of large CD21+ meshwork as seen in NLPHD
- Background lymphocytes: CD3+, CD8+
- Background histiocytes: CD68+
- Lack of large CD21+ meshwork as seen in NLPHD
- WHO Pathology & Genetics. Tumours of Haematopoietic and Lymphoid Tissues. IARC Press, Lyon 2008
- Hematopathology Clinical Pathologic Guidelines. Hematopathology section, University of New Mexico
- Hematopathology. Elaine Sarkin Jaffe, MD, Nancy L. Harris, MD, James Vardiman, MD, Elias Campo, MD, and Daniel Arber, MD. 2010
Final diagnosis: T-Cell/Histiocyte-Rich Large B-Cell Lymphoma
http://enjoypath.com/hp/hp-145.htm
| T-Cell/Histiocyte-Rich Large B-Cell Lymphoma | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CLINICAL FEATURES | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| MICROSCOPIC FINDINGS | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DIFFERENTIAL DIAGNOSES | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IMMUNOHISTOCHEMISTRY AND SPECIAL STAINS | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| REFERENCES | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
-
panzenggang 离线
- 帖子:189
- 粉蓝豆:480
- 经验:246
- 注册时间:2008-01-09
- 加关注 | 发消息
-
panzenggang 离线
- 帖子:189
- 粉蓝豆:480
- 经验:246
- 注册时间:2008-01-09
- 加关注 | 发消息
The background of HL usually contains lymphocytes, eosinophils and plasma cells. However, rare eosinophils and plasma cells are present in this cases.
The classic HL cells have abundant cytoplasm with large eosinophilic nucleoli,. The tumor cells in this case show a mixed morphologic features, including centroblastic, immunoblastic, and HL-like.
Hint: what other cells are present in the background in addition to lymphocytes?











